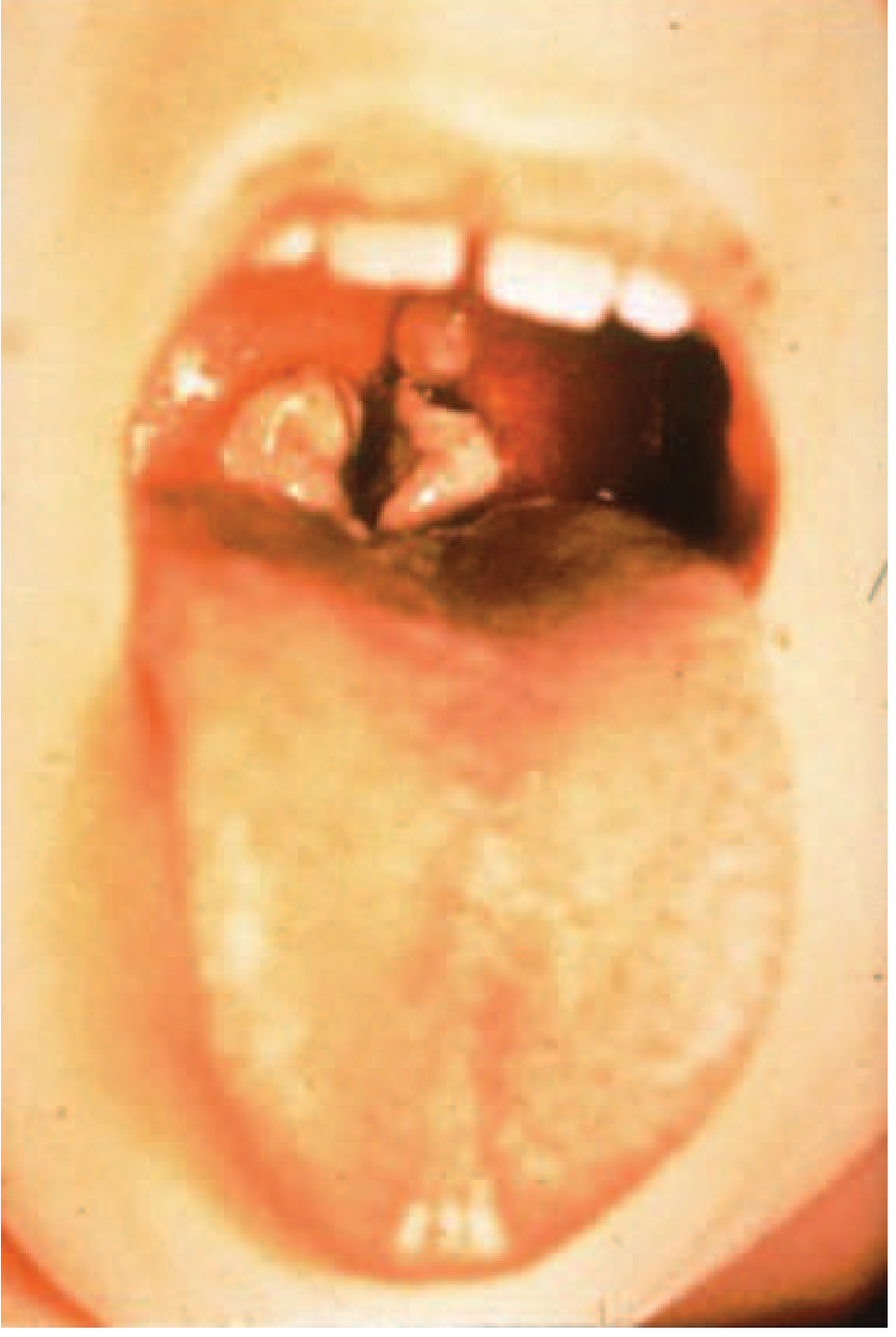
Pseudo membrane formation in Diphtheria
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive, high-quality information from multiple authoritative sources. Here is a detailed synthesis:
Pseudomembrane Formation in Diphtheria
The Organism
Diphtheria is caused by Corynebacterium diphtheriae, a non-motile, gram-positive pleomorphic bacillus. The pseudomembrane is the hallmark of the disease and forms only in infections by toxin-producing (tox+) strains. Non-toxigenic strains can colonize the nasopharynx or skin but do not produce pseudomembranes or systemic toxic effects.
- Jawetz Melnick & Adelberg's Medical Microbiology, p. 203
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery
Step-by-Step Mechanism of Pseudomembrane Formation
1. Bacterial Implantation and Toxin Production
After inhalation (incubation period 2-5 days, range 1-10 days), C. diphtheriae implants on the mucosa of the upper respiratory tract. The organism does not invade deep tissues and practically never enters the bloodstream. Instead, it rapidly multiplies locally and elaborates diphtheria toxin - a 535-amino acid single-chain protein that is the primary virulence factor.
2. Diphtheria Toxin Mechanism
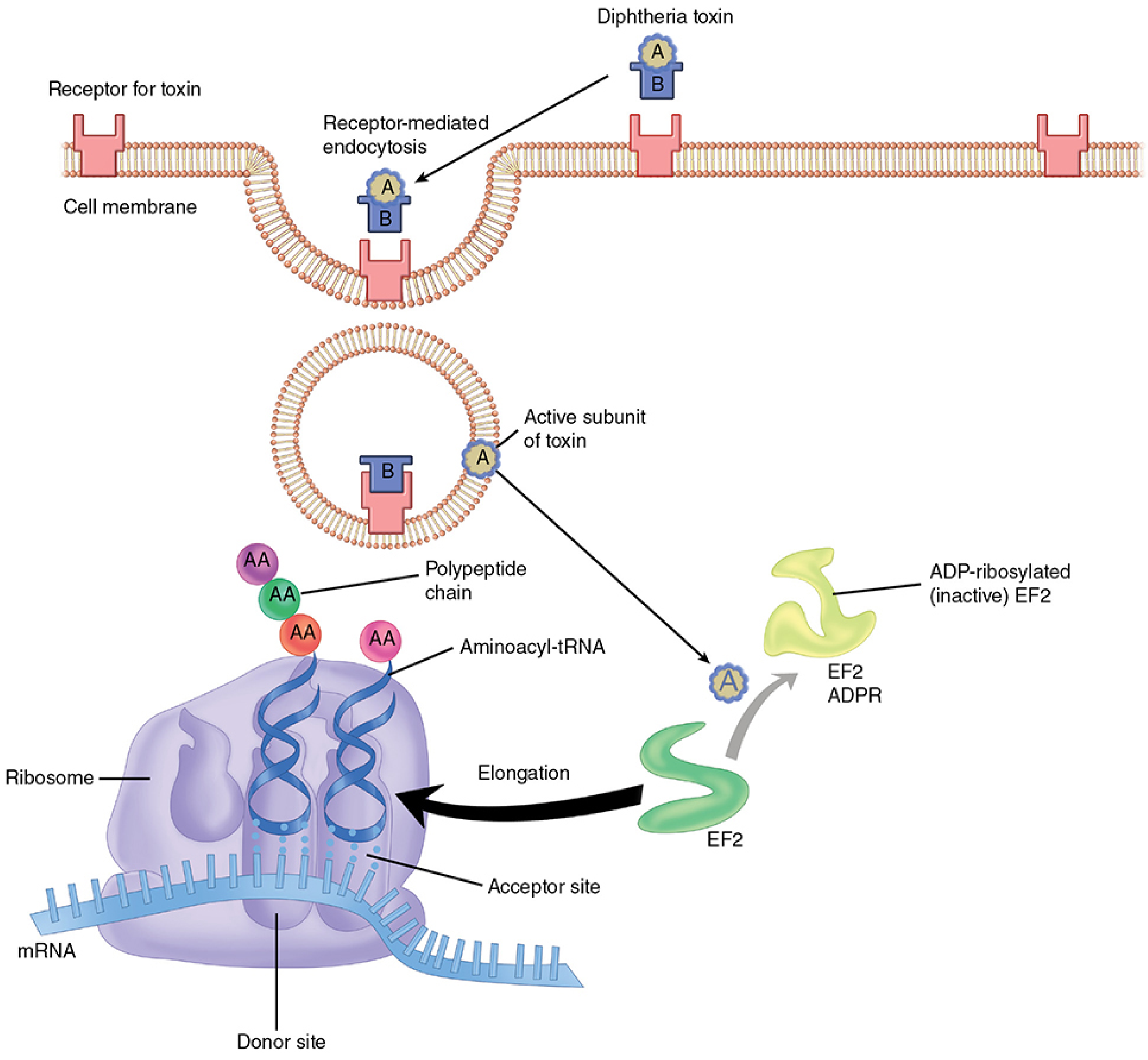
The toxin has two functional fragments:
- Fragment B (binding): Binds to the heparin-binding epidermal growth factor-like precursor receptor on the host cell surface; mediates receptor-mediated endocytosis
- Fragment A (active): Released into the cytosol from an acidified early endosomal compartment; catalyzes NAD+-dependent ADP-ribosylation of Elongation Factor 2 (EF-2), permanently inactivating it
This halts ribosomal protein synthesis, leading to irreversible cell death.
- Harrison's Principles of Internal Medicine 22E (2025), p. 1266
- Sherris & Ryan's Medical Microbiology, p. 46
3. Epithelial Necrosis
Diphtheria toxin is absorbed directly into the mucous membranes of the respiratory epithelium. The resulting inhibition of protein synthesis causes necrosis of the mucosal epithelial layer accompanied by:
- Submucosal edema
- Hyperemia
- Vascular congestion of the submucosal base
This creates mucosal ulcers at the site of infection.
- Harrison's Principles of Internal Medicine 22E (2025), p. 1266
4. Fibrinopurulent Exudate Formation
The necrotic epithelium triggers a brisk inflammatory response. From the ulcerated base, a significant fibrinopurulent (fibrinous + purulent) exudate is produced:
- The necrotic epithelial cells become embedded in exuding fibrin
- Red blood cells (erythrocytes) and white blood cells (neutrophils) are incorporated into the fibrin mesh
- This entire combination coagulates to form the pseudomembrane
The structural result is:
"Mucosal ulcers with a pseudomembranous coating composed of an inner band of fibrin and a luminal band of neutrophils."
- Harrison's Principles of Internal Medicine 22E (2025)
Gross Appearance and Evolution
| Feature | Description |
|---|---|
| Initial appearance | White or whitish, may wipe off easily in very early disease |
| Established membrane | Thick, grayish-white, sharply demarcated |
| Advanced/severe disease | Turns gray, then green or black as necrosis progresses |
| Adherence | Tightly adherent to the underlying mucosa - unlike streptococcal exudate |
| Bleeding on removal | Attempting to remove it tears the underlying capillaries and causes bleeding |
| Progression | May actually increase in size after first noted |
- Harrison's Principles of Internal Medicine 22E (2025)
- Goldman-Cecil Medicine
- Park's Textbook of Preventive & Social Medicine
Composition of the Pseudomembrane
The pseudomembrane is not truly a membrane - it has no epithelial lining of its own. It consists of:
- Necrotic epithelial cells
- Fibrin (inner band, anchors it to the underlying ulcerated submucosa)
- Neutrophils (luminal band)
- Red blood cells
- Living and dead C. diphtheriae bacilli (which continue to produce toxin within the membrane)
The organisms within the membrane continue to actively produce toxin, which is then absorbed into the bloodstream and carried to distant organs (heart, nerves, kidneys, adrenals).
- Jawetz Melnick & Adelberg's Medical Microbiology, p. 202
- Park's Textbook of Preventive & Social Medicine
Location and Spread
The pseudomembrane typically begins in the tonsillopharyngeal region and can extend to:
| Site | Form | Features |
|---|---|---|
| Tonsillopharyngeal | Most common (~80% of respiratory cases) | Grayish, adherent, bleeds on removal |
| Nasal | Mildest form | Serosanguinous/purulent discharge; may extend to pharynx |
| Laryngeal | Hoarseness, croupy cough | Can be confused with viral croup |
| Tracheobronchial | Most severe; usually by secondary spread | Can extend into medium-sized bronchi |
In approximately 80% of untreated symptomatic cases, membranous diphtheria develops 2-3 days after the onset of prodromal symptoms.
- Goldman-Cecil Medicine, p. 3067
- Harrison's Principles of Internal Medicine 22E (2025)
Why the Pseudomembrane is Dangerous
- Airway obstruction: Expanding or sloughing membranes can cause fatal obstruction. The laryngeal membrane in particular can cause suffocation if not relieved by intubation or tracheotomy.
- Toxin absorption: The bacilli within the membrane continue producing toxin, which is absorbed and causes systemic toxicity:
- Myocarditis (most common; in up to 25-35% of cases; arrhythmias, heart block, ventricular tachycardia)
- Neuropathy: Demyelination causing palatal palsy, oculomotor palsies, peripheral motor neuropathy
- Parenchymal damage to liver, kidneys (tubular necrosis), and adrenal glands
- "Bull-neck" diphtheria: Massive cervical lymphadenopathy + submucosal edema, indicating severe disease with high toxin load
- Robbins & Kumar Basic Pathology, p. 493
- Goldman-Cecil Medicine
Key Distinguishing Feature from Other Exudates
| Feature | Diphtheria Pseudomembrane | Streptococcal Exudate |
|---|---|---|
| Adherence | Tightly adherent to mucosa | Loosely adherent, easily wiped off |
| Bleeding on removal | Yes - bleeds | No significant bleeding |
| Extent | Can extend beyond tonsils | Usually limited to tonsils |
| Color | Gray-white to gray-green/black | White-yellow |
| Systemic toxicity | Severe (myocarditis, neuropathy) | Post-streptococcal sequelae |
- Harrison's Principles of Internal Medicine 22E (2025)
Clinical Diagnosis
The CDC defines confirmed respiratory diphtheria as laboratory-proven or epidemiologically linked to a culture-confirmed case. The presence of a classic pharyngeal pseudomembrane alone is sufficient evidence to begin immediate treatment - specific treatment must never be delayed for laboratory confirmation.
Diagnosis requires:
-
Sore throat + adherent tonsillopharyngeal/nasal pseudomembranous lesions + low-grade fever
-
Isolation of C. diphtheriae on Löffler's or tellurite selective medium (inoculated from submembranous swabs)
-
Antitoxin + antibiotics (to kill bacteria and halt toxin production)
-
Jawetz Melnick & Adelberg's Medical Microbiology
-
Harrison's Principles of Internal Medicine 22E (2025)
This is a shared conversation. Sign in to Orris to start your own chat.