Teach me date rape drugs / club drugs… in detail.. every single thing … introduction of each , mechanism, street name, how is it abused, intoxication, dependence, misuse abuse, clinical features. Withdrawal, acture treatment of intoxication, treatment of withdrawal,… dependence treatment… every single thing… and recent advances… in detail
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Searching PubMed
GHB flunitrazepam ketamine MDMA date rape club drugs
Reading File
Finding Sources
Finding Sources
Searching PubMed
club drugs treatment intoxication withdrawal
Reading File
Reading File
Reading File
Searching the Web
date rape club drugs GHB ketamine MDMA rohypnol clinical features treatment 2024 2025
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive data from multiple authoritative textbooks. Let me compile the full detailed response.
Date Rape Drugs / Club Drugs - Complete Clinical Guide
Sources: Rosen's Emergency Medicine 10e, Kaplan & Sadock's Synopsis of Psychiatry, Maudsley Prescribing Guidelines 15e, Lippincott Illustrated Reviews: Pharmacology, Stahl's Essential Psychopharmacology, Tintinalli's Emergency Medicine, Forensic Medicine & Toxicology 36e (2026), Kaplan-Sadock Synopsis
INTRODUCTION AND OVERVIEW
Club drugs are a pharmacologically heterogeneous group of psychoactive compounds abused primarily by adolescents and young adults at nightclubs, bars, raves, and trance scenes. The major agents are:
| Drug | Class | Primary Role |
|---|---|---|
| GHB (gamma-hydroxybutyrate) | CNS depressant / GABA-ergic | Date rape + recreation |
| Flunitrazepam (Rohypnol) | Benzodiazepine | Date rape + recreation |
| Ketamine | Dissociative anesthetic | Club drug + date rape |
| MDMA (Ecstasy) | Empathogen-entactogen amphetamine derivative | Club drug |
| Methamphetamine | Stimulant | Club drug |
| LSD | Hallucinogen | Club drug |
The Drug-Induced Rape Prevention and Punishment Act was passed by Congress specifically because GHB, flunitrazepam, and ketamine are often colorless, tasteless, and odorless - making them ideal for surreptitious addition to beverages. GHB, ketamine, and Rohypnol are specifically termed "date rape drugs" because they produce disorientation, sedation, and anterograde amnesia - victims often cannot recall events during drug exposure. - Kaplan & Sadock's Synopsis of Psychiatry
DRUG 1: GHB (Gamma-Hydroxybutyrate)
Introduction
GHB (gamma-hydroxybutyrate; sodium oxybate) is an endogenous short-chain fatty acid naturally present in the mammalian brain where it functions as a neurotransmitter. It was first synthesized in the 1960s and originally explored as an anesthetic agent. It is FDA-approved (as Xyrem) for narcolepsy with cataplexy (2002), but with severe restrictions. Illicitly, it is known as "liquid X", "liquid ecstasy", "liquid G", "Georgia Home Boy", "grievous bodily harm (GBH)", "fantasy", and "easy lay." Its precursors, gamma-butyrolactone (GBL) and 1,4-butanediol (BDO/BD), are converted to GHB in the body and are abused in the same fashion. - Dermatology 5e, Stahl's Essential Psychopharmacology
Street Names
- Liquid Ecstasy, Liquid X, Liquid G
- GBH (Grievous Bodily Harm)
- Georgia Home Boy
- Fantasy, Easy Lay, Scoop
- Goop, Cherry Meth, Organic Quaalude
Mechanism of Action
GHB is an endogenous CNS substance formed from GABA. It acts as:
- A full agonist at specific GHB receptors (dedicated receptors in the brain)
- A partial agonist at GABA-B receptors - acting as an antagonist when GABA is high and an agonist when GABA is low
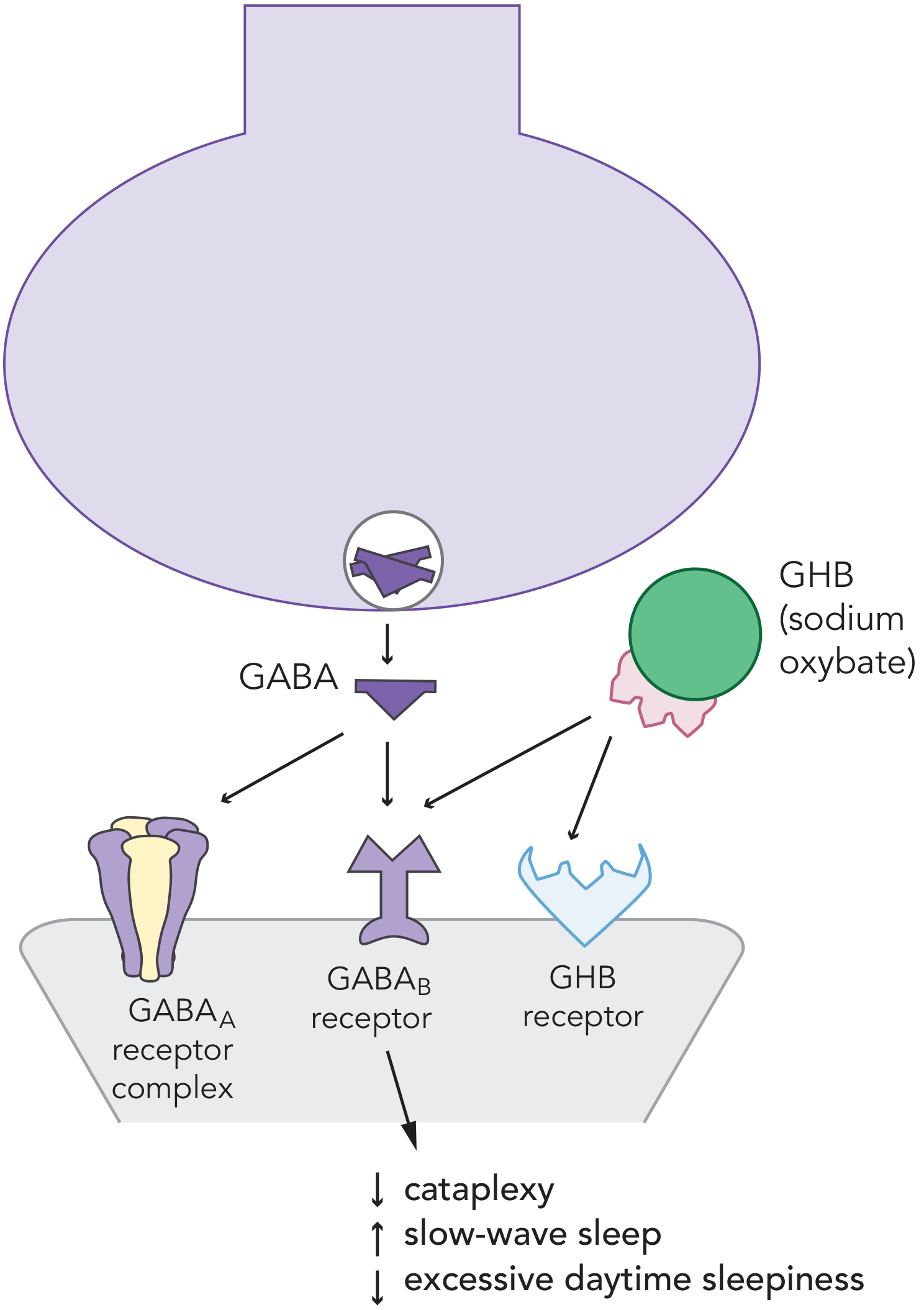
Figure: GHB (sodium oxybate) acts as a full agonist at GHB receptors and partial agonist at GABA-B receptors, reducing cataplexy, increasing slow-wave sleep, and reducing excessive daytime sleepiness. - Stahl's Essential Psychopharmacology
At recreational doses, GHB produces profound CNS depression. Because it reportedly promotes muscle mass and elevates growth hormone in vivo, it has also been misused by bodybuilders. - Dermatology 5e
Physical Appearance and How It Is Used/Abused
- Usually a clear, colorless liquid with a slightly salty taste; also available as white powder or capsules
- Virtually odorless and tasteless in beverages - ideal for surreptitious drugging
- Administered orally (swallowed directly or mixed into drinks)
- Onset: 15-30 minutes after ingestion
- Duration: effects last up to 6 hours
- Ingestion of 1 g produces euphoria and relaxation
- Ingestion of 2 g produces deep sleep
- Ingestion of 4 g produces coma - particularly when mixed with alcohol (synergistic effect)
- Also misused by bodybuilders for its anabolic properties
Intoxication / Clinical Features
CNS:
- Dose-dependent sedation ranging from euphoria → disinhibition → sedation → coma
- Anterograde amnesia (critical for date rape use)
- Dizziness, confusion, disorientation
- Slurred speech, ataxia
- Hallucinations (at higher doses)
Cardiovascular:
- Bradycardia
- Hypotension
Respiratory:
- Respiratory depression (potentially life-threatening)
- Apnea
Other:
- Nausea, vomiting
- Myoclonic jerks (can resemble seizures)
- Hypotonia
- Hypothermia
- Diaphoresis
Key clinical point: Despite marked CNS depression, GHB patients may awaken suddenly and become agitated - a characteristic feature. Concomitant traumatic injuries (from falls/syncope) are common and must be excluded. - Rosen's Emergency Medicine
Dependence
GHB produces rapid physiological dependence with tolerance developing quickly, particularly in frequent users. Withdrawal from GHB/GBL can be life-threatening, similar to alcohol and benzodiazepine withdrawal.
Withdrawal Syndrome
GHB withdrawal is potentially fatal and represents a medical emergency. Features include:
- Onset: 1-6 hours after last dose (very rapid, due to GHB's short half-life of ~30-60 minutes)
- Autonomic instability: tachycardia, hypertension, diaphoresis, fever
- Neurological: tremors, agitation, confusion, delirium, psychosis
- Seizures (can be severe)
- Insomnia (often profound)
- Course can resemble alcohol withdrawal delirium (delirium tremens)
- Can persist 5-15 days, longer than alcohol withdrawal
Key distinguishing feature: GHB withdrawal often requires very high doses of benzodiazepines that would be sedating in other contexts - patients rapidly metabolize/tolerate BZDs. - Rosen's Emergency Medicine, Maudsley Guidelines 15e
Acute Treatment of Intoxication
- Primarily supportive - no specific antidote exists
- Airway management and respiratory support (intubation if needed)
- IV access, cardiac monitoring, pulse oximetry
- Position in recovery position to prevent aspiration
- Exclude co-ingestants (especially opioids, alcohol, other CNS depressants)
- Exclude traumatic injuries
- Flumazenil and naloxone are not effective
- Most patients recover spontaneously within 2-6 hours
Treatment of Withdrawal (Maudsley Guidelines 15e)
Setting: Inpatient - GHB withdrawal is a medical emergency.
First-line: High-dose benzodiazepines (e.g., diazepam titrated to effect) - doses often far exceed normal sedative doses
Protocol:
- Use CIWA-Ar (Clinical Institute Withdrawal Assessment) to monitor severity
- Diazepam loading in severe cases
- Baclofen 10 mg PO TDS added as adjunctive pharmacotherapy where benzodiazepines prove inadequate (baclofen acts at GABA-B receptors, similar to GHB's partial agonism)
- Phenobarbital has been used for severe GHB withdrawal (case series, 2023)
- Pharmaceutical-grade GHB tapering (in Netherlands/Belgium protocol): more physiological, reduces seizure risk - matched-subject observational study showed non-inferiority to BZD tapering (Beurmanjer et al., CNS Drugs 2020)
Key references:
- Dijkstra et al: Detoxification with titration and tapering in GHB-dependent patients - Dutch GHB monitor project. Drug Alcohol Depend 2017; 170:164-173
- Freeman et al: Phenobarbital to manage severe GHB withdrawal: a case series. Drug Alcohol Rev 2023; 42:27-32
Dependence Treatment / Long-Term
- No established pharmacotherapy for GHB use disorder
- Cognitive behavioral therapy and motivational enhancement
- Baclofen has been investigated as maintenance therapy (GABA-B agonist)
- Monitoring for co-occurring stimulant use disorder (GHB is frequently co-used with methamphetamine in chemsex contexts)
DRUG 2: FLUNITRAZEPAM (Rohypnol)
Introduction
Flunitrazepam (marketed as Rohypnol by Roche) is a potent benzodiazepine with rapid onset, manufactured legally in over 60 countries for preoperative sedation and treatment of severe insomnia, but never approved for use in the United States or Canada. It gained prominence in the US in the 1990s as an inexpensive recreational sedative and "date rape" drug. It is classified as a Schedule I controlled substance in the US. - Rosen's Emergency Medicine, Forensic Medicine & Toxicology 36e
Street Names
- Roofies, Roche, Rope
- La Roche, Rib, Forget-Me Pill
- Mexican Valium, Mind Eraser
- Wolfies, Circles
Mechanism of Action
Flunitrazepam has 10 times greater affinity for benzodiazepine receptors than diazepam. It binds to the benzodiazepine site on the GABA-A receptor complex, enhancing chloride ion conductance, causing membrane hyperpolarization and CNS depression. This produces:
- Sedation and hypnosis
- Anterograde amnesia (the key factor in date rape)
- Muscle relaxation
- Anxiolysis
- Anticonvulsant effects
Physical Appearance and How It Is Used/Abused
- Originally: white tablet, odorless and tasteless when dissolved
- Current formulation (after regulation): Light green pill with blue core - turns beverages blue when dissolved, to aid detection. However, generic versions may not contain the blue dye.
- Tablets sold on street for $0.50-$5 each
- Most tablets in North America produced illegally in Mexico/Latin America
- Packaged in foil-backed clear plastic blister packs
- Ingested orally; commonly used with alcohol (potentiates effects dramatically)
- Also snorted, and occasionally injected
- Used by cocaine abusers to moderate the "comedown" from stimulants
Intoxication / Clinical Features
Onset: 20-30 minutes after ingestion, peak at ~2 hours
Half-life: 16-36 hours; coma can be prolonged up to 48 hours
- Disinhibition (similar to alcohol but more pronounced)
- Profound sedation, confusion, disorientation
- Anterograde amnesia (hallmark - complete blackout)
- Slurred speech, impaired coordination
- Hypotonia, muscle relaxation
- Loss of consciousness at higher doses
- Respiratory depression
- Paradoxical agitation possible
- Despite marked CNS depression, patients can usually be aroused with noxious stimuli
Combination with alcohol: Dramatically potentiates all effects - rapid loss of consciousness, severe amnesia. - Rosen's Emergency Medicine, Forensic Medicine & Toxicology 36e
Dependence and Withdrawal
Since flunitrazepam is a benzodiazepine, it produces the full benzodiazepine dependence syndrome:
- Dependence develops with repeated use (days to weeks)
- Tolerance develops across all effects
- Withdrawal can be life-threatening - similar to alcohol withdrawal
Withdrawal features:
- Anxiety, agitation, insomnia
- Tremors, sweating
- Tachycardia, hypertension
- Seizures (potentially fatal)
- Psychosis, delirium
- Timeline: onset 24-72 hours after last dose, can last 1-2 weeks
Acute Treatment of Intoxication
- Supportive care: airway protection, respiratory monitoring
- Flumazenil (benzodiazepine antagonist) - use with caution: risk of precipitating seizures in chronic users; very short duration compared to flunitrazepam's long half-life requires prolonged monitoring for recurrent sedation
- Monitor for hypoxia, hypoventilation, aspiration
- Not detected on routine urine drug screens - specific testing (police crime lab) needed; metabolites detectable up to 72 hours in urine with specialized testing
Treatment of Withdrawal
Follows standard benzodiazepine withdrawal protocols:
- 3-5 day inpatient detoxification with 24-hour intensive medical monitoring
- Long-acting benzodiazepine (diazepam) substitution and tapering
- Phenobarbital as alternative for severe cases or BZD cross-tolerance issues
- Seizure precautions throughout
- CIWA-Ar monitoring protocol
Dependence Treatment
- Standard substance use disorder treatment for benzodiazepine dependence
- Gradual taper over weeks to months
- CBT for anxiety/insomnia management
- Address underlying co-occurring substance use (often polydrug users)
DRUG 3: KETAMINE
Introduction
Ketamine is a dissociative anesthetic derived from phencyclidine (PCP), first synthesized in 1962. It is an FDA-approved medication (Schedule III) used in clinical anesthesia, procedural sedation, and increasingly in treatment-resistant depression (esketamine/Spravato). Recreationally, it is abused for its dissociative and hallucinogenic properties, particularly at clubs and raves. Sometimes used to facilitate sexual assault. In urology, ketamine has been documented in ketamine cystitis, with an estimated 200,000 users in the US having used it in a prior year. - Campbell-Walsh-Wein Urology, Stahl's, Kaplan & Sadock's
Street Names
- Special K, Vitamin K
- Kit Kat, Cat Valium
- Super K, Jet, Purple
- Super Acid, Bump
Mechanism of Action
Ketamine is a non-competitive NMDA (N-methyl-D-aspartate) receptor antagonist. It blocks the NMDA receptor channel, which normally responds to glutamate. This creates:
- Dissociative anesthesia - state of analgesia + sedation + amnesia with eyes-open
- Preservation of airway reflexes (at anesthetic doses)
- Sympathomimetic cardiovascular effects (tachycardia, hypertension)
- Hallucinogenic and psychedelic effects at sub-anesthetic doses
Additional mechanisms:
- Opioid receptor interactions
- Sigma receptor activity
- Dopaminergic and serotonergic modulation
- Activation of AMPA receptor signaling (relevant to antidepressant effect)
Physical Appearance and How It Is Used/Abused
- Commercially available as a clear liquid or off-white powder (after evaporation)
- Odorless, tasteless - can be added to drinks undetected
- Routes of abuse: intranasal ("bumps"), oral, intramuscular injection, vaporized and inhaled
- At clubs: typically snorted as powder
- Duration of action: 30-60 minutes IM; 15-30 minutes intranasal
- The "K-hole": very high doses produce a profound dissociative state with complete detachment from reality, near-death-experience feeling - sought by some users
Intoxication / Clinical Features
Low to moderate doses (recreational):
- Dissociation, derealization, depersonalization
- Euphoria, dreamlike state
- Perceptual distortions, visual/auditory hallucinations
- Altered sense of time
- Analgesia
- Mild tachycardia and hypertension (sympathomimetic)
- Nystagmus (characteristic)
- Ataxia, impaired coordination
High doses (K-hole):
- Profound dissociation, immobility
- Complete amnesia of the experience
- Respiratory depression possible (though airway reflexes usually preserved)
- Emergence reactions - agitation, confusion on awakening
Chronic use:
- Ketamine cystitis: severe, progressive lower urinary tract symptoms (frequency, urgency, dysuria, hematuria), upper tract damage (hydronephrosis), potentially requiring cystectomy
- Cognitive impairment, memory deficits
- Hepatic/biliary damage (cholangiopathy)
- Psychological dependence
Dependence and Withdrawal
- Psychological dependence is well established with regular use
- Physical dependence with withdrawal syndrome can occur with heavy use
- Withdrawal features: craving, anxiety, restlessness, diaphoresis, shaking - generally less severe than GHB or benzodiazepine withdrawal
Acute Treatment of Intoxication
- Primarily supportive - most effects short-lived
- Quiet, low-stimulation environment (reduce "emergence reactions")
- Benzodiazepines for agitation (diazepam 5-10 mg IV/IM)
- Cardiac monitoring (tachycardia/hypertension)
- Airway monitoring
- Avoid physostigmine (worsens emergence reactions)
- Benzodiazepines preferred over antipsychotics for acute agitation
Dependence Treatment
- No approved pharmacotherapy
- CBT, relapse prevention
- Urological follow-up mandatory (ketamine cystitis monitoring - renal ultrasound, cystoscopy)
- Complete abstinence often required to prevent further urological damage
- Hepatology input if biliary involvement
DRUG 4: MDMA (Methylenedioxymethamphetamine / Ecstasy)
Introduction
MDMA (3,4-methylenedioxymethamphetamine) is a synthetic derivative of methamphetamine with combined stimulant and hallucinogenic properties. First synthesized in 1912 (Merck), it was explored in psychotherapy in the 1970s-80s before being classified Schedule I in 1985. Commonly known as "Ecstasy" or "Molly", it is among the most widely used club drugs worldwide. Related compounds include MDA ("love drug"), MDEA ("Eve"), and MDPV. - Lippincott Pharmacology, Kaplan & Sadock's, Forensic Medicine 36e
Street Names
- Ecstasy, E, X, XTC
- Molly (purportedly "pure" MDMA powder)
- Adam, Beans, Roll
- Disco Biscuits, Hug Drug
- Love Drug, Clarity
Mechanism of Action
MDMA has profound serotonin-releasing effects - its primary mechanism - plus norepinephrine release and, to a lesser extent, dopamine:
- Massively increases serotonin release from presynaptic terminals into the synaptic cleft
- Blocks serotonin reuptake transporter (SERT) - preventing reuptake
- Inhibits serotonin synthesis - depleting intracellular stores acutely
- Also releases norepinephrine and dopamine
- Sometimes described as an "empathogen" due to unique serotonin-mediated emotional effects
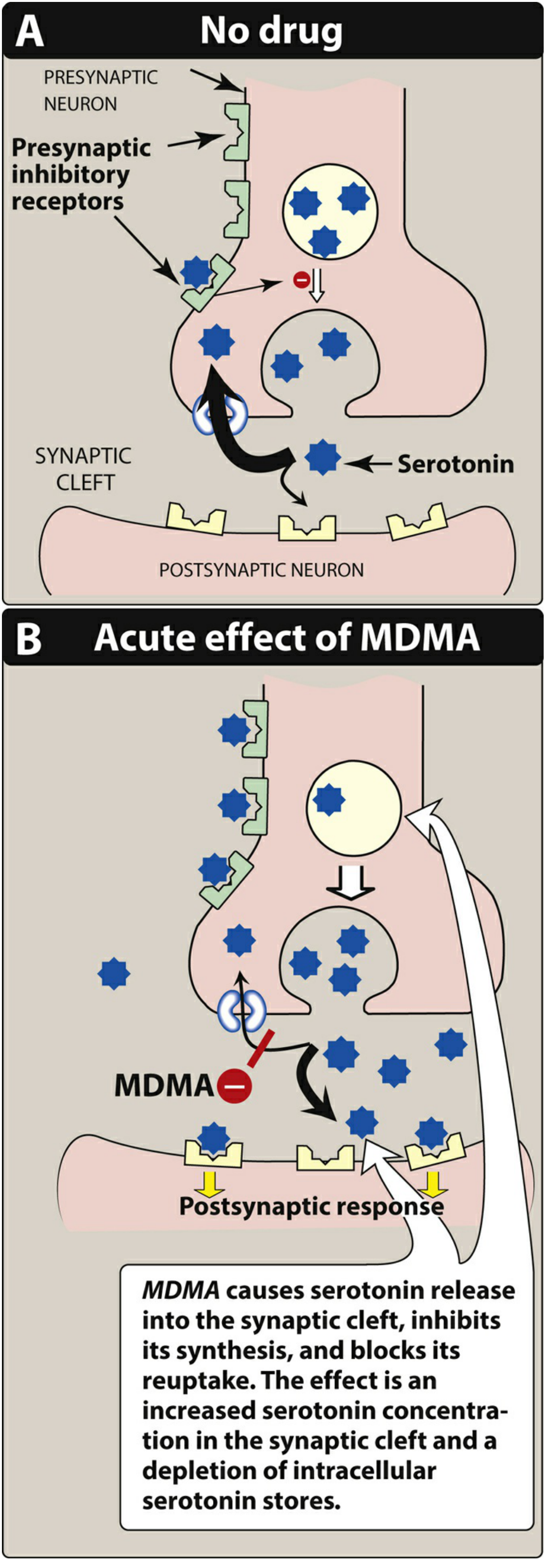
Figure: MDMA causes serotonin release into the synaptic cleft, inhibits its synthesis, and blocks its reuptake. The net effect is increased synaptic serotonin concentration and depletion of intracellular serotonin stores. - Lippincott Illustrated Reviews: Pharmacology
Physical Appearance and How It Is Used/Abused
- Colorful tablets/pills with logos (e.g., dove, mitsubishi, smiley face) - often sold as "ecstasy"
- "Molly" = crystalline powder or capsules (marketed as "purer")
- WARNING: MDMA products are frequently adulterated with methamphetamine, ketamine, methylone (synthetic cathinone), or PMA/PMMA (much more dangerous)
- Ingested orally; sometimes insufflated or dissolved in liquid
- Typical recreational dose: 75-125 mg
- Widely used at raves, clubs, music festivals; enhances music, dancing, social bonding
Intoxication / Clinical Features
Desired effects (low-moderate dose):
- Euphoria and emotional closeness/empathy ("entactogenic")
- Heightened sensory perception - music, touch especially pleasurable
- Increased energy, sociability, sense of well-being
- Mild hallucinations and perceptual distortions
- Increased heart rate and blood pressure
Adverse/toxic effects:
- Hyperthermia - potentially life-threatening (most dangerous acute effect, especially in hot/crowded environments with dancing)
- Tachycardia, hypertension
- Diaphoresis, dehydration
- Bruxism and trismus (jaw clenching/teeth grinding) - characteristic
- Dry mouth
- Nausea
- Mydriasis
- Hyponatremia - SIADH-like syndrome from excessive water intake + ADH hypersecretion; can cause cerebral edema (more common in females)
- Serotonin syndrome - with concomitant use of serotonergic drugs (SSRIs, MAOIs); features: hyperthermia + clonus + altered mental status
- Rhabdomyolysis (from hyperthermia + excessive motor activity)
- Cardiac dysrhythmias
- Seizures (at high doses or hyperthermia)
Dependence
- MDMA produces primarily psychological dependence rather than physical dependence
- Tolerance develops rapidly with repeated use (rapidly diminishing effects)
- Post-MDMA "comedown" / withdrawal:
- Occurs 1-2 days after use (consistent with serotonin depletion)
- Depression, fatigue, irritability, poor concentration ("mid-week blues")
- Insomnia
- Anxiety, reduced sociability
- More severe depression, irritability, and unsociability than alcohol withdrawal (study data)
- Duration typically 1-5 days
Neurotoxicity
- Repeated MDMA use causes selective, long-lasting damage to serotonergic nerve terminals (demonstrated in animals)
- In humans: associated with cognitive deficits, memory impairment (potentially permanent with heavy use)
- Metabolized (in part) to MDA, which has greater neurotoxic potential
Acute Treatment of Intoxication
- Temperature management is the top priority - hyperthermia is the main killer
- Move to cool environment
- Tepid water misting, ice packs
- Aggressive cooling measures
- Benzodiazepines (IV diazepam/lorazepam) - reduce agitation, help with cooling, control seizures
- Life-threatening hyperthermia: neuromuscular blockers + endotracheal intubation to control excessive movement and heat generation
- Cyproheptadine (serotonin antagonist) for serotonin syndrome - note: only available orally, limits use in severe cases
- Correct hyponatremia carefully (hypertonic saline if severe/symptomatic; avoid overrapid correction)
- Cardiac monitoring
- Rhabdomyolysis: IV fluids, urine alkalinization
- Do NOT give extra water to hyperthermic patients without checking sodium first (risk of worsening hyponatremia)
Treatment of Withdrawal / Dependence
- No approved pharmacotherapy for MDMA use disorder
- Supportive care for the comedown period
- Short-term sleep aids if needed (non-BZD, avoid dependence)
- SSRIs: theoretically might help serotonin depletion but clinical evidence limited
- CBT for relapse prevention
- Neuropsychological monitoring for long-term cognitive effects
DRUG 5: METHAMPHETAMINE (as Club Drug)
Introduction
Methamphetamine is a synthetic psychostimulant that appears in the club drug context as "crystal meth," "tina," "ice." In chemsex contexts (sex on drugs), it is often co-used with GHB/GBL. Street names: meth, crystal, tina, ice, speed, glass. - Maudsley Guidelines 15e
Mechanism
Releases dopamine, norepinephrine, and serotonin from presynaptic terminals; inhibits reuptake; acts longer and more potently than cocaine. Unlike cocaine, rapidly crosses the blood-brain barrier.
Intoxication Features
- Euphoria, increased energy, decreased appetite
- Tachycardia, hypertension, hyperthermia
- Diaphoresis, flushing, mydriasis
- Bruxism, skin picking ("tweaking"), formication
- Tooth decay ("meth mouth") from dry mouth + bruxism + poor hygiene
- Paranoia, psychosis (hallucinations, persecutory delusions)
Methamphetamine Psychosis
- Psychotic symptoms in ~25% of users persist 1 month after use
- Between 16-38% of patients initially diagnosed with methamphetamine psychosis are later diagnosed with schizophrenia
- Indistinguishable from primary psychotic disorder when persistent
- Treatment: Benzodiazepines for acute agitation; olanzapine or aripiprazole if antipsychotics needed. Note: fourfold increased risk of EPSEs in methamphetamine users. - Maudsley Guidelines 15e
Withdrawal
- Low mood, listlessness, fatigue, irritability, hypersomnia
- Intense craving
- Generally not life-threatening (unlike GHB/BZD)
Treatment
- Mirtazapine: 2022 systematic review and meta-analysis showed reduction in methamphetamine consumption in meth use disorder
- CBT (most evidence-based psychosocial intervention)
- Contingency management
- No approved pharmacotherapy in US/EU
DRUG 6: LSD (Lysergic Acid Diethylamide)
Introduction
LSD is a potent synthetic hallucinogen derived from ergot alkaloids. Although less commonly associated with date rape, it is included in the club drug category. It is odorless, colorless, with a slightly bitter taste. - Kaplan & Sadock's
Street Names
- Acid, Blotter, Tabs
- Trips, Dots, Lucy
Mechanism
Primarily a serotonin 5-HT2A receptor agonist in the cortex. This disrupts normal sensory processing and produces hallucinations.
Clinical Features
- Visual hallucinations and perceptual distortions (dose-dependent)
- Synesthesia (cross-sensory experiences)
- Emotional lability, paranoia at high doses
- Panic reactions ("bad trips")
- Effects last 8-12 hours
- No physiological dependence
- Tolerance develops rapidly (requires escalating doses)
- Flashbacks (HPPD - Hallucinogen Persisting Perception Disorder): occur up to 1 year after use
Acute Treatment
- Quiet, low-stimulation "talk-down" environment
- Benzodiazepines for severe agitation or panic
- Antipsychotics (haloperidol) for extreme cases
- No specific antidote
DRUG 7: CHLORAL HYDRATE ("Mickey Finn")
Introduction
Historically used as a "knockout drop" - the original "Mickey Finn." When combined with ethanol, they produce rapid unconsciousness. Occasionally still prescribed for procedural sedation. - Rosen's Emergency Medicine
Mechanism
Metabolized by alcohol dehydrogenase to trichloroethanol, which acts on GABA-A receptors (barbiturate-like). Chloral hydrate and ethanol potentiate each other - chloral hydrate increases ethanol half-life by competing for alcohol dehydrogenase.
Clinical Features
- CNS and respiratory depression
- Cardiovascular toxicity (hallmark): sensitizes myocardium to catecholamines; ventricular tachycardia/fibrillation, torsades de pointes, atrial fibrillation
- GI irritation (esophagitis, hemorrhagic gastritis)
- Citrus/pear-like odor to breath
- Toxic dose: ~10 g in adults; potentially fatal cardiac dysrhythmia
Treatment
- Supportive: airway management
- Dysrhythmias: short-acting beta-blocker (propranolol/esmolol) - NOT epinephrine (sensitized myocardium)
- Avoid naloxone
- Hemodialysis for severe toxicity (trichloroethanol is dialyzable)
SUMMARY TABLE: CLINICAL COMPARISON
| Feature | GHB | Rohypnol | Ketamine | MDMA |
|---|---|---|---|---|
| Class | CNS depressant | Benzodiazepine | Dissociative anesthetic | Entactogen-stimulant |
| Mechanism | GHB-R + GABA-B | GABA-A (BZD site) | NMDA antagonist | Serotonin release/reuptake block |
| Onset | 15-30 min | 20-30 min | 15-30 min (intranasal) | 30-60 min |
| Duration | 1.5-6 hours | 8-48 hours | 30-60 min | 3-5 hours |
| Amnesia | Yes (profound) | Yes (profound) | Yes | Partial |
| Detectability (routine screen) | No | No | No | Usually No |
| Life-threatening withdrawal | YES | YES | No | No |
| Key toxicity | Respiratory depression, coma | Respiratory depression, coma | Emergence agitation, cystitis | Hyperthermia, hyponatremia, serotonin syndrome |
| Antidote | None | Flumazenil (with caution) | None | None (cyproheptadine for SS) |
DETECTION AND FORENSIC ASPECTS
- GHB, flunitrazepam, and ketamine are not detected on routine ED toxicology screening (Tintinalli's Emergency Medicine)
- GHB has a very short half-life (~30-60 min) - urine/serum must be collected within 4-8 hours of suspected ingestion
- Flunitrazepam metabolites detectable in urine up to 72 hours with specialized testing
- MDMA may appear on amphetamine screens but false negatives occur
- Urine sample preservation crucial: refrigerate at 4°C, freeze if >72 hours
- In suspected drug-facilitated sexual assault: contact police crime laboratory for specialized testing
- Hair analysis (hair strands) can detect drugs weeks to months later - increasingly used in forensic cases
RECENT ADVANCES (2023-2026)
-
GHB withdrawal - pharmaceutical GHB tapering: A matched-subject observational study (Belgium/Netherlands, published in CNS Drugs 2020, ongoing real-world use post-2022) showed pharmaceutical GHB tapering is non-inferior to benzodiazepine tapering for GHB-dependent patients, with potentially fewer complications. The Dutch GHB Monitor Project continues to refine protocols. (Maudsley Guidelines 15e reference: Beurmanjer H et al.)
-
Phenobarbital for severe GHB withdrawal: A 2023 case series (Freeman et al., Drug Alcohol Rev 2023) documented successful use of phenobarbital for managing severe GHB withdrawal refractory to benzodiazepines - adding an important option to the armamentarium.
-
MDMA-assisted psychotherapy: MDMA was under late-stage clinical trials for PTSD (Phase 3 MAPS trials). The FDA issued a Complete Response Letter in August 2024 citing concerns about trial design - not yet approved, but ongoing research continues. Promising signals in combat veterans and sexual assault survivors.
-
Esketamine (Spravato): The S-enantiomer of ketamine, approved by FDA (2019) for treatment-resistant depression and major depression with acute suicidal ideation. Administered intranasally under supervised clinical settings. Creates new considerations around ketamine's medical vs. illicit use.
-
New designer drugs / novel psychoactive substances (NPS): Bath salts (synthetic cathinones like MDPV, mephedrone, methylone) continue to emerge as club drugs. MDPV (methylenedioxypyrovalerone) is a particularly potent synthetic stimulant. Forensic medicine 36e (2026) highlights detection challenges for NPS.
-
Medetomidine contamination (2026): A 2026 review (Annals of Emergency Medicine) documented emergence of medetomidine (a veterinary alpha-2 agonist) in the illicit drug supply - implications for emergency care and withdrawal management, representing a new threat.
-
Drug checking services: Harm reduction programs now offer real-time drug testing at festivals/venues (e.g., fentanyl test strips, reagent kits, mass spectrometry). Evidence supports reduction in high-risk drug use when people know what substances are present.
-
Liquid GHB testing strips: Development of colorimetric point-of-care GHB test strips for drinks has advanced - though sensitivity/specificity remains imperfect.
KEY POINTS FOR CLINICAL PRACTICE
- Assume co-ingestion - most date rape scenarios involve multiple drugs plus alcohol
- GHB and flunitrazepam are invisible on routine drug screens - clinical suspicion must drive management
- GHB withdrawal can kill - recognize it, treat aggressively with high-dose benzodiazepines ± baclofen
- MDMA hyperthermia is the leading cause of death - aggressive cooling is the priority
- Ketamine cystitis is an underrecognized serious complication of chronic use
- Forensic evidence collection is time-critical: collect blood and urine immediately in suspected sexual assault; contact specialist labs
- Psychological trauma from drug-facilitated assault is profound - forensic exam + psychological support + legal referral are all part of care
- Adulteration is rampant - "Molly" or "ecstasy" bought on the street may contain fentanyl, methamphetamine, PMMA, or synthetic cathinones that are far more dangerous
- Kaplan & Sadock's Synopsis of Psychiatry, p. 688-689
- Rosen's Emergency Medicine 10e, pp. 3060-3061, 3186-3190
- Maudsley Prescribing Guidelines in Psychiatry, 15th ed., pp. 537-564
- Lippincott Illustrated Reviews: Pharmacology, p. 1554-1555
- Stahl's Essential Psychopharmacology, pp. 461-462
- Tintinalli's Emergency Medicine, p. 2182
- Forensic Medicine & Toxicology 36th ed. (2026), pp. 170-194, 9461-9522
- Dermatology 5e, p. 3730
This is a shared conversation. Sign in to Orris to start your own chat.