Nasal polyps
Reading File
Finding Sources
Searching PubMed
"nasal polyps"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Searching Images
nasal polyps endoscopy
Loading Image
Loading Image
Here is a comprehensive overview of nasal polyps.
Nasal Polyps
Definition & Pathogenesis
Nasal polyps are focal protrusions of inflamed nasal mucosa that typically originate near the ethmoid sinuses in the middle meatus, extending into the nasal cavity. They develop from recurrent mucosal inflammation and edema. On examination they appear silver-gray, translucent, painless, and insensate — painlessness is an important distinguishing feature from sinonasal tumors.
Inflammatory mechanisms:
- Type 2 inflammation (dominant in most CRSwNP): driven by IL-4, IL-5, IL-13, and IgE, with tissue eosinophilia, comorbid asthma, and severe sinus disease
- Type 17 inflammation (subset): predominantly neutrophilic, mediated by IL-17
- Aspirin-exacerbated respiratory disease (AERD): polyps + aspirin sensitivity + asthma from upregulated leukotriene production via arachidonic acid metabolism
Associated conditions:
| Condition | Notes |
|---|---|
| Chronic rhinosinusitis | Most common association |
| Asthma | Strong comorbidity |
| Cystic fibrosis | Especially ΔF508 mutation — test all children with polyps |
| Allergic fungal sinusitis | Elevated IgE, Aspergillus cultures, Charcot-Leyden crystals, characteristic CT densities |
| AERD (Samter's triad) | Polyps + aspirin sensitivity + asthma |
| Inverted papilloma (HPV) | Unilateral; benign but can transform to malignancy |
Despite the apparent allergic appearance, only 0.5% of atopic patients develop nasal polyps, and most patients with polyps are not atopic.
Histology
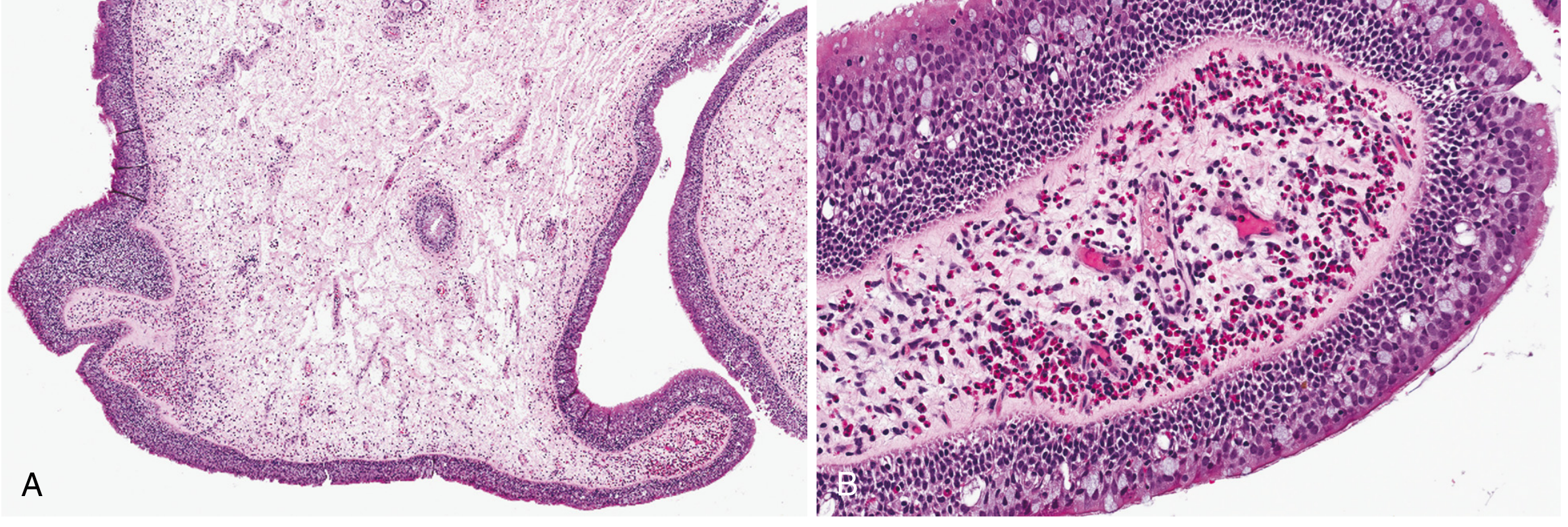
Fig. 16.10 — Robbins & Cotran Pathologic Basis of Disease: (A) Low-power: edematous stroma lined by respiratory epithelium. (B) High-power: stromal edema with eosinophil-rich infiltrate.
Histologic features:
- Edematous mucosa with loose stroma
- Hyperplastic or cystic mucus glands
- Infiltrates of neutrophils, eosinophils, and plasma cells
- Intact mucosal surface (unless superinfected)
- Can reach 3–4 cm in length
Endoscopic Appearance
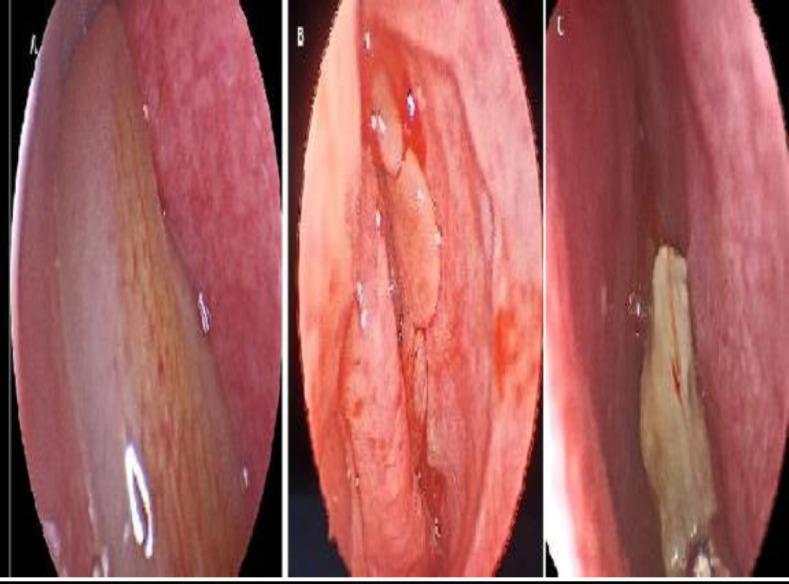
Nasal endoscopy comparison: (A) antrochoanal polyp; (B) bilateral CRSwNP; (C) allergic fungal sinusitis with characteristic "peanut-butter" mucin.
Clinical Features
| Symptom | Notes |
|---|---|
| Nasal obstruction | Often unrelenting; may be visible at nostril in advanced cases |
| Anosmia | Hallmark symptom |
| Rhinorrhea, postnasal drip | Typical rhinitis symptoms |
| Facial/ear pain | More common than in rhinitis without polyps |
| Facial asymmetry / orbital involvement | Sign of neglected advanced disease |
Diagnosis
- Anterior rhinoscopy / nasal endoscopy — visualize polyps directly; staging by extent
- CT scan — defines extent, drainage obstruction, sinus involvement
- Key red flag: Unilateral polyposis → suspect antral choanal polyp, malignancy, inverted papilloma, or allergic fungal sinusitis → early biopsy recommended
- In children: test for cystic fibrosis
- Workup: allergy testing, asthma evaluation, IgE level, fungal cultures if AFS suspected
Treatment
Step 1: Medical (First-line)
| Treatment | Details |
|---|---|
| Intranasal corticosteroids | First-line; effective for reducing polyp bulk and symptoms |
| Oral corticosteroid burst | Prednisone: 40 mg × 5d → 30 mg × 5d → 20 mg × 5d → 10 mg × 5d; or methylprednisolone dose pack |
| Oral steroids + doxycycline | Combination may be more effective (100 mg BID) |
| Montelukast | Leukotriene antagonist, 10 mg once daily; useful adjunct |
| Allergy treatment | Address underlying allergic triggers |
Step 2: Biologics (for refractory CRSwNP)
In adults with CRSwNP refractory to intranasal corticosteroids, biologics added to nasal steroid spray:
| Biologic | Mechanism | Dosing |
|---|---|---|
| Dupilumab | Anti-IL-4Rα (blocks IL-4/IL-13) | 300 mg SC every 2 weeks |
| Omalizumab | Anti-IgE | Weight/IgE-based dosing |
| Mepolizumab | Anti-IL-5 | 100 mg SC every 4 weeks |
A 2024 systematic review and meta-analysis (PMID 39149992) found dupilumab comparable to sinus surgery for polyp burden reduction and symptom control in CRSwNP — an important finding for treatment decision-making.
Step 3: Surgery
- Endoscopic sinus surgery (ESS) — improves symptomatic control, reduces oral steroid need
- Indicated when medical therapy is inadequate
- Polyps almost always recur without continued postoperative medical therapy
- Postoperative intranasal steroids ± biologics are essential to slow recurrence
Special Situations
- Aspirin-exacerbated respiratory disease (AERD): aspirin desensitization or biologics (2026 systematic review [PMID 41556270] supports biologic use in AERD)
- Inverted papilloma: surgical excision; surveillance for malignant transformation
- Cystic fibrosis: manage underlying disease; ESS often needed
Key Associations to Remember
- Samter's triad = nasal polyps + aspirin sensitivity + asthma
- Cystic fibrosis in children → always test
- Unilateral polyp → malignancy until proven otherwise
- AERD mechanism: NSAIDs inhibit COX → shunting to lipoxygenase pathway → ↑ leukotrienes
Sources: Goldman-Cecil Medicine (9780323930345); Robbins & Cotran Pathologic Basis of Disease (9780443264528); Textbook of Family Medicine 9e (9780323239905). Recent evidence: PMID 39149992 (dupilumab vs. surgery meta-analysis, 2024), PMID 41556270 (biologics in AERD, 2026).
This is a shared conversation. Sign in to Orris to start your own chat.