Celecoxib?
Reading File
Finding Sources
Searching PubMed
celecoxib COX-2 inhibitor
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a thorough overview of Celecoxib drawn from multiple authoritative pharmacology and rheumatology textbooks:
Celecoxib
Class & Mechanism
Celecoxib (brand: Celebrex) is a selective COX-2 inhibitor (coxib class) - a diaryl heterocyclic NSAID. It is a benzenesulfonamide approximately 10-20 times more selective for COX-2 than COX-1 at usual therapeutic doses.
Key distinction from non-selective NSAIDs:
- COX-1 (constitutive): found in GI mucosa, kidneys, platelets - responsible for protective prostaglandins and thromboxane-mediated platelet aggregation
- COX-2 (inducible): upregulated at sites of inflammation, injury, and cancer
- Celecoxib inhibits the inflammatory COX-2 pathway without substantially blocking COX-1, reducing GI toxicity relative to traditional NSAIDs
- It does not significantly inhibit thromboxane A2 (platelet aggregation is unaffected at usual doses)
- It does suppress prostacyclin (PGI2) synthesis in vascular endothelium (via COX-2) - contributing to cardiovascular risk
Unlike aspirin's irreversible COX-1 inhibition, celecoxib's COX-2 inhibition is reversible.
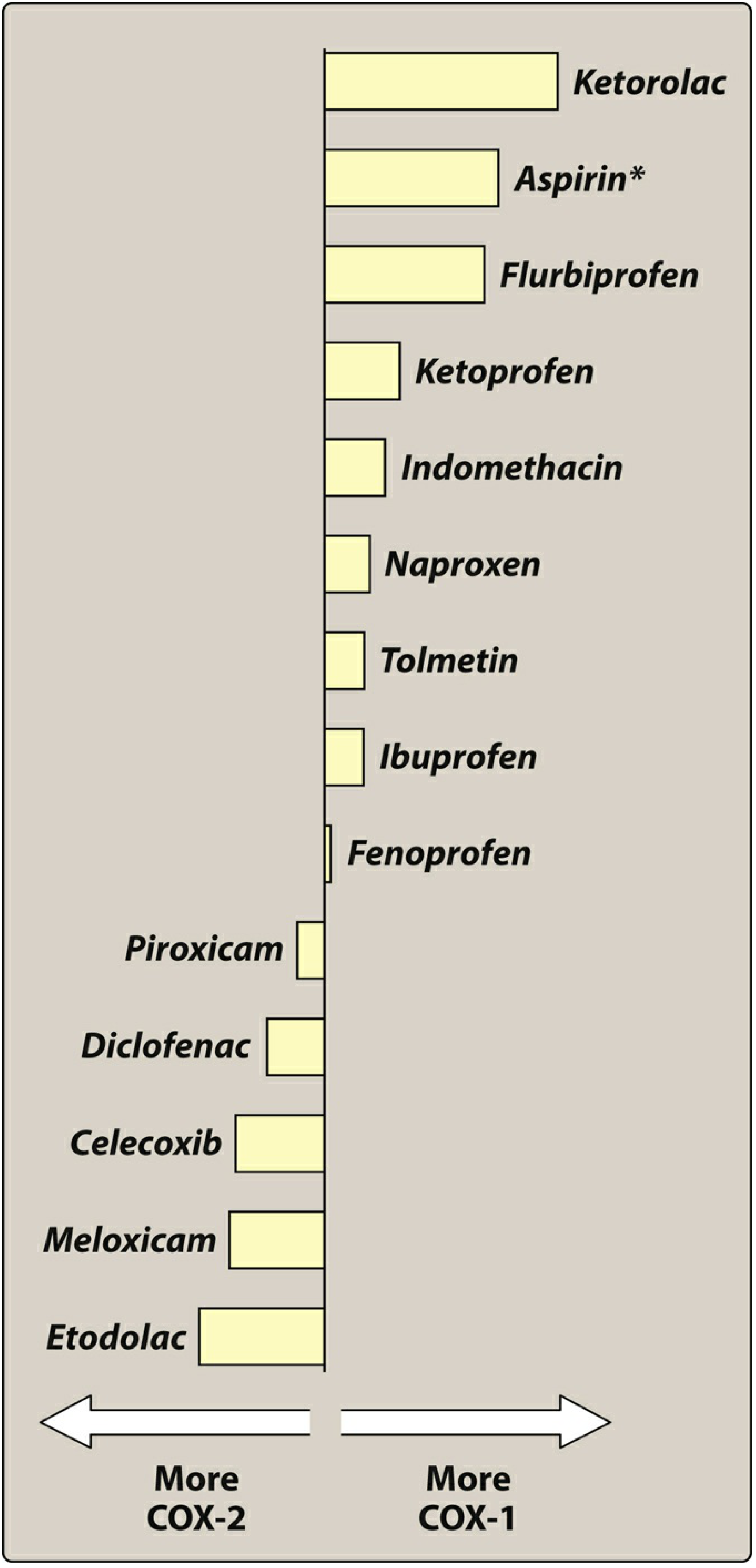
COX-2 Selectivity in Context
The chart below ranks NSAIDs from most COX-2 selective (left) to most COX-1 selective (right):
Indications
- Osteoarthritis (OA)
- Rheumatoid arthritis (RA)
- Juvenile rheumatoid arthritis (JRA) in children ≥2 years
- Ankylosing spondylitis (AS)
- Acute pain (post-surgical, dysmenorrhea)
- Off-label / investigational: adjunctive therapy for schizophrenia (400 mg/day, targeting neuroinflammation); anti-inflammatory therapy for depression
Pharmacokinetics
| Parameter | Details |
|---|---|
| Route | Oral |
| Peak (Cmax) | ~3 hours |
| Protein binding | 97% |
| Metabolism | Liver - primarily CYP2C9 (major), CYP3A4 (minor), glucuronidation |
| Half-life | ~11 hours |
| Dosing frequency | Once or twice daily |
| Excretion | Feces and urine (as metabolites) |
Dose adjustments:
- Moderate hepatic impairment: reduce dose by 50%
- Severe hepatic or renal disease: avoid
Dosing
| Indication | Dose |
|---|---|
| OA | 200 mg once daily or 100 mg twice daily |
| RA, AS | 100-200 mg twice daily |
| Acute pain | 400 mg loading dose, then 200 mg if needed on Day 1; thereafter 200 mg twice daily |
| Max daily dose | 800 mg/day |
| Children ≥2 y (JRA) | 50 mg twice daily (10-25 kg); 100 mg twice daily (>25 kg) |
Adverse Effects
GI
- Causes fewer endoscopic ulcers and GI bleeding than most traditional NSAIDs (the primary clinical advantage)
- This GI benefit is lost when aspirin is co-administered - patients requiring concomitant aspirin (cardiovascular prophylaxis) should be aware of this
- Common: headache, dyspepsia, diarrhea, abdominal pain
Cardiovascular
- Like all NSAIDs, celecoxib carries a risk of myocardial infarction and stroke (black box warning)
- The PRECISION trial (>24,000 patients; OA/RA with high CV risk) compared celecoxib vs. ibuprofen vs. naproxen - celecoxib was non-inferior to ibuprofen and naproxen for cardiovascular outcomes (not worse, but not safer)
- The CV risk arises because celecoxib suppresses COX-2-derived prostacyclin (vasodilatory, antithrombotic) but does not suppress COX-1-derived thromboxane A2 (prothrombotic) - creating a prothrombotic imbalance
- Patients at high CV risk + high GI risk who also need aspirin should use naproxen or celecoxib + PPI
Renal
- Renal toxicity similar to traditional NSAIDs (COX-2 is active in the kidney for prostaglandin-mediated afferent arteriole dilation)
- Avoid in severe renal disease
Bone
- Chronic use may decrease bone mineral density, particularly in older males
- May slow fracture healing and tendon-to-bone healing
Allergy
- Contraindicated in patients with sulfonamide allergy (due to the sulfonamide moiety in its structure)
- Also contraindicated in patients with aspirin/NSAID-sensitive asthma or urticaria (cross-reactivity possible)
Drug Interactions
| Interacting Drug | Consequence |
|---|---|
| Aspirin | Loses GI protection benefit; combined use increases GI risk |
| Warfarin | Occasional interaction (CYP2C9 inhibition) - monitor INR |
| Lithium | Celecoxib increases lithium plasma concentrations |
| Fluconazole | Celecoxib increases fluconazole concentrations (via CYP2C9) |
| CYP2D6 substrates | Celecoxib inhibits CYP2D6 - may increase levels of tricyclics, antipsychotics, etc. |
Contraindications
- Severe hepatic or renal impairment
- Sulfonamide hypersensitivity
- NSAID-/aspirin-sensitive asthma
- Perioperative CABG surgery (all NSAIDs)
- Pregnancy (especially third trimester - risk of premature closure of ductus arteriosus)
- History of peptic ulcer disease / GI bleeding (relative)
Special Populations
- Pregnancy: Avoid, especially in the third trimester
- Elderly: Use lowest effective dose; monitor renal function
- CYP2C9 poor metabolizers: Higher drug exposure - use with caution, consider dose reduction
Key Clinical Takeaway
Celecoxib is the only purposefully developed COX-2 selective inhibitor still approved in the US (rofecoxib/Vioxx and valdecoxib/Bextra were withdrawn due to cardiovascular events). It offers a genuine GI advantage over non-selective NSAIDs only when aspirin is not co-prescribed. Its cardiovascular risk is comparable to ibuprofen and naproxen (per the PRECISION trial), not lower - so it is not a "safer" NSAID for the heart.
Sources: Lippincott Illustrated Reviews: Pharmacology, p. 1361-1363 | Katzung's Basic & Clinical Pharmacology, 16th ed. | Goodman & Gilman's The Pharmacological Basis of Therapeutics | Firestein & Kelley's Textbook of Rheumatology
Recent evidence: A 2025 umbrella review (PMID 40911151) assessed celecoxib safety in chronic musculoskeletal conditions - no major new safety signals beyond established cardiovascular and GI considerations. A 2025 meta-analysis (PMID 40833536) found celecoxib shows efficacy in adjunctive treatment of schizophrenia.
This is a shared conversation. Sign in to Orris to start your own chat.