Explain about pulse in detail
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
Now I have comprehensive information. Let me compile a thorough, well-structured answer.
Pulse - A Detailed Overview
1. Definition and Physiological Basis
The pulse is the rhythmic expansion and recoil of an arterial wall caused by the pressure wave generated with each heartbeat. It is important to understand that what you feel when you palpate a pulse is not blood flow itself, but a pressure wave. Blood flows through the vasculature at approximately 0.5 m/sec, while pressure waves in the aorta move at 3-5 m/sec - Roberts and Hedges' Clinical Procedures in Emergency Medicine.
With each cardiac cycle, blood ejected into the aorta initiates this pressure wave, which propagates outward through the arterial tree and can be palpated at various surface locations throughout the body.
2. Clinical Importance
The pulse is one of the most important indices of clinical severity. It provides information about:
- The cardiovascular condition of the patient
- Abnormalities of the heart and vascular system (hypertension, hypotension)
- Systemic conditions such as shock, fever, and thyrotoxicosis
- Cardiac contractility (distinguishing true cardiac arrest from just electrical rhythm) - S Das Manual on Clinical Surgery
3. Properties of the Pulse
When examining a pulse, the following six properties are assessed:
a) Rate
The number of beats per minute. Normal values vary with age:
| Age Group | Normal Pulse Rate (beats/min) |
|---|---|
| Newborn | 120-160 |
| Infant (1-12 months) | 80-140 |
| Toddler (1-3 years) | 80-130 |
| Preschool (3-5 years) | 80-120 |
| School age (6-10 years) | 70-110 |
| Adolescent/Adult | 60-100 |
| Conditioned athlete | 30-50 (can be normal) |
- Tachycardia: HR > 100 bpm in adults (some propose >95 bpm). Causes include fever, hyperthyroidism, sepsis, hypovolemia, pain, anemia, stimulant drugs (cocaine, methamphetamine, anticholinergics).
- Bradycardia: HR < 60 bpm in adults (some propose <45 bpm as a more accurate threshold). Causes include hypothermia, myxedema coma, high athletic conditioning, digitalis/beta-blockers, vagal stimulation.
The pulse also varies with respiration - it increases with inspiration and slows with expiration. This is called sinus dysrhythmia and is physiological, especially in young people.
b) Rhythm
- Regular: Normal.
- Irregularly irregular: Suggests atrial fibrillation or flutter with variable block. In these cases, the apical pulse (auscultated) is often higher than the peripheral pulse because some beats have inadequate stroke volume and are not transmitted - this difference is called the pulse deficit.
- Regularly irregular: Suggests frequent premature beats (e.g., bigeminy).
c) Volume
Reflects stroke volume and correlates with pulse pressure (difference between systolic and diastolic BP).
- Large/bounding volume: Seen in aortic regurgitation, fever, hyperthyroidism, arteriovenous fistula, anemia, sepsis (early/hyperdynamic phase).
- Small/thready volume: Seen in shock, heart failure, hypovolemia, aortic stenosis, advanced sepsis.
d) Tension (Force)
- Reflects vascular tone and blood pressure. A high-tension pulse suggests hypertension; a low-tension pulse suggests hypotension.
e) Character (Waveform)
The shape and quality of the pulse. Several named abnormal pulse characters exist:
| Pulse Character | Description | Cause |
|---|---|---|
| Water-hammer (Collapsing) pulse | Rapid forceful upstroke, then rapid collapse. Felt best by elevating the arm. | Aortic regurgitation, patent ductus arteriosus, thyrotoxicosis, fever |
| Pulsus paradoxus | Exaggerated fall in systolic BP (>10 mmHg) during inspiration | Cardiac tamponade, severe asthma, constrictive pericarditis |
| Pulsus alternans | Beat-to-beat alternation in pulse amplitude (alternating strong and weak) | Systolic left ventricular failure, severe heart failure |
| Bisferiens pulse | Double-peaked systolic pulse | Aortic regurgitation with stenosis, HOCM |
| Anacrotic pulse | Slow-rising, delayed upstroke with a palpable notch on the ascending limb | Severe aortic stenosis |
| Dicrotic pulse | Double pulse (one in systole, one in diastole) | Low cardiac output states |
| Pulsus bigeminus | Alternating strong and weak beats in paired fashion | Bigeminal arrhythmia |
- Roberts and Hedges' Clinical Procedures in Emergency Medicine; Miller's Anesthesia; Fuster and Hurst's The Heart
f) Condition of the Arterial Wall
Palpation of the vessel wall (e.g., the radial artery) may reveal atherosclerotic thickening or calcification (pipe-stem artery / Monckeberg's arteriosclerosis) - S Das Manual on Clinical Surgery.
4. Pulse Pressure
Pulse pressure = Systolic BP - Diastolic BP. Normal pulse pressure is approximately 40 mmHg (range: 30-50 mmHg).
- Narrow pulse pressure (<25 mmHg): Seen in shock, heart failure, cardiac tamponade, severe aortic stenosis.
- Wide pulse pressure (>60 mmHg): Seen in aortic regurgitation, hyperthyroidism, severe anemia, fever, arteriovenous fistula, elderly patients (due to arterial stiffness).
Mean Arterial Pressure (MAP) = Diastolic BP + 1/3 (Pulse Pressure), or MAP = (2 × Diastolic + Systolic) / 3. - Roberts and Hedges' Clinical Procedures in Emergency Medicine
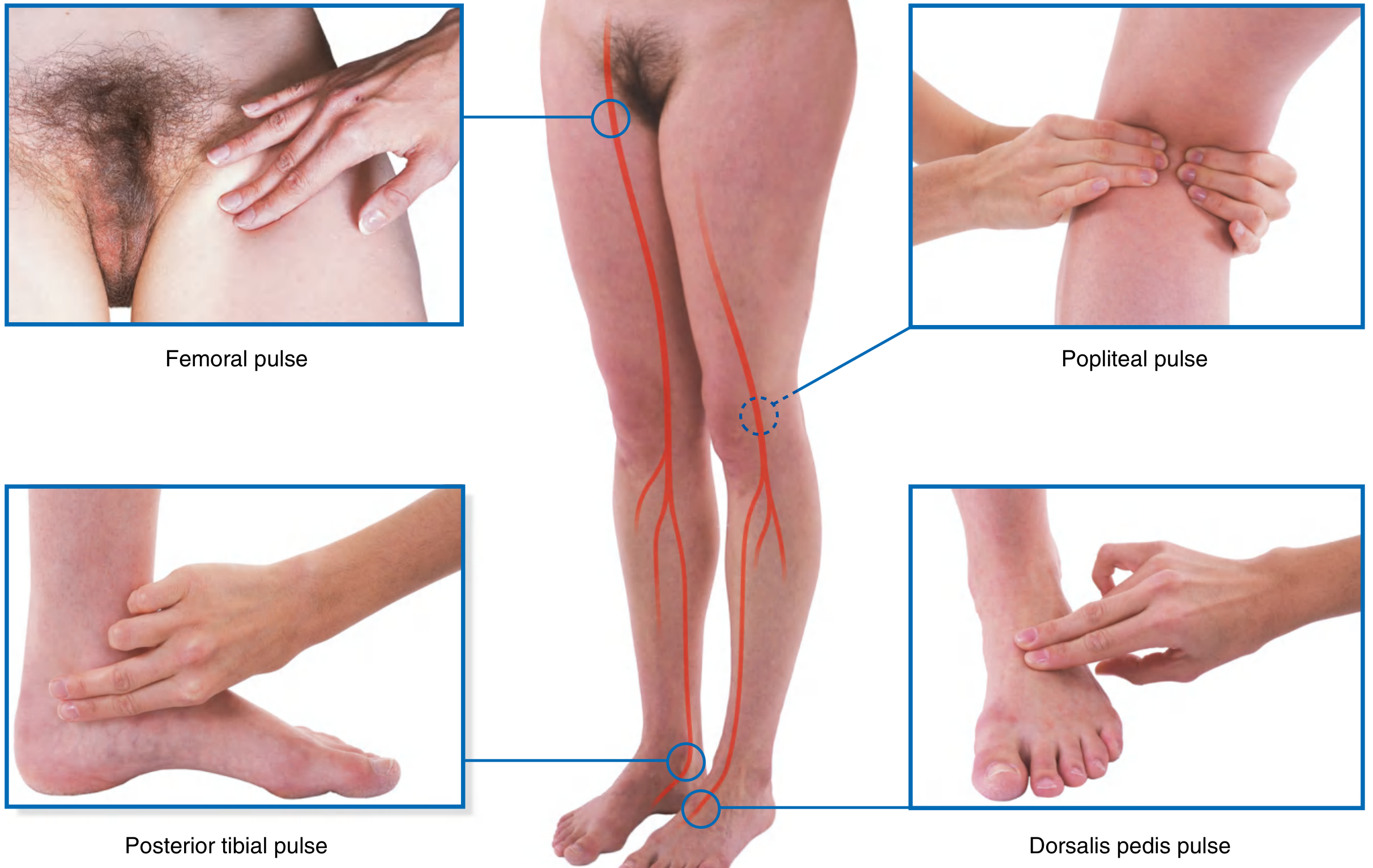
5. Pulse Sites (Where to Palpate)
Pulses can be felt at any superficial artery. Key sites include:
| Site | Artery | Notes |
|---|---|---|
| Radial (wrist) | Radial artery | Most commonly used in routine examination |
| Carotid (neck) | Carotid artery | Best site during CPR; palpate below thyroid cartilage to avoid carotid sinus massage; NEVER palpate both sides simultaneously |
| Brachial (elbow) | Brachial artery | Best for assessing pulse contour and amplitude; medial aspect of antecubital fossa with elbow slightly flexed |
| Femoral (groin) | Femoral artery | Inferior to inguinal ligament, midpoint between ASIS and pubic symphysis |
| Popliteal (back of knee) | Popliteal artery | Deep in the popliteal fossa |
| Posterior tibial | Posterior tibial artery | Posteroinferior to medial malleolus |
| Dorsalis pedis (foot) | Dorsalis pedis artery | Between extensor hallucis longus and extensor digitorum longus tendons |
| Temporal | Superficial temporal artery | In front of the ear / temple |
| Apex (precordium) | N/A (auscultated) | Counted by stethoscope; used when peripheral pulse is irregular |
- Gray's Anatomy for Students
6. How to Palpate the Pulse
- Use the tips of the index and middle fingers (not the thumb - the thumb has its own pulse which may be mistakenly counted).
- For routine examination: count for 15 seconds and multiply by 4 for a regular pulse.
- If any irregularity is suspected: count for a full 60 seconds.
- In neonates: use direct auscultation or umbilical palpation.
- In unstable children: palpate central pulses (femoral, brachial) rather than peripheral ones.
- Doppler ultrasound can be used when the pulse is impalpable (low-flow states, peripheral vascular disease, BP measurement in infants). - Roberts and Hedges' Clinical Procedures in Emergency Medicine
7. Special Considerations
Pulse in CPR
During chest compressions, a palpated femoral pulse may represent to-and-fro blood movement rather than true forward flow. The carotid pulse is preferred for assessing adequacy of compressions. - Roberts and Hedges' Clinical Procedures in Emergency Medicine
Pulse in Sepsis
- Early/hyperdynamic sepsis: Bounding pulses (increased CO, decreased peripheral resistance).
- Late/septic shock: Weak, thready pulses (decreased CO, increased resistance).
Pulse in Trauma/Hypovolemia
Absence of a radial pulse or absence of both radial and femoral pulses is associated with hypotension in hypovolemic trauma patients - though individual variation limits its use as an absolute gauge.
Carotid Pulse
The carotid pulse is examined for volume and contour. It is increased (more intense) in states with high stroke volume: aortic regurgitation, AV fistula, hyperthyroidism, fever, anemia. The upstroke is delayed in valvular aortic stenosis, and amplitude is reduced in any cause of low stroke volume. - Goldman-Cecil Medicine
8. Pulse Amplitude Grading Scale
| Grade | Description |
|---|---|
| 0 | Absent |
| 1+ | Weak/thready |
| 2+ | Normal |
| 3+ | Bounding |
9. Summary of Abnormal Pulse Rates
| Condition | Pulse Change |
|---|---|
| Fever | Tachycardia (except typhoid, drug fever - relative bradycardia) |
| Thyrotoxicosis | Tachycardia |
| Myxedema coma | Bradycardia |
| Hypothermia | Bradycardia (pulse decreases by 50% at 28°C) |
| Shock | Initially tachycardia, then bradycardia before arrest |
| Beta-blockers/Digitalis | Bradycardia, blunted heart rate response |
| Cocaine/Methamphetamine | Tachycardia |
The pulse remains one of the most readily available and clinically rich signs in medicine. A careful assessment of all six properties - rate, rhythm, volume, tension, character, and arterial wall condition - can reveal systemic disease, hemodynamic status, and specific cardiac pathology without any additional equipment.
This is a shared conversation. Sign in to Orris to start your own chat.