Pcpndt act
Searching the Web
PCPNDT Act India 1994 key provisions amendments 2003
Finding Sources
Here is a thorough overview of the PCPNDT Act (Pre-Conception and Pre-Natal Diagnostic Techniques Act):
PCPNDT Act - Overview
Full Name
The Pre-Conception and Pre-Natal Diagnostic Techniques (Prohibition of Sex Selection) Act, 1994 (as amended in 2003)
Background & History
- 1987: Maharashtra became the first state to enact its own law regulating PNDT.
- 1994: The Central Government passed the PNDT Act (Pre-Natal Diagnostic Techniques Act), which came into force on January 1, 1996.
- 2001: The Supreme Court passed an interim judgment in CEHAT vs. Union of India (2001) 5 SCC 577, mandating strict implementation.
- 2003: The PNDT Act was amended and renamed as the PCPNDT Act to cover pre-conception sex selection and address practical gaps.
- 2005/2008: Constitutional validity of the Act was upheld in Vinod Soni vs. Union of India and Vijay Sharma vs. Union of India.
Objective / Preamble
The Act aims to:
- Prohibit sex selection - before or after conception
- Regulate prenatal diagnostic techniques - for detecting genuine medical conditions (genetic abnormalities, metabolic disorders, chromosomal abnormalities, congenital malformations, sex-linked disorders)
- Prevent misuse of such techniques for sex determination leading to female foeticide
Key Provisions
Permitted Uses of Prenatal Diagnostic Techniques
Prenatal diagnosis is allowed ONLY when the pregnant woman is:
- Age 35 or above
- Has had 2 or more spontaneous abortions or foetal loss
- Has been exposed to potentially teratogenic agents (drugs, radiation, infection, chemicals)
- Has a family history of mental retardation or physical deformities
- Has any other condition specified by the Central Supervisory Board (CSB)
Prohibited Acts
- Sex determination of foetus by any technique
- Communicating the sex of the foetus to the pregnant woman or her relatives (by word, sign, or any other method)
- Conducting or abetting sex-selective abortions
- Advertising any technique for sex determination
- Sale of ultrasound machines to unregistered bodies
Compulsory Registration
All the following must be registered:
- Genetic Counselling Centres
- Genetic Laboratories
- Genetic Clinics
- Ultrasound Clinics
- Imaging Centres
Consent & Record-Keeping
- Informed written consent of the pregnant woman is mandatory before any procedure
- Detailed Form F must be filled for every ultrasound/diagnostic procedure
- All records must be maintained and made available for inspection
Prohibition of Advertisements (Section 22)
No person or organisation may advertise any service for sex determination. Violations attract up to 3 years imprisonment and a fine up to Rs. 10,000.
Regulatory Authorities
| Level | Authority |
|---|---|
| Central | Central Supervisory Board (CSB) - chaired by the Union Health Minister |
| State | State Supervisory Board (SSB) - chaired by State Health Minister (added in 2003) |
| District | Appropriate Authority (AA) - at district level for registration and enforcement |
| Advisory | Advisory Committees at central and state levels |
The Appropriate Authority has powers of a civil court for search, seizure, and sealing of equipment (empowered by the 2003 amendment).
Penalties (Sections 23-25)
| Offence | First Conviction | Subsequent Conviction |
|---|---|---|
| Conducting sex determination / violating Act | 3 years imprisonment + Rs. 10,000 fine | 5 years imprisonment + Rs. 50,000 fine |
| Seeking sex determination (woman or relative) | Presumed under compulsion; woman is not penalized | - |
| Advertising | 3 years imprisonment + Rs. 10,000 fine | - |
- A registered medical practitioner convicted under this Act is reported to the respective State Medical Council, which may suspend or cancel their registration.
2003 Amendment - Key Changes
- Coverage extended to pre-conception sex selection techniques
- Ultrasound machines brought within the ambit of the Act
- Empowerment of the Central Supervisory Board; creation of State Supervisory Boards
- More stringent punishments introduced
- Appropriate authorities empowered with powers of a civil court for search, seizure, and sealing
- Regulation of sale of ultrasound machines - only to registered bodies
Important Points for Exams
- The Act is administered by the Ministry of Health & Family Welfare.
- Sex of the foetus must not be disclosed even if accidentally detected.
- The burden of proof in certain cases is reversed - the accused must prove innocence.
- Form F is the key form for ultrasound documentation.
- The pregnant woman who undergoes sex determination is not punishable (she is treated as a victim of compulsion).
- Both the person conducting AND the person seeking sex determination (except the woman) are liable.
This Act is a significant piece of social legislation in India aimed at addressing the declining child sex ratio (particularly female infanticide and foeticide), and remains a key topic in medical law, community medicine, and forensic medicine syllabi.
Morden sewage treatment plant
Searching the Web
modern sewage treatment plant processes stages technology 2024
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Excellent! I have everything needed for a complete, well-illustrated answer from Park's Textbook.
Modern Sewage Treatment Plant
(Source: Park's Textbook of Preventive and Social Medicine)
Aim of Sewage Treatment
The aim of sewage treatment is to "stabilize" the organic matter so it can be safely disposed of, and to convert sewage water into an effluent of acceptable purity for disposal into land, rivers, or the sea.
Raw or inadequately treated sewage must never be discharged into water bodies because:
- Aerobic bacteria deplete dissolved oxygen, killing aquatic life
- Anaerobic decomposition produces hydrogen sulphide (offensive odour)
Indicators of Sewage Strength
| Parameter | Definition | "Weak" | "Strong" |
|---|---|---|---|
| BOD (Biochemical Oxygen Demand) | O₂ absorbed over 5 days at 20°C | 100 mg/L | 300 mg/L |
| COD (Chemical Oxygen Demand) | O₂ equivalent for chemical oxidation | - | Used when toxic substances are present |
| Suspended Solids | Particulate matter in sewage | 100 mg/L | 500 mg/L |
Decomposition of Organic Matter
- Aerobic process - Most efficient; requires free dissolved O₂. Organic matter broken down into CO₂, water, ammonia, nitrates, and sulphates by bacteria, fungi, and protozoa.
- Anaerobic process - Used for highly concentrated sewage. End-products are methane, ammonia, CO₂, and H₂. Reactions are slower but effective.
Flow Diagram of a Modern Sewage Treatment Plant
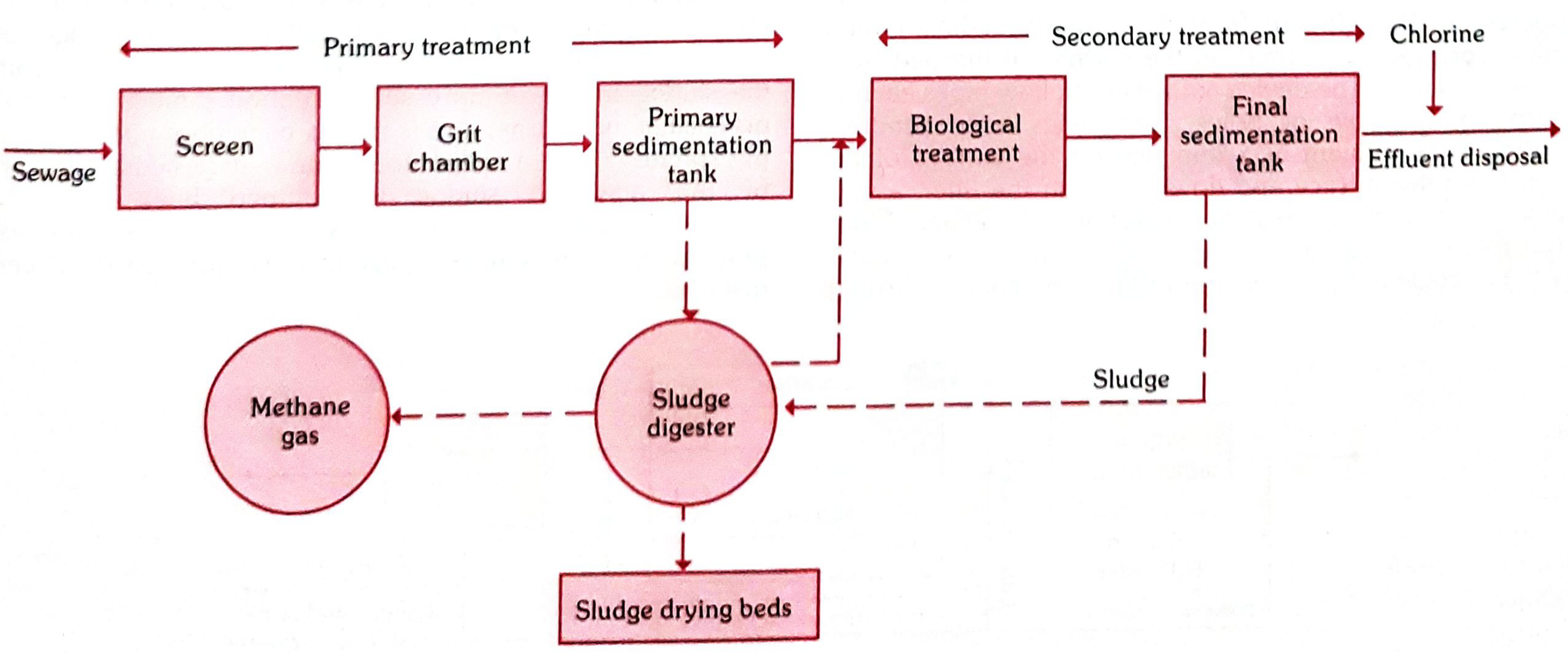
A. PRIMARY TREATMENT (Physical)
1. Screening
- Sewage first passes through a metal screen with steel bars set 5 cm apart
- Removes large floating objects: wood, rags, garbage, dead animals
- Prevents clogging of the plant
- Fixed or moving type screens; screenings disposed of by trenching/burial
2. Grit Chamber (Detritus Chamber)
- Long narrow chamber, 10-20 metres in length
- Maintains constant velocity of ~1 foot/second, detention period of 30 seconds to 1 minute
- Allows settlement of heavier solids (sand, gravel) while letting organic matter pass through
- Grit disposed by plain dumping or trenching
3. Primary Sedimentation Tank
- Huge tank holding 1/4 to 1/3 of dry weather flow
- Sewage flows slowly at 1-2 feet/minute, detention time of 6-8 hours
- 50-70% of solids settle by gravity (sedimentation)
- 30-40% reduction in coliform organisms
- Settled organic matter = sludge (removed mechanically)
- Fat/grease rises as scum (removed periodically)
- Chemical treatment with lime, aluminium sulphate, or ferrous sulphate when trade waste is present
B. SECONDARY TREATMENT (Biological/Aerobic)
Effluent from primary tank still contains dissolved organic matter and living organisms with high BOD. It is subjected to aerobic oxidation by one of two methods:
(a) Trickling Filter Method
- A bed of crushed stones or cinder, 1-2 m deep and 2-30 m in diameter
- Effluent from primary tank is sprinkled uniformly on the bed surface by a revolving device
- A complex biological growth (zoogleal layer - algae, fungi, protozoa, bacteria) develops on the stone surface
- As effluent percolates through, it gets oxidized by bacterial flora in the zoogleal layer
- Action is biological, not mechanical filtration - the name "filter" is a misnomer
- Dead biological material (humus) washes down and is collected in secondary sedimentation tanks
- Suitable for smaller towns - cheaper to install and easier to operate
(b) Activated Sludge Process (Modern method)
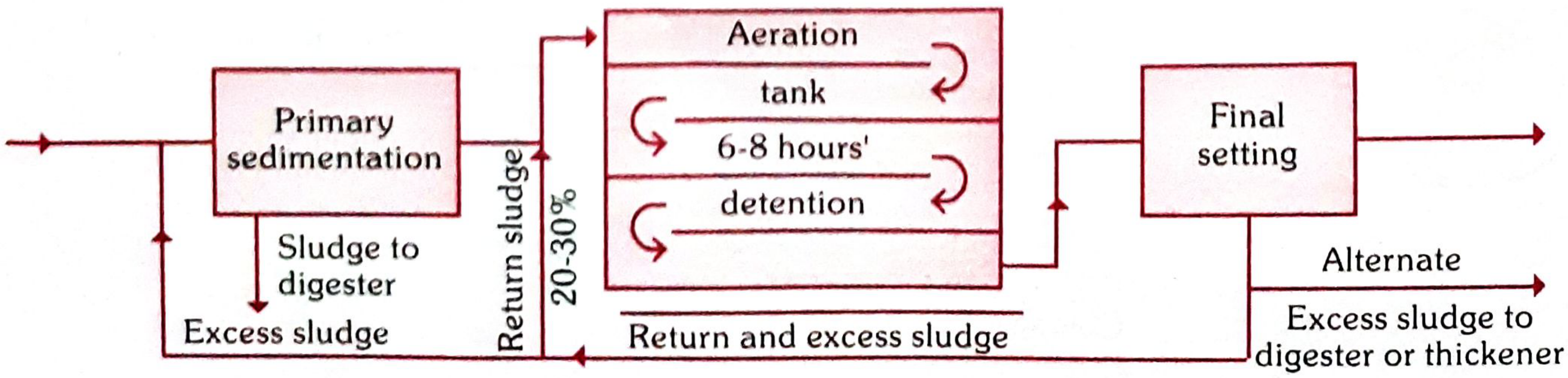
- The "heart" is the aeration tank
- Effluent from primary tank is mixed with return sludge (20-30% of incoming flow) from the final settling tank - this return sludge is a rich culture of aerobic bacteria
- Mixture is aerated in the aeration chamber for 6-8 hours
- Aeration methods:
- Mechanical agitation
- Diffuse aeration (compressed air forced from bottom) - considered better
- During aeration, organic matter is oxidized into CO₂, nitrates, and water
- Typhoid and cholera organisms are destroyed; coliforms are greatly reduced
- 1 acre of activated sludge plant = work of 10 acres of percolating filter
- Suitable for larger cities - requires skilled operation but occupies less space
Secondary Sedimentation Tank
- Oxidized sewage is detained for 2-3 hours
- Settled sludge = "activated sludge" (aerated, practically inoffensive, rich in bacteria, nitrogen, phosphates)
- Part of this sludge is pumped back to the aeration tanks (return sludge)
- Remainder goes to sludge digestion tanks
- Final effluent is chlorinated before disposal
C. SLUDGE TREATMENT & DISPOSAL
Sludge Digestion
- 1 million gallons of sewage produces 15-20 tons of sludge (95% water, revolting odour)
- Modern plants use anaerobic auto-digestion in sludge digestion tanks
- Takes 3-4 weeks for complete digestion
- End-products:
- Methane gas - used for heating and lighting
- Residue is inoffensive, tarry mud - excellent manure when dried
- Other methods: sea disposal (coastal cities), land composting with town refuse
D. EFFLUENT DISPOSAL
By Dilution (into rivers/streams)
- Effluent must be chlorinated to remove pathogens before discharge
- Royal Commission Standards (1908): effluent must have
- Suspended solids: ≤30 mg/litre
- 5-day BOD: ≤20 mg/litre
- (Assumed 8:1 dilution by the receiving water body)
- These remain the backbone of sewage effluent purity standards
By Land Application
- Used in irrigation or for sludge composting
Comparison: Trickling Filter vs Activated Sludge Process
| Feature | Trickling Filter | Activated Sludge |
|---|---|---|
| Space required | Large (10 acres per unit) | Small (1 acre) |
| Installation cost | Cheaper | Higher |
| Operation | Simple, easy | Requires skilled staff |
| Best suited for | Smaller towns | Larger cities |
| Aeration | Natural (wind through bed) | Mechanical/diffuse |
- Park's Textbook of Preventive and Social Medicine, pp. 865-868
Healt problem in tribal areas
Finding Sources
Searching the Web
health problems tribal areas India malaria malnutrition sickle cell
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
I now have comprehensive content from Park's Textbook. Let me compile the full answer.
Health Problems in Tribal Areas
(Source: Park's Textbook of Preventive and Social Medicine)
Who Are Tribal People?
- The term "Scheduled Tribes" is defined under Article 366(25) of the Indian Constitution
- Over 104 million tribal people live in India, spread across 705 tribes, accounting for 8.6% of the population
- Concentrated in 10 major states and 8 North-East states; ~90% live in rural/hilly/forested areas
- Numerically largest: Madhya Pradesh (15 million) > Maharashtra (10 million) > Odisha (9 million) > Rajasthan (9 million)
- They have remained marginal - geographically, socio-economically, and politically
Demographic Indicators
| Indicator | Tribal (ST) | National Average |
|---|---|---|
| Life Expectancy at Birth | 63.9 years | 67 years |
| Literacy Rate (2011) | 59% | 73% |
| Sex Ratio (2011) | 990 per 1000 | 943 per 1000 |
| Child Sex Ratio (0-6 yrs) | 957 | 914 |
| Institutional Delivery | 68% | 78.9% |
| Postnatal Care (within 48 hrs) | 37% | Higher |
Burden of Disease - Quadruple Burden
Tribal populations suffer a "quadruple burden" of disease:
- Communicable diseases
- Non-communicable diseases
- Malnutrition
- Mental health and addictions
1. Communicable Diseases
Malaria
- Tribal population (8.6% of India) accounts for 30% of all malaria cases in India
- Responsible for >60% of P. falciparum cases and ~50% of malaria mortality
- Mobile tribal populations engaged in forest-related activities are a high-risk group
- Common vector: Anopheles culicifacies - resistant to DDT and Dieldrin
- Active hotspots: Mizoram, Tripura, Chhattisgarh, Odisha, Jharkhand, Maharashtra
Tuberculosis (TB)
- Prevalence of TB in tribal areas: 703 per 1,00,000 vs 256 per 1,00,000 in non-tribal population
- Only 11% of pulmonary TB gets treated based on smear-positive reporting
- Undernutrition significantly increases susceptibility
Leprosy
- New leprosy cases among tribals: 18.5% of total national cases
- India declared elimination (< 1/10,000) by end of 2005, but tribal pockets remain burdened
Other Communicable Diseases
- Intestinal worm infestations (due to feco-oral transmission, poor sanitation)
- Scabies
- Upper respiratory tract infections (URTI)
- Diarrhoeal diseases
- Vaccine-preventable diseases due to poor immunization coverage
2. Nutritional Problems
- 42% of children are underweight in tribal communities
- Anaemia is highly prevalent, especially in women and children (compounded by malaria and helminth infestations)
- Vitamin A deficiency - leads to night blindness and increased infection risk
- 46.5% stunting reported in states like Meghalaya
- Rising wasting rates in Nagaland
- Low BMI among tribal women is a major risk factor for maternal mortality
3. Maternal and Child Health
- Infant Mortality Rate (IMR) is significantly higher than national average
- Early marriage and early childbearing are common
- High incidence of anaemia in pregnant women
- Institutional delivery rate (68%) lower than national average (78.9%)
- Only 37% of tribal women receive postnatal care within 48 hours of home delivery
- Poor access to antenatal care, skilled birth attendance, and emergency obstetric care
4. Genetic Disorders
Sickle Cell Disease
- Prevalence of sickle cell disease (anaemia + trait combined): 1-40% across different tribal communities
- Sickle cell anaemia (homozygous) prevalent in 1 in 86 births among tribal communities in Central India
- Particularly high among Bhils of Rajasthan, Gujarat, and Madhya Pradesh
G6PD Deficiency
- Among 14 primitive tribal populations from 4 states, G6PD deficiency prevalence ranged from 0.7 to 15.6%
- Interacts with malaria susceptibility and antimalarial drug reactions
Thalassaemia
- Prevalence of thalassaemia also varies 1-40% in different tribal communities
5. Mental Health and Addictions
- 72% of tribal men (age 15-54 years) use tobacco, compared to 56% in non-tribal men
- ~50% of tribal men consume some form of alcohol
- Both tobacco and alcohol:
- Are risk factors for NCDs
- Reduce productivity and increase poverty
- Disrupt family harmony
- Generate law and order problems
6. Non-Communicable Diseases (NCDs)
- Increasing burden of hypertension, diabetes, cardiovascular diseases
- Aggravated by tobacco and alcohol use
- Limited screening and early detection facilities in remote areas
7. Animal Attacks and Violence
- Forest-dwelling tribal communities face snake bites, dog bites, and scorpion stings
- Timely anti-snake venom and anti-rabies treatment often unavailable
- Conflict areas add additional burden of injury and violence
Root Causes of Poor Health in Tribal Areas
| Factor | Detail |
|---|---|
| Geographic isolation | Hilly/forested terrain, poor roads, hard-to-reach habitations |
| Poverty | Low income, food insecurity, inability to afford healthcare |
| Poor sanitation | Open defecation, contaminated water supply |
| Low literacy | Especially among women - limits health-seeking behaviour |
| Cultural barriers | Traditional beliefs, dependence on faith healers |
| Limited healthcare infrastructure | Few PHCs, CHCs; shortage of doctors willing to serve in tribal areas |
| Displacement | Development-induced displacement disrupts community health networks |
Healthcare Initiatives for Tribal Areas
- Tribal Sub-Plan (TSP) strategy (now Scheduled Tribal Component - STC) from 5th Five Year Plan
- Ministry of Tribal Affairs and Ministry of Health & Family Welfare run tailored schemes
- Mobile health units to reach remote populations
- Tribal Health Expert Committee (constituted 2013) identified 10 special problems with targets:
- Control malaria
- Reduce malnutrition and child mortality
- Ensure safe motherhood
- Address sickle cell disease
- Promote health literacy
- Treat animal bites and accidents
- Provide family planning + infertility care
- NAMS Task Force on Tribal Health (2024) focused on hemoglobinopathies, NCD burden, mental health, maternal health, oral health, and access
- Encouragement of traditional medicine documentation and promotion of medicinal plant cultivation
- Park's Textbook of Preventive and Social Medicine, pp. 801-807 | PMC Article on Tribal Health | NAMS Task Force Report 2024
This is a shared conversation. Sign in to Orris to start your own chat.