Spondylolisthesis 10 marks ms orthopaedics
spondylolisthesis classification Meyerding grades management MS orthopaedics
spondylolisthesis Meyerding grading classification spine
Spondylolisthesis — MS Orthopaedics (10 Marks)
Definition
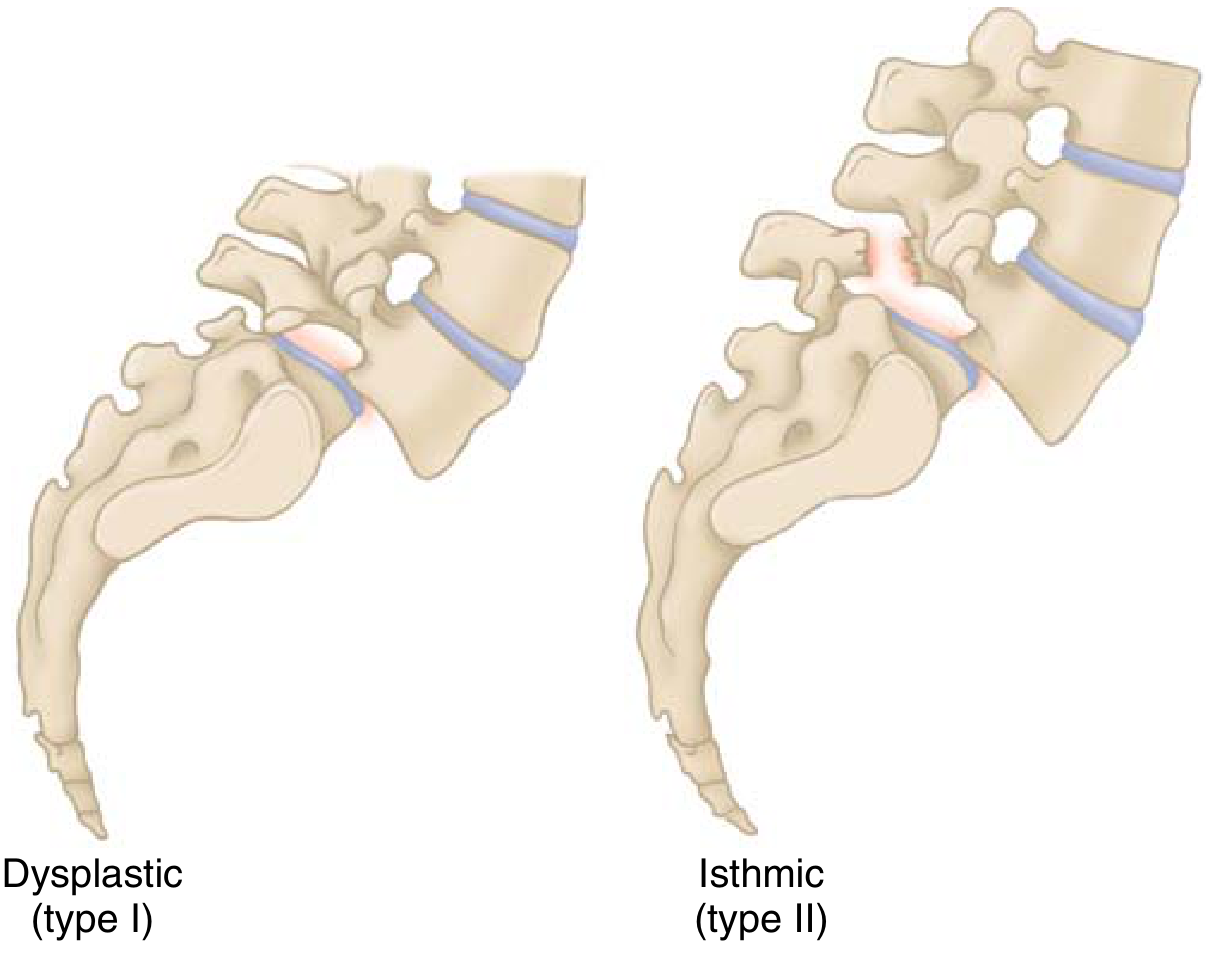
Classification — Wiltse, Newman & McNab (6 Types)
| Type | Age | Pathology |
|---|---|---|
| I — Dysplastic | Child | Congenital dysplasia of S1 superior facet; neural arch intact → high risk of cauda equina |
| II — Isthmic (most common) | 5–50 yrs | Pars interarticularis defect (fatigue fracture/elongation); typically L5–S1 |
| III — Degenerative | >40 yrs | Facet arthrosis → subluxation without pars defect; typically L4–L5; commoner in women |
| IV — Traumatic | Any age | Acute fracture of elements other than pars |
| V — Pathologic | Any age | Bone incompetence (Paget's, tumour, osteoporosis) |
| VI — Postsurgical | Adult | Excessive resection of neural arch/facets |
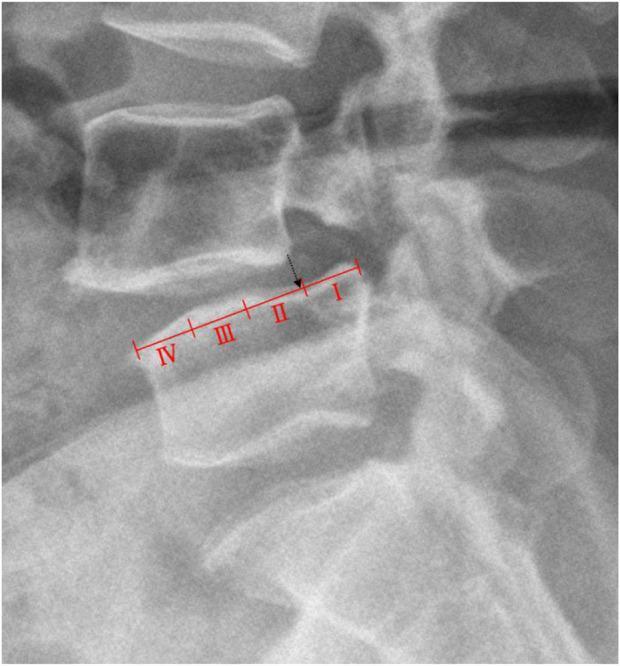
Grading — Meyerding Classification
| Grade | % Slip |
|---|---|
| I | 0–25% |
| II | 26–50% |
| III | 51–75% |
| IV | 76–100% |
| V | >100% (Spondyloptosis — complete fall-off) |
- Slip angle (normally <0°, i.e., lordotic at L5–S1 disc) — quantifies kyphosis at the slip level
- Sacral inclination (normally >30°)
- Pelvic incidence (PI) (normally ~50°) — predicts intervention and prognosis
Epidemiology & Natural History
- Prevalence ~4–6% in the general population
- Isthmic type: most common in White males, gymnasts, football linemen (repetitive hyperextension stress)
- Degenerative type: most common in women >40 years at L4–L5
- Most common symptomatic level: L5–S1 (isthmic); L4–L5 (degenerative)
- Unilateral pars defects rarely progress to slip
- Slip progression slows in adulthood; degeneration of the disc → foraminal stenosis → L5 root compression
Clinical Features
Symptoms
- Low back pain — most common; worse on extension; relieved by flexion
- Radicular pain — L5 root (isthmic, foraminal compression); bilateral L5 (high-grade)
- Neurogenic claudication — in degenerative type with canal stenosis
- Cauda equina syndrome — bladder/bowel dysfunction; rare but emergency
Signs
- Palpable step-off deformity at lumbosacral junction
- Flattening of lumbar lordosis
- "Pelvic waddle" gait in severe cases
- Hamstring tightness (reflex protective spasm — a hallmark in children/adolescents)
- "Heart-shaped" buttocks — in high-grade slips due to posterior displacement of sacrum
- Restriction of lumbar flexion/extension
- Neurological deficit: weakness of EHL (L5), reduced ankle reflex (S1)
Investigations
Radiography (Plain X-ray) — Primary Investigation
- Lateral view: best to visualize slip, Meyerding grading, slip angle
- AP view: inverted Napoleon's hat sign (Grade IV–V)
- Oblique view (45°): shows the "Scotty dog" sign; a collar/break around the neck = pars defect (spondylolysis)
- 80% of pars lesions visible on lateral; 15% additional on oblique
Other Imaging
| Modality | Use |
|---|---|
| CT scan | Best for bony detail; pars defect morphology |
| MRI | Neural compression, disc degeneration, Gill nodule (fibrocartilaginous repair tissue), bony oedema (stress reaction) |
| SPECT | Increased uptake = acute/healing lesion; guides conservative treatment prognosis |
| Bone scan | Rarely needed; SPECT preferred |
Treatment
Conservative (Non-operative)
- Activity modification (avoid hyperextension sports — gymnastics, football)
- Flexion exercises (Williams' exercises); core strengthening
- NSAIDs for pain
- Bracing (thoracolumbosacral orthosis) — especially in adolescents with acute pars stress reaction
- Epidural steroid injections for radicular symptoms
- Adolescents with Grade I may return to contact sports once asymptomatic
- Grade II asymptomatic → restricted from gymnastics and football; regular radiological follow-up
Indications for Surgery
- Progressive slip (especially in skeletally immature patients)
- Neurological deficit (motor weakness, cauda equina syndrome)
- High-grade slip (Grades III–IV)
- Intractable pain failing ≥6 months conservative management
- Cosmetically unacceptable deformity
Surgical Options
Low-Grade Slips (Grades I–II)
- Posterolateral fusion in situ — procedure of choice; L4–S1 fusion with pedicle screw instrumentation
- If neural compression present → decompression + fusion (posterior lumbar interbody fusion/PLIF or TLIF)
- Gill's procedure (excision of loose Gill fragment/fibrocartilaginous mass at pars) alone is not recommended as it increases instability; must be combined with fusion
High-Grade Slips (Grades III–IV)
- Reduction + instrumented fusion vs in-situ fusion — controversial
- Reduction risks: L5 root neurapraxia (traction injury) — must be done slowly with wake-up tests or neurophysiological monitoring
- Circumferential fusion (anterior + posterior) often required for high-grade slips
- Spondyloptosis (Grade V): partial reduction followed by fusion
Degenerative Spondylolisthesis
- Decompression (laminectomy/laminotomy) alone is inadequate if there is instability
- Decompression + posterolateral fusion ± pedicle screws (instrumented fusion gives better outcomes)
Complications
| Complication | Notes |
|---|---|
| Neurological injury during surgery | L5 neurapraxia (reduction of high-grade) |
| Pseudarthrosis | Failed fusion; requires revision |
| Adjacent segment disease | Degeneration at levels adjacent to fusion |
| Cauda equina syndrome | Emergency if progressive |
| Slip progression | Monitor with serial X-rays in children |
Key Points for Exam (Scoring Points)
- Definition: Forward slip of one vertebra on another
- Wiltse classification — 6 types; isthmic most common
- Meyerding grading — 5 grades; Grades I–II = low-grade, III–IV = high-grade, V = spondyloptosis
- Scotty dog sign on oblique X-ray — pars defect (spondylolysis)
- Clinical hallmarks: palpable step-off, hamstring tightness, pelvic waddle, heart-shaped buttocks
- Radiological measurements: slip %, slip angle, sacral inclination, pelvic incidence
- Conservative treatment for low-grade, asymptomatic or mildly symptomatic
- Fusion in situ for low-grade surgical cases; decompression added if neural compromise
- High-grade: in-situ vs. reduction-and-fusion debate; neurological risk of L5 neurapraxia
- Degenerative type: decompression + fusion; decompression alone → higher recurrence
Cervical spondylolisthesis
cervical spondylolisthesis classification clinical features management orthopaedics
https://pmc.ncbi.nlm.nih.gov/articles/PMC3103955
degenerative cervical spondylolisthesis
cervical spondylolisthesis degenerative MRI X-ray
Cervical Spondylolisthesis
Definition
- Traumatic cervical spondylolisthesis — most notably Hangman's fracture (traumatic spondylolisthesis of C2)
- Degenerative cervical spondylolisthesis — slip secondary to disc and facet degeneration, most common in the subaxial spine (C3–C5)
Types / Classification
A. Traumatic Cervical Spondylolisthesis
1. Hangman's Fracture (Traumatic Spondylolisthesis of the Axis — C2)
| Type | Displacement | Angulation | Disc C2–C3 | Stability |
|---|---|---|---|---|
| I | <3 mm | <11° | Intact | Stable |
| II | >3 mm | >11° | Disrupted | Unstable |
| IIa | Minimal | Severe (>11°) | Disrupted | Most unstable — do NOT apply traction |
| III | >3 mm + facet dislocation | Severe | Disrupted | Most severe |

2. Subaxial Traumatic Spondylolisthesis (C3–C7)
- Unilateral facet dislocation: ~25% anterior slip, rotational deformity
- Bilateral facet dislocation (perched facets): ≥50% anterior slip; high risk of cord injury
- Teardrop fracture-dislocation: hyperflexion; severe cord injury common
B. Degenerative Cervical Spondylolisthesis
Dean et al. Classification (2 types):
- Type I (Adjacent type) — more common; slip occurs adjacent to a relatively stiff, spondylotic cervical segment (the mobile segment next to the stiff one bears excess load)
- Type II (Spondylotic type) — slip occurs within the spondylotic segment itself
Woiciechowsky et al. Classification (3 types):
- Type 1: Spondylolisthesis with facet joint degeneration only
- Type 2: Spondylolisthesis with degeneration of facet joints AND vertebral bodies/discs
- Type 3: Spondylolisthesis with severe cervical spine deformity
Epidemiology
- Degenerative cervical spondylolisthesis: most common at C3/4 (46%) and C4/5 (49%)
- Prevalence in the general population: lower than lumbar; often underdiagnosed
- More common in elderly; no clear gender predisposition in degenerative type
- 46% of patients demonstrate segmental instability on flexion-extension radiographs
Pathophysiology
Degenerative Type
- Disc degeneration → disc space narrowing → increased load transfer to facet joints
- Facet arthropathy → capsular laxity → segmental instability
- Forward slip of the superior vertebra → dynamic or fixed spondylolisthesis
- Secondary changes: osteophyte formation, ligamentum flavum hypertrophy, uncovertebral joint hypertrophy → canal and foraminal stenosis
- Spinal cord compression → myelopathy; foraminal compression → radiculopathy
Clinical Features
1. Traumatic Cervical Spondylolisthesis
- History of high-energy trauma (MVA, fall from height, diving)
- Neck pain, restricted movement
- Variable neurology: may be neurologically intact (Hangman's) or have complete cord injury (bilateral facet dislocation)
- Signs of cord injury: spastic quadriparesis, sensory level, bladder/bowel dysfunction
- Diaphragm sparing: C3/C4 injuries may spare breathing if partial
2. Degenerative Cervical Spondylolisthesis
| Symptom | Frequency |
|---|---|
| Neck/occipital pain | 51% |
| Myelopathy or myeloradiculopathy | 64% |
| Radiculopathy alone | 22% |
- Upper limbs: Weakness and wasting of hand intrinsics (C8/T1); clumsy hands; loss of fine motor dexterity
- Lower limbs: Spastic paraparesis, scissor gait, wide-based gait; Babinski sign positive
- Lhermitte's sign: Electric shock sensation down spine on neck flexion
- Hoffman's sign: Positive (flicking middle finger → thumb flexion)
- Hyperreflexia below the level; hyporeflexia/LMN signs at the level
- Inverted radial reflex: Pathognomonic of C5/6 cord lesion
- Numbness and paresthesias in hands (often earliest symptom)
| Level | Pain | Sensory | Weakness | Reflex lost |
|---|---|---|---|---|
| C4/5 | Neck → shoulder | Lateral arm | Deltoid, spinati | — |
| C5/6 | Neck → lateral forearm, thumb | Thumb, index | Biceps, wrist extensors | Biceps, brachioradialis |
| C6/7 | Neck → middle finger | Middle finger | Triceps, wrist flexors | Triceps |
| C7/T1 | Neck → ring/little finger | Medial forearm | Hand intrinsics | — |
Investigations
Radiography
- Lateral X-ray: Best for alignment; anterior slip, disc height loss, osteophytes
- Flexion-extension views: Essential for demonstrating dynamic instability; >3.5 mm translation or >11° angulation = instability (White & Panjabi criteria)
- CT scan (with sagittal reconstruction): Bone detail, fracture characterization, facet morphology
- CTMM (CT myelogram): When MRI contraindicated
- Anterior vertebral slip (Grade I most common)
- Disc space narrowing
- Osteophyte formation
- Facet hypertrophy
- Loss of cervical lordosis or focal kyphosis
MRI — Investigation of Choice for Neural Compression
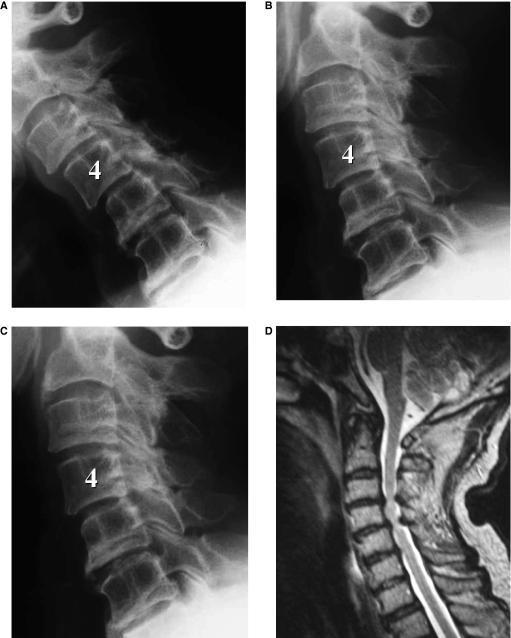
- Degree of canal compromise
- Cord signal changes (T2 hyperintensity = myelomalacia — poor prognostic sign)
- Disc degeneration, ligamentum flavum hypertrophy
- Neural foraminal stenosis
EMG/NCS
- Differentiates radiculopathy from peripheral neuropathy
- Identifies level of root compression
Treatment
Conservative Management
- Cervical collar/immobilisation (Philadelphia collar for Hangman's Type I–II)
- Halo vest: for Hangman's Type II, displaced injuries requiring reduction and immobilisation
- NSAIDs, analgesics
- Cervical traction (Gardner-Wells tongs) for closed reduction of facet dislocations — contraindicated in Type IIa Hangman's (risk of distraction injury)
- Physiotherapy: cervical stabilisation exercises, traction, heat
- Epidural steroid injections for radiculopathy
Surgical Management
- Myelopathy (progressive or severe)
- Radiologically proven instability (>3.5 mm slip or >11° angulation)
- Neurological deficit (radiculopathy with objective motor weakness)
- Failed conservative management (>6–12 weeks)
- Hangman's Types II, IIa, III — unstable injuries
- Spinal cord compression with signal change on MRI
For Degenerative Spondylolisthesis
| Approach | Procedure | Indication |
|---|---|---|
| Anterior | ACDF (Anterior Cervical Discectomy & Fusion) | 1–2 level disease; restores height, decompresses, fuses |
| Anterior | Corpectomy + fusion | Multilevel disease; significant spondylosis |
| Posterior | Laminectomy | Multilevel stenosis without instability (rarely alone) |
| Posterior | Laminoplasty | Multilevel cord compression (preserves motion) |
| Posterior | Laminectomy + lateral mass fusion | Multilevel with instability; prevents post-laminectomy kyphosis |
| Combined | 360° fusion | Severe deformity, kyphosis, high-grade instability |
For Traumatic Spondylolisthesis
| Fracture Type | Treatment |
|---|---|
| Hangman's Type I | Hard collar 12 weeks |
| Hangman's Type II | Halo vest or anterior C2–C3 ACDF |
| Hangman's Type IIa | Halo vest with extension (NOT traction); anterior ACDF |
| Hangman's Type III | Posterior stabilisation (C1–C3 fusion) |
| Bilateral facet dislocation | Closed reduction under traction + posterior fusion |
| Unilateral facet dislocation | Anterior or posterior fusion depending on disc status |
Key Differences from Lumbar Spondylolisthesis
| Feature | Cervical | Lumbar |
|---|---|---|
| Most common cause | Degenerative / traumatic | Isthmic / degenerative |
| Common level | C3/4, C4/5 | L4/5, L5/S1 |
| Neural complication | Myelopathy (cord) | Radiculopathy / cauda equina |
| Emergency | Cord compression/myelopathy | Cauda equina syndrome |
| Pars defect | Rare | Hallmark of isthmic type |
| Meyerding grading | Less commonly applied | Standard grading system |
| Investigation of choice | MRI cervical spine | MRI lumbar spine |
| Flexion-extension films | Critical (dynamic instability) | Useful but less critical |
| Main surgery | ACDF | Posterolateral fusion ± decompression |
Summary — Points for Exam
- Traumatic: Hangman's fracture (C2) — hyperextension; Levine-Edwards 4 types; often neurologically intact due to canal widening
- Degenerative: C3/4, C4/5; disc + facet arthropathy; 64% present with myelopathy
- Dean's classification: Type I (adjacent to stiff segment) vs. Type II (within spondylotic segment)
- Stability criteria: >3.5 mm translation OR >11° angulation = instability (White & Panjabi)
- MRI: investigation of choice; T2 cord signal change = myelomalacia = poor prognosis
- Flexion-extension X-rays: essential to demonstrate dynamic instability
- Lhermitte's + Hoffman's + inverted radial reflex: hallmarks of cervical myelopathy
- ACDF: standard procedure for 1–2 level disease
- Type IIa Hangman's: DO NOT apply traction — extension + halo
- Posterior stabilisation for Type III Hangman's and bilateral facet dislocations
Recent advances in spondylolisthesis cervical lubar
lumbar spondylolisthesis treatment advances
cervical spondylolisthesis surgical treatment outcomes
recent advances spondylolisthesis 2023 2024 2025 minimally invasive surgery robotic navigation
spondylolisthesis fusion decompression TLIF PLIF
minimally invasive spine surgery spondylolisthesis MIS-TLIF outcomes
degenerative spondylolisthesis decompression alone versus fusion
LIFT trial TLIF PLIF spondylolisthesis 2024 RCT results non-inferiority
PMID: 38369106
PMID: 36849239
PMID: 41043182
PMID: 41067692
spondylolisthesis robotic navigation pedicle screw accuracy
PMID: 40638017
PMID: 40605215
endoscopic spine surgery spondylolisthesis full endoscopic TLIF
cervical spondylotic myelopathy laminoplasty ACDF outcomes