explaun me 10 commomheart diseases with ECG changes and ECG images
Reading File
Finding Sources
Finding Sources
Searching Images
ECG changes myocardial infarction ST elevation
Searching Images
atrial fibrillation ECG irregular rhythm absent P waves
Searching Images
left ventricular hypertrophy ECG high voltage criteria
Searching Images
complete heart block third degree AV block ECG
Finding Sources
Finding Sources
Searching Images
Wolff-Parkinson-White syndrome ECG delta wave short PR
Searching Images
pulmonary embolism ECG S1Q3T3 right heart strain sinus tachycardia
Searching Images
ventricular tachycardia ECG wide complex tachycardia
Searching Images
pericarditis ECG diffuse ST elevation PR depression
Searching Images
hyperkalemia ECG peaked T waves wide QRS sine wave
Searching Images
dilated cardiomyopathy ECG low voltage bundle branch block poor R wave progression
I now have comprehensive ECG images for all 10 conditions. Let me compile the full educational response.
10 Common Heart Diseases with ECG Changes
1. ST-Elevation Myocardial Infarction (STEMI)
Pathophysiology: Complete occlusion of a coronary artery → transmural ischemia → progressive myocyte necrosis.
ECG Changes:
- Hyperacute T-waves (earliest sign — tall, broad, peaked)
- ST-segment elevation ≥1 mm in ≥2 contiguous limb leads, or ≥2 mm in ≥2 contiguous precordial leads (convex/"tombstone" morphology)
- Reciprocal ST depression in opposing leads
- Pathological Q waves (>40 ms wide, >25% of R-wave height) — develop within hours to days indicating necrosis
- T-wave inversion in the evolving/resolving phase
Territory localization:
| Territory | Leads with STE | Culprit artery |
|---|---|---|
| Anterior | V1–V4 | LAD |
| Lateral | I, aVL, V5–V6 | LCx |
| Inferior | II, III, aVF | RCA |
| Posterior | Tall R + ST↓ in V1–V3 | RCA/LCx |

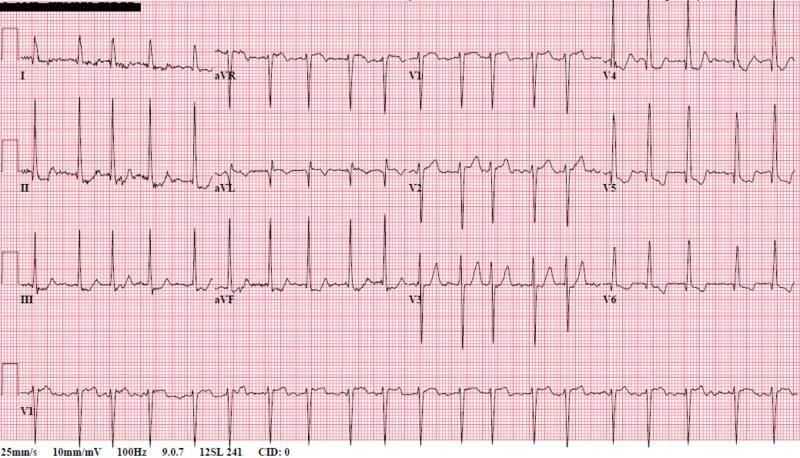
2. Atrial Fibrillation (AF)
Pathophysiology: Disorganized electrical activity in the atria replaces coordinated sinus node depolarization, producing chaotic atrial activation and irregularly irregular ventricular conduction.
ECG Changes:
- Absent P waves — replaced by fine fibrillatory (f) waves best seen in V1
- Irregularly irregular R-R intervals (hallmark finding)
- Narrow QRS complexes (unless aberrant conduction or bundle branch block)
- Rate varies: controlled (<100 bpm), rapid ventricular response (>100 bpm), or slow (in nodal disease)
3. Complete (Third-Degree) AV Block
Pathophysiology: Total failure of conduction through the AV node or His-Purkinje system → complete atrioventricular dissociation. The ventricles are driven by a slow escape rhythm.
ECG Changes:
- Complete AV dissociation — P waves and QRS complexes march independently
- Regular P-P intervals at a faster atrial rate
- Regular R-R intervals at a slower ventricular escape rate (20–40 bpm if ventricular; 40–60 bpm if junctional)
- Wide QRS (>120 ms) if infra-Hisian escape; narrow QRS if junctional escape
- No consistent PR interval — P waves appear before, within, or after QRS complexes
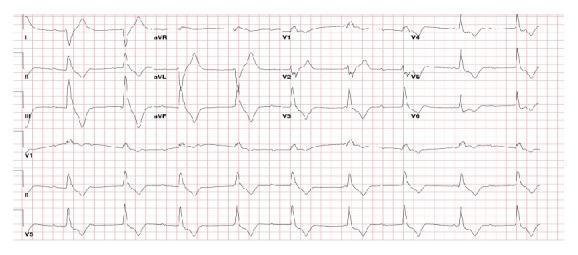
4. Acute Pericarditis
Pathophysiology: Inflammation of the pericardium → epicardial irritation → diffuse myocardial surface injury current. Evolves through 4 ECG stages over weeks.
ECG Changes (Stage I — acute):
- Diffuse concave ("saddle-shaped") ST elevation in all leads except aVR and V1
- PR-segment depression in most leads (very specific — reflects atrial injury)
- PR elevation in aVR (reciprocal)
- Spodick's sign — downsloping TP segment
- No reciprocal ST depression (unlike STEMI) — key distinguishing feature
Key differentiator from STEMI: Diffuse distribution across multiple vascular territories; concave (not convex) ST morphology; PR depression.

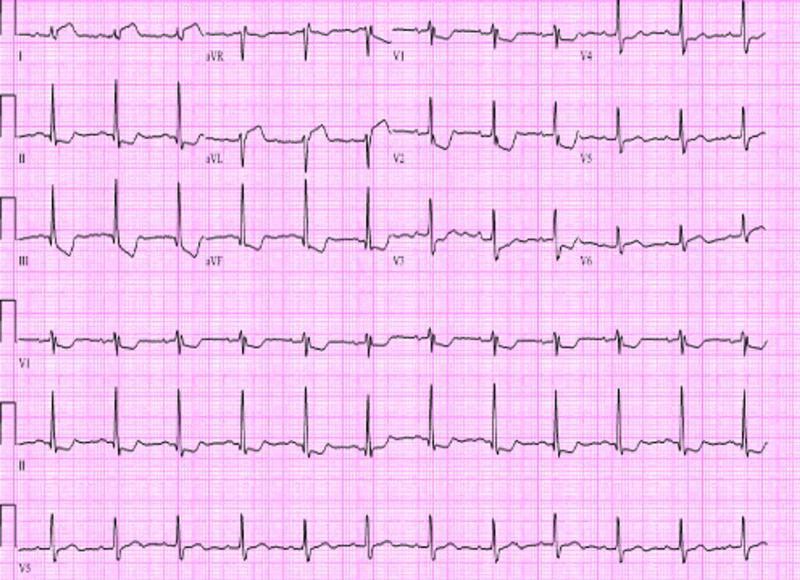
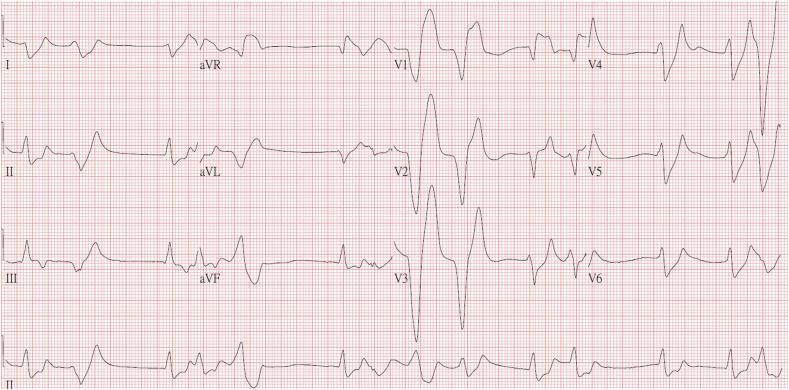
5. Left Ventricular Hypertrophy (LVH)
Pathophysiology: Chronic pressure or volume overload (hypertension, aortic stenosis) → concentric or eccentric hypertrophy → increased myocardial mass → greater electrical voltage.
ECG Changes:
- High QRS voltage: Sokolow-Lyon criteria: S in V1 + R in V5 or V6 ≥35 mm; Cornell criteria: R in aVL + S in V3 >28 mm (men), >20 mm (women)
- Left axis deviation
- "Strain pattern": ST depression + T-wave inversion in lateral leads (I, aVL, V5–V6) — indicates subendocardial ischemia from increased oxygen demand
- Prolonged QRS duration (not frank LBBB)
- Left atrial enlargement (P mitrale — broad, notched P in II)
6. Pulmonary Embolism (PE)
Pathophysiology: Acute pulmonary arterial obstruction → sudden rise in right ventricular afterload → right ventricular strain and dilation → clockwise cardiac rotation.
ECG Changes (most common: sinus tachycardia ± non-specific ST-T changes):
- Sinus tachycardia (most frequent finding)
- S1Q3T3 pattern (McGinn-White sign): Deep S wave in lead I + Q wave in lead III + T-wave inversion in lead III
- Right bundle branch block (complete or incomplete)
- T-wave inversions V1–V4 (right ventricular strain)
- Right axis deviation
- P pulmonale (peaked P in II — right atrial enlargement)
- Low voltage if massive PE
Note: The classic S1Q3T3 is present in only ~20% of PE cases. Sinus tachycardia alone is the most common finding.

7. Wolff-Parkinson-White (WPW) Syndrome
Pathophysiology: Congenital accessory pathway (Bundle of Kent) bypasses the AV node → pre-excitation of the ventricle occurs before the normal His-Purkinje system fires → delta wave and short PR. Risk of life-threatening arrhythmias (AF with rapid conduction through the accessory pathway).
ECG Changes (sinus rhythm — pre-excitation pattern):
- Short PR interval (<120 ms)
- Delta wave — slurred, slow upstroke at the onset of QRS
- Widened QRS (>120 ms) due to fusion of pre-excited and normally conducted beats
- Secondary ST-T changes (discordant to the delta wave/QRS)
- "Pseudo-infarction" Q waves in inferior leads with negative delta waves (type B pattern)
Accessory pathway localization by delta wave polarity in limb and precordial leads.

8. Ventricular Tachycardia (VT)
Pathophysiology: Rapid ventricular depolarization originating below the His bundle — most commonly from re-entry circuits around myocardial scar (ischemic cardiomyopathy), triggered activity, or abnormal automaticity.
ECG Changes:
- Wide QRS complex tachycardia (>120 ms) at rate >100 bpm (usually 140–220 bpm)
- AV dissociation — P waves visible but independent of QRS (pathognomonic when present)
- Fusion beats and capture beats (confirms AV dissociation)
- Positive or negative QRS concordance across precordial leads
- QRS axis: Northwest axis (−90° to ±180°) strongly suggests VT
- Brugada criteria and Vereckei criteria used to differentiate from SVT with aberrancy

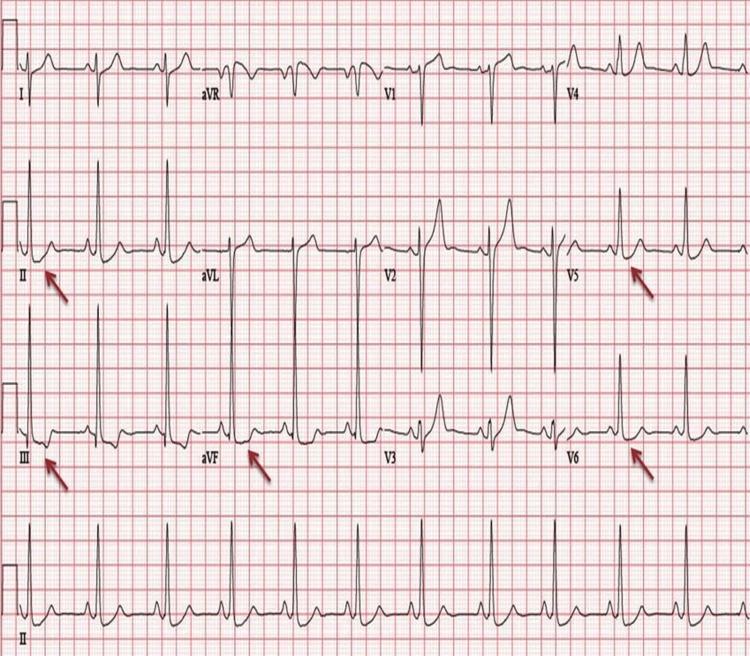
9. Hyperkalemia
Pathophysiology: Elevated extracellular potassium depolarizes resting membrane potential → progressive conduction slowing → fatal arrhythmias if untreated. ECG evolves with rising K⁺ levels.
ECG Changes (progressive with rising K⁺):
| Serum K⁺ | ECG Change |
|---|---|
| 5.5–6.5 mEq/L | Tall, narrow-based, peaked ("tented") T waves — earliest sign |
| 6.5–7.5 mEq/L | PR prolongation, P-wave flattening/disappearance |
| 7.5–8.5 mEq/L | QRS widening (intraventricular conduction delay) |
| >8.5 mEq/L | Sine-wave pattern (QRS and T merge), ventricular fibrillation, asystole |
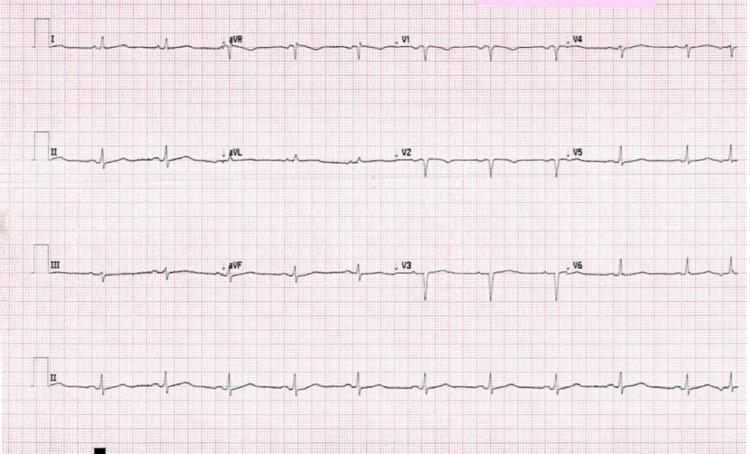
10. Dilated Cardiomyopathy (DCM)
Pathophysiology: Ventricular dilation and systolic dysfunction (reduced EF) from ischemic, idiopathic, viral, toxic, or genetic causes → diffuse myocardial fibrosis → conduction system disease and chamber enlargement.
ECG Changes:
- Left bundle branch block (LBBB) — most characteristic finding; indicates His-Purkinje fibrosis
- Poor R-wave progression across precordial leads (V1–V4)
- Low voltage QRS in limb leads (infiltration/fibrosis)
- Pathological Q waves mimicking prior infarction (ischemic DCM)
- Left atrial enlargement (broad, notched P mitrale)
- Sinus tachycardia (compensatory)
- Atrial fibrillation (common complication)
- Ventricular ectopy / non-sustained VT
Quick Reference Summary Table
| # | Condition | Key ECG Finding |
|---|---|---|
| 1 | STEMI | Convex ST elevation + reciprocal depression + Q waves |
| 2 | Atrial Fibrillation | No P waves, irregularly irregular RR |
| 3 | Complete Heart Block | AV dissociation, slow escape rhythm |
| 4 | Acute Pericarditis | Diffuse concave ST↑, PR depression |
| 5 | LVH | High voltage + lateral strain pattern |
| 6 | Pulmonary Embolism | Sinus tachycardia, S1Q3T3, RV strain |
| 7 | WPW Syndrome | Short PR + delta wave + wide QRS |
| 8 | Ventricular Tachycardia | Wide QRS tachycardia, AV dissociation |
| 9 | Hyperkalemia | Peaked T waves → sine wave |
| 10 | Dilated Cardiomyopathy | LBBB, poor R progression, low voltage |
Sources: Harrison's Principles of Internal Medicine 22E (2025); Tintinalli's Emergency Medicine; Ganong's Review of Medical Physiology; Lippincott Illustrated Reviews: Pharmacology. ECG images from peer-reviewed clinical literature.
This is a shared conversation. Sign in to Orris to start your own chat.