Hmp shunt pathway
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Here is a thorough overview of the HMP shunt (Hexose Monophosphate Shunt), also called the Pentose Phosphate Pathway (PPP), drawn from Lippincott's Illustrated Reviews: Biochemistry and Basic Medical Biochemistry (6e).
HMP Shunt (Hexose Monophosphate Shunt / Pentose Phosphate Pathway)
Overview
The pentose phosphate pathway runs parallel to glycolysis in the cytosol. It does not produce ATP. Its two main outputs are:
- NADPH - a reducing agent needed for reductive biosynthesis and antioxidant defense
- Ribose 5-phosphate - required for nucleotide and nucleic acid synthesis
All cells run this pathway, but it is especially active in:
- Liver, lactating mammary glands, adipose tissue (fatty acid synthesis)
- Testes, ovaries, placenta, adrenal cortex (steroid hormone synthesis)
- Red blood cells (protection from oxidative stress)
The pathway has two phases: an irreversible oxidative phase and a reversible nonoxidative phase.
Phase 1: Oxidative Phase (Irreversible)
Three reactions convert glucose 6-phosphate to ribulose 5-phosphate, generating 2 NADPH and releasing 1 CO₂ per glucose 6-phosphate.
| Step | Enzyme | Reaction | Product |
|---|---|---|---|
| 1 | Glucose 6-phosphate dehydrogenase (G6PD) | Glucose 6-P + NADP⁺ → 6-Phosphogluconolactone + NADPH | 6-Phosphogluconolactone |
| 2 | 6-Phosphogluconolactone hydrolase | Hydrolysis | 6-Phosphogluconate |
| 3 | 6-Phosphogluconate dehydrogenase | 6-Phosphogluconate + NADP⁺ → Ribulose 5-P + CO₂ + NADPH | Ribulose 5-phosphate |
Key regulatory point: G6PD catalyzes the committed, rate-limiting step. It is inhibited by NADPH (product inhibition). When NADPH is consumed (e.g., during oxidative stress), NADPH/NADP⁺ ratio drops, relieving inhibition and increasing flux. Insulin upregulates G6PD gene expression.
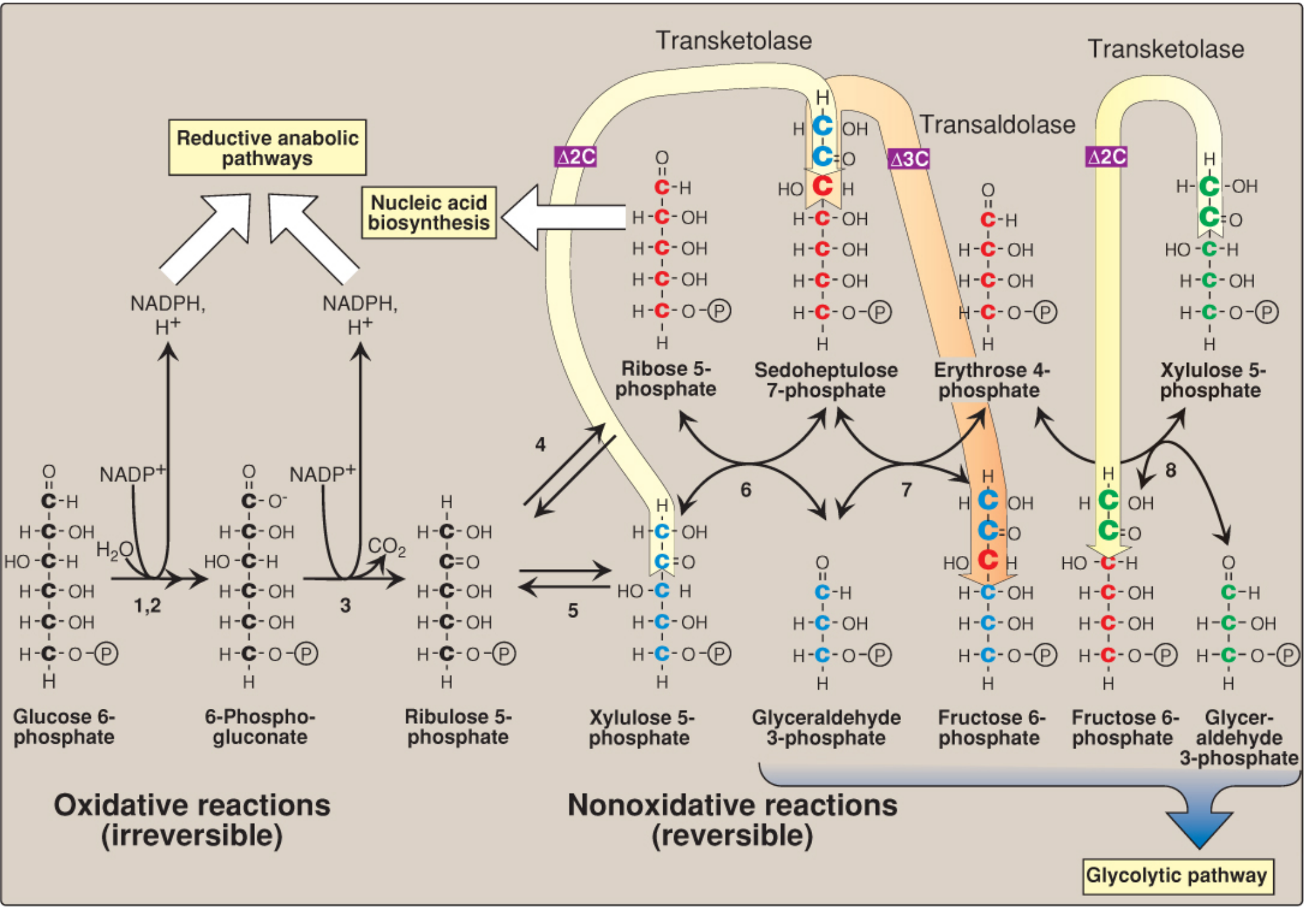
Phase 2: Nonoxidative Phase (Reversible)
Ribulose 5-phosphate is converted into other sugars depending on what the cell needs. The key enzymes are:
- Ribose 5-phosphate isomerase - converts ribulose 5-P → ribose 5-P (for nucleotide synthesis)
- Phosphopentose epimerase - converts ribulose 5-P → xylulose 5-P
- Transketolase (requires Thiamine Pyrophosphate/TPP) - transfers 2-carbon units from a ketose to an aldose (steps 6 and 8 in the diagram)
- Transaldolase - transfers 3-carbon units (step 7 in the diagram)
The net result of the nonoxidative phase feeds intermediates back into glycolysis as fructose 6-phosphate and glyceraldehyde 3-phosphate.
The interconversions can be summarized as:
5C + 5C → 7C + 3C (transketolase) → 4C + 6C (transaldolase) → 5C + 6C (transketolase)
Direction of the nonoxidative phase depends on cellular needs:
| Cell Need | Direction |
|---|---|
| More ribose 5-P than NADPH | Glycolytic intermediates → ribose 5-P (reverse) |
| More NADPH than ribose 5-P | Ribulose 5-P → glycolytic intermediates (forward) |
| Need both | Oxidative phase runs fully |
Overall Equation
3 Glucose 6-P + 6 NADP⁺ → 3 CO₂ + 6 NADPH + 2 Fructose 6-P + Glyceraldehyde 3-P
Compared to glycolysis (3 glucose 6-P → 6 NADH + 9 ATP + 6 pyruvate), the HMP shunt yields 6 NADPH, 3 CO₂, 5 NADH, 8 ATP, and 5 pyruvate when intermediates flow onward through glycolysis.
Role of NADPH
NADPH is used for:
- Fatty acid and cholesterol synthesis (liver, adipose)
- Steroid hormone synthesis (adrenal cortex, gonads)
- Reduction of glutathione (all cells, especially RBCs)
- Cytochrome P450 reactions (hydroxylation reactions)
- NADPH oxidase in phagocytes for respiratory burst (killing microbes)
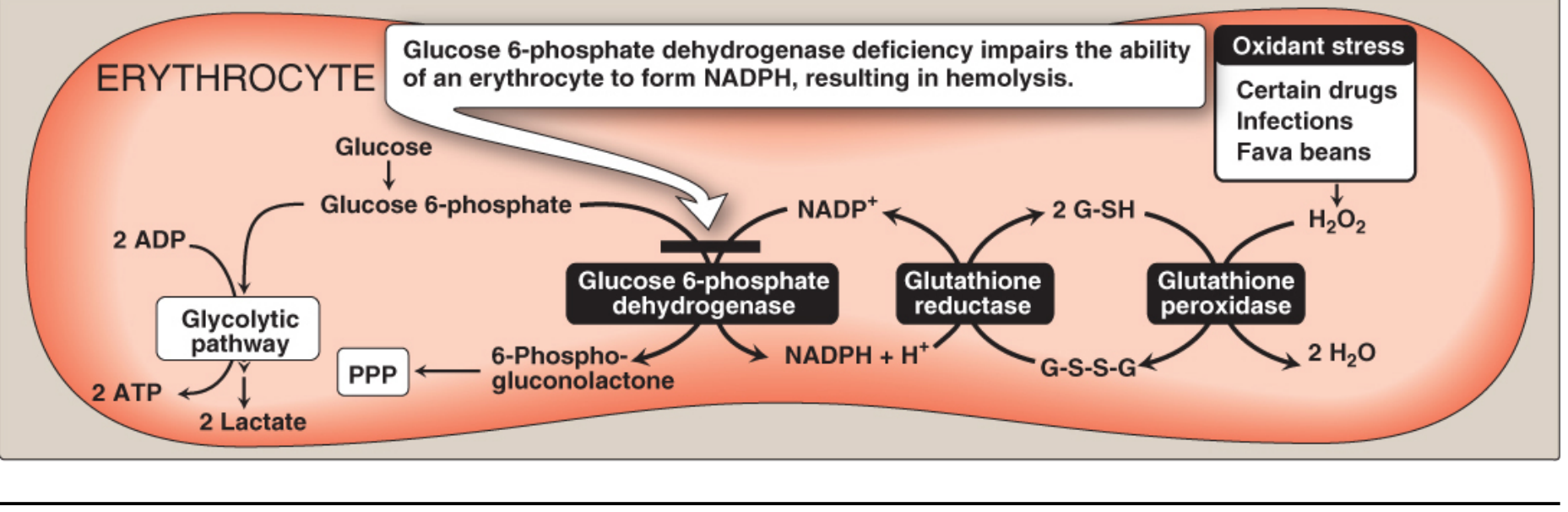
In RBCs, the HMP shunt is the only source of NADPH. NADPH regenerates reduced glutathione (G-SH) via glutathione reductase, which then neutralizes H₂O₂ via glutathione peroxidase.
Clinical Significance: G6PD Deficiency
- Inheritance: X-linked recessive (affects mostly males)
- Prevalence: >400 million people worldwide; highest in Middle East, tropical Africa/Asia, Mediterranean
- Mechanism: Lack of G6PD → reduced NADPH → depleted reduced glutathione → RBCs cannot neutralize oxidants → oxidative damage to hemoglobin (Heinz bodies) and RBC membrane → hemolytic anemia
- Why RBCs are uniquely vulnerable: RBCs have no nucleus/ribosomes, so they cannot replenish G6PD; and the HMP shunt is their only source of NADPH
Precipitating factors (oxidant stressors):
- Drugs: primaquine, dapsone, sulfonamides, nitrofurantoin
- Foods: fava beans (favism - divicine and isouramil)
- Infections
Clinical features:
- Hemolytic anemia (episodic)
- Neonatal jaundice (1-4 days after birth)
- Bite cells, Heinz bodies on blood smear
- Splenomegaly, pigmented gallstones (chronic cases)
Evolutionary benefit: G6PD deficiency confers resistance to Plasmodium falciparum malaria - oxidant stress from the parasite causes preferential lysis of infected RBCs.
Thiamine (Vitamin B1) Connection
Transketolase requires thiamine pyrophosphate (TPP) as a cofactor. In thiamine deficiency, transketolase activity falls. Measuring RBC transketolase activity (with and without added TPP) is a classic test for diagnosing thiamine deficiency (beriberi).
Sources: - Biochemistry, 8th ed., Lippincott Illustrated Reviews, p. 424-434; - Basic Medical Biochemistry: A Clinical Approach, 6e, p. 959-965; - Goldman-Cecil Medicine, p. 1701
This is a shared conversation. Sign in to Orris to start your own chat.