Tell me 5 common heart disease with their ECG changes, and also give me ecg pics.
Reading File
Finding Sources
Finding Sources
Searching Images
ECG ST elevation myocardial infarction STEMI
Searching Images
atrial fibrillation ECG electrocardiogram
Finding Sources
Finding Sources
Finding Sources
Searching Images
complete heart block AV block third degree ECG
Searching Images
left ventricular hypertrophy ECG voltage criteria
Searching Images
heart failure ECG changes cardiomegaly
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
I have excellent ECG images for all 5 conditions. Now I'll compile a comprehensive response.
5 Common Heart Diseases & Their ECG Changes
1. 🫀 ST-Elevation Myocardial Infarction (STEMI)
ECG Changes
| Feature | Finding |
|---|---|
| ST segments | Convex (tombstone) elevation ≥1 mm in ≥2 contiguous leads |
| Reciprocal changes | ST depression in leads opposite the infarct zone |
| Hyperacute T-waves | Tall, peaked T-waves in the earliest phase |
| Pathological Q waves | Develop within hours–days (marker of necrosis) |
| QRS changes | R-wave loss / QS pattern in infarcted territory |
Localisation:
- Anterior (V2–V4): LAD occlusion
- Inferior (II, III, aVF): RCA occlusion
- Lateral (I, aVL, V5–V6): LCx occlusion
As described in Harrison's Principles of Internal Medicine 22E: "Profound ST elevation or depression in multiple leads usually indicates very severe ischemia. The division of acute myocardial infarction due to obstructive coronary artery disease into ST-segment elevation and non-ST elevation types is useful since the consistent efficacy [of reperfusion] differs."
ECG Image — Anterior STEMI

12-lead ECG: Acute anterior STEMI. Prominent convex ST elevation is visible across V2–V6. Reciprocal ST depression is present in the inferior leads (II, III, aVF). The QRS complexes show evolving QS pattern in V2–V3, confirming transmural injury.
2. 🫀 Atrial Fibrillation (AF)
ECG Changes
| Feature | Finding |
|---|---|
| P waves | Absent — replaced by chaotic fibrillatory (f) waves (best seen in V1, II) |
| Rhythm | Irregularly irregular R-R intervals (hallmark) |
| Ventricular rate | Variable; 100–160 bpm if uncontrolled |
| QRS morphology | Narrow (normal conduction), unless aberrancy or pre-excitation |
| Baseline | Fine undulating fibrillatory waves, not organized atrial activity |
Tintinalli's Emergency Medicine states: "The ECG hallmarks of atrial fibrillation include the absence of discernible P waves and an irregularly irregular ventricular rhythm. With the chaotic atrial activity, distinct P waves are not noted; rather, either a flat baseline or fine chaotic fibrillatory waves are present."
ECG Image — Atrial Fibrillation with Rapid Ventricular Response

12-lead ECG: Atrial fibrillation with rapid ventricular response. No organized P waves are visible; fine fibrillatory waves replace them. The R-R intervals are completely irregular across all leads. QRS complexes are narrow, confirming supraventricular origin.
3. 🫀 Complete (Third-Degree) AV Heart Block
ECG Changes
| Feature | Finding |
|---|---|
| P waves | Present, regular, at normal atrial rate (~60–100 bpm) |
| QRS complexes | Present, regular, at slow escape rate (20–60 bpm) |
| PR interval | Completely variable — no fixed relationship between P and QRS |
| AV dissociation | P waves "march through" QRS complexes independently |
| QRS width | Narrow if junctional escape; wide (>120 ms) if ventricular escape |
The Washington Manual of Medical Therapeutics classifies AV blocks into: 1st degree, 2nd degree (Mobitz I/Wenckebach and Mobitz II), and 3rd degree (complete). Complete heart block carries risk of drop attacks (Stokes-Adams attacks) and is an indication for permanent pacemaker.
ECG Image — Complete (3rd Degree) AV Block

12-lead ECG: Complete (3rd degree) AV block. Total AV dissociation is present — P waves fire at a faster independent atrial rate while wide QRS complexes occur at a slow ventricular escape rate (~35 bpm). There is no consistent PR interval. Wide QRS indicates an infra-nodal escape focus.
4. 🫀 Left Ventricular Hypertrophy (LVH)
LVH is caused by longstanding hypertension, aortic stenosis, or hypertrophic cardiomyopathy.
ECG Changes
| Feature | Finding |
|---|---|
| Sokolow-Lyon criteria | SV1 + RV5 or RV6 ≥ 35 mm |
| Cornell criteria | RaVL + SV3 > 28 mm (men), >20 mm (women) |
| R in aVL | ≥ 12 mm alone suggests LVH |
| Strain pattern | ST depression + T-wave inversion in I, aVL, V4–V6 (lateral leads) |
| Left axis deviation | Common |
| P mitrale | Notched, broad P wave in II if LA enlargement coexists |
Harrison's notes: "The sensitivities of conventional voltage criteria for left ventricular hypertrophy are low in middle-age to older adults and may be decreased further in obese persons and smokers, as well as with right bundle branch block."
ECG Image — Left Ventricular Hypertrophy with Strain
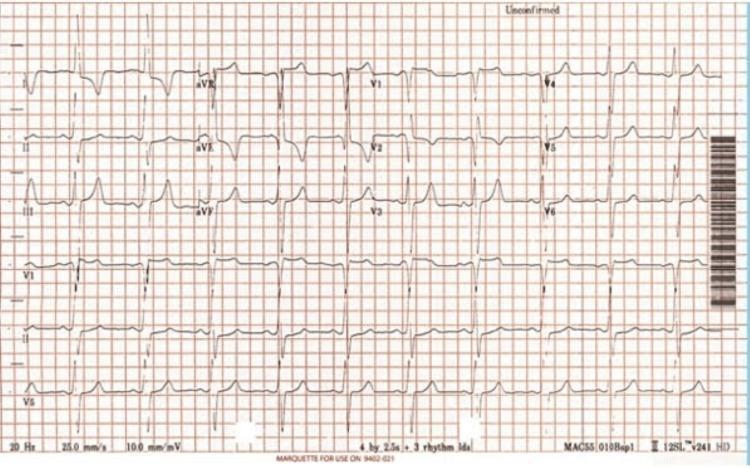
12-lead ECG: Left ventricular hypertrophy meeting Cornell voltage criteria (tall R in aVL + deep S in V3). Prominent T-wave inversions in V4–V6, I, and aVL represent the classic LVH "strain pattern," indicating secondary repolarization abnormality from severe hypertrophy.
5. 🫀 Heart Failure with Reduced Ejection Fraction (HFrEF) / Dilated Cardiomyopathy
Heart failure does not have a single pathognomonic ECG pattern, but several findings are characteristic:
ECG Changes
| Feature | Finding |
|---|---|
| Left bundle branch block (LBBB) | Wide QRS >120 ms, broad notched R in I/aVL/V5–V6, deep S in V1 — seen in up to 25% of HFrEF |
| Poor R-wave progression | Loss of R-wave height V1→V4, suggesting anterior wall disease or dilation |
| Sinus tachycardia | Compensatory increase in HR |
| Atrial fibrillation | Common comorbid arrhythmia |
| QRS prolongation | Marker of dyssynchrony; target of CRT therapy if ≥150 ms |
| Non-specific ST-T changes | ST depression, T-wave inversions |
| LVH pattern | When due to hypertensive cardiomyopathy |
Goldman-Cecil Medicine states: "Patients with heart failure and a reduced ejection fraction have substantial prolongation of the QRS duration on the surface electrocardiogram, which is a marker of abnormal electrical activation of the left ventricle" — the rationale for cardiac resynchronization therapy (CRT).
ECG Image — Heart Failure / Dilated Cardiomyopathy with LBBB
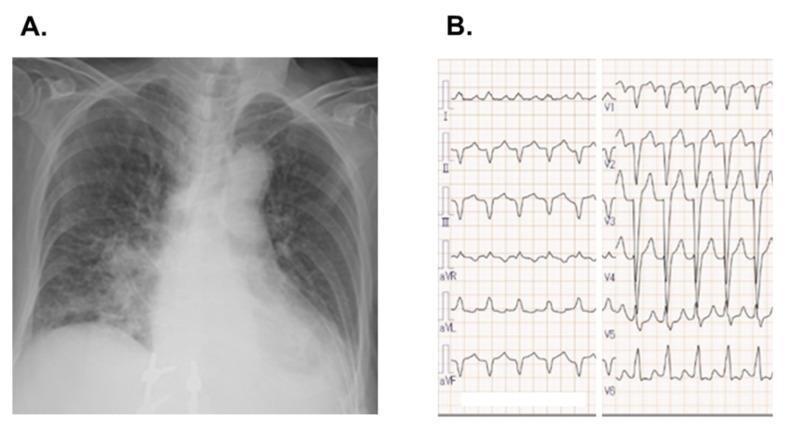
Chest X-ray (A) + 12-lead ECG (B): Cardiomegaly with bilateral pulmonary congestion on CXR. The ECG shows a complete LBBB pattern — wide QRS complexes with broad notched R waves in lateral leads and deep S waves in V1. Poor R-wave progression across V1–V4 is consistent with dilated cardiomyopathy.
Quick Summary Table
| # | Disease | Key ECG Finding |
|---|---|---|
| 1 | STEMI | ST elevation ≥1 mm in ≥2 contiguous leads + reciprocal depression |
| 2 | Atrial Fibrillation | No P waves + irregularly irregular RR intervals |
| 3 | Complete AV Block | AV dissociation: P waves & QRS independent, slow escape rhythm |
| 4 | Left Ventricular Hypertrophy | High voltage (Sokolow/Cornell) + lateral strain pattern |
| 5 | Heart Failure / DCM | LBBB, QRS prolongation, poor R-wave progression, ST-T changes |
Sources: Harrison's Principles of Internal Medicine 22E; Tintinalli's Emergency Medicine; Goldman-Cecil Medicine; The Washington Manual of Medical Therapeutics; Guyton & Hall Textbook of Medical Physiology.
This is a shared conversation. Sign in to Orris to start your own chat.