Simply explain me psvt
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a clear, simple explanation of PSVT:
PSVT - Paroxysmal Supraventricular Tachycardia
What is it?
PSVT is a family of rapid heart rhythms that start and stop suddenly (hence "paroxysmal") and originate above the ventricles (hence "supraventricular"). The heart suddenly races, then just as suddenly snaps back to normal.
- Harrison's Principles, 22E
The 3 Types (What Causes It?)
About two-thirds of PSVT cases are caused by one of three mechanisms:
| Type | Share | Mechanism |
|---|---|---|
| AVNRT (AV Nodal Reentrant Tachycardia) | ~65% | An electrical loop trapped inside the AV node itself |
| AVRT (AV Reentrant Tachycardia) | ~30% | Uses a secret "accessory pathway" (extra electrical wire) bypassing the AV node - includes WPW syndrome |
| Atrial Tachycardia | ~5% | Ectopic focus firing rapidly from atrial tissue |
Think of it like an electrical short circuit in the heart's wiring. The signal goes around and around in a loop, making the heart beat very fast.
Who Gets It?
-
More common in women
-
Peak onset in late teens and young adults
-
Most patients have no underlying heart disease
-
Incidence is roughly 35 cases per 100,000 person-years
-
Fuster and Hurst's The Heart, 15E
Symptoms
- Palpitations (sudden racing heart - the most common complaint)
- Lightheadedness / dizziness
- Shortness of breath (dyspnea)
- Chest discomfort
- Patients can often pinpoint the exact moment it starts and when it stops
ECG Findings

Key ECG features:
-
Narrow QRS complex (< 100 ms) - fast but normal-looking beats
-
Rate: 130-300 bpm (typically 170-180 bpm)
-
No normal P waves - they are either buried inside the QRS (~70% of cases) or appear as a small "retrograde" (inverted) P wave just before or after the QRS
-
Regular rhythm
-
Tintinalli's Emergency Medicine
Treatment
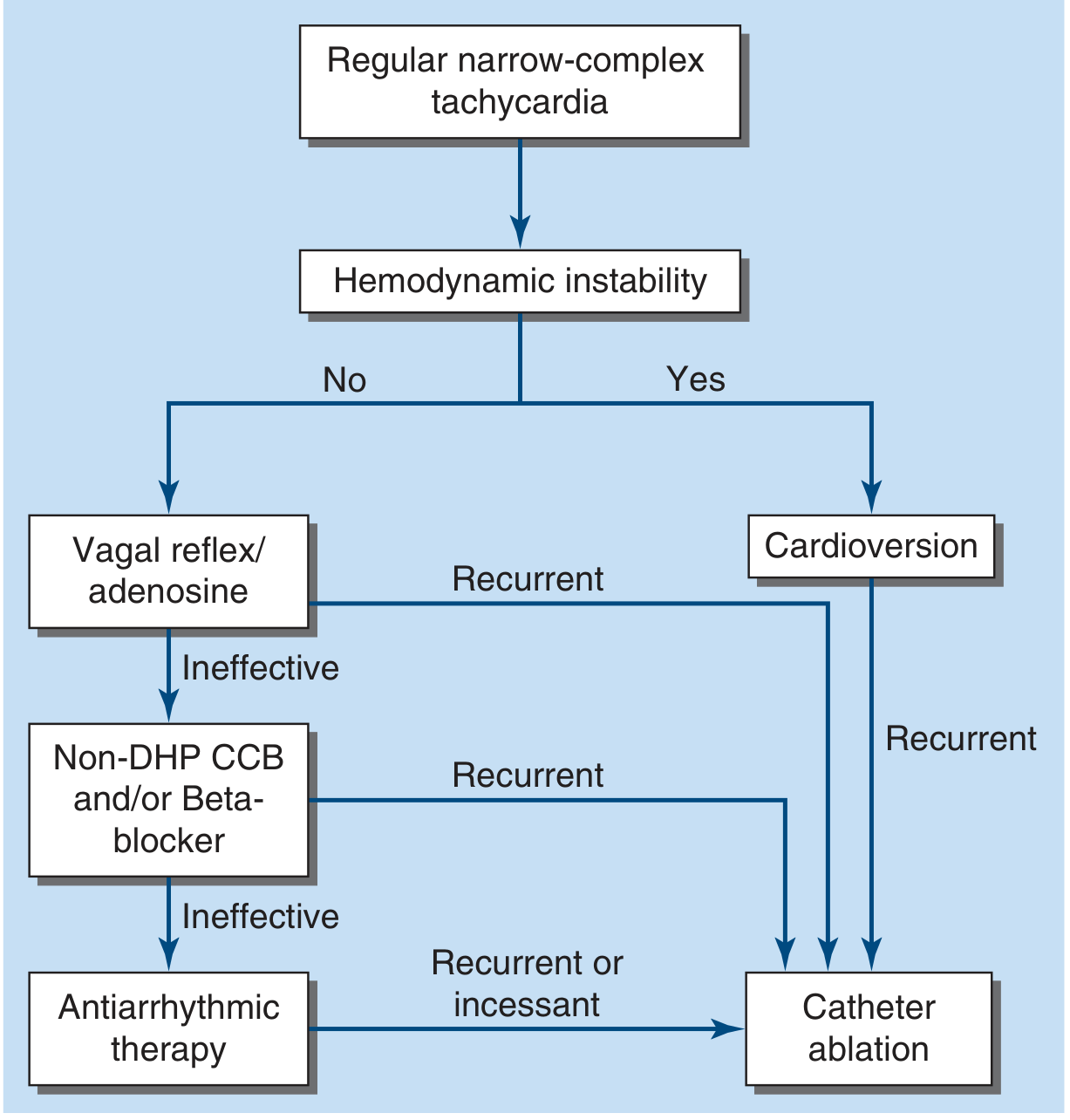
Step 1 - Vagal maneuvers (first, if patient is stable):
- Valsalva maneuver (bear down hard like you're straining)
- Carotid sinus massage
- These work by boosting the vagus nerve, which slows the AV node and breaks the loop
Step 2 - IV Adenosine (if vagal maneuvers fail):
- Temporarily blocks the AV node, terminating the reentrant circuit
- Works in the vast majority of cases
- Side effects: brief chest tightness, flushing, sense of doom (lasts ~10 seconds)
Step 3 - IV Beta-blockers or Calcium channel blockers (verapamil/diltiazem):
- If adenosine fails or is contraindicated
- Slower onset, risk of hypotension
If unstable (hypotensive, unconscious):
- Synchronized DC cardioversion immediately
Long-term / recurrent PSVT:
- Catheter ablation - burns the reentrant pathway with radiofrequency energy - this is curative with high success rates
Simple Summary
PSVT = Heart suddenly racing at 150-300 bpm due to an electrical loop, usually no structural heart disease. Fix it acutely with Valsalva or adenosine; cure it long-term with catheter ablation.
- Harrison's Principles of Internal Medicine 22E | Fuster and Hurst's The Heart, 15E | Tintinalli's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.