Management in ruptured hepatic adenoma
Reading File
Finding Sources
Finding Sources
Searching PubMed
"hepatic adenoma" AND rupture AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Searching PubMed
"liver adenoma" AND (hemorrhage OR rupture) AND (embolization OR resection)
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
I now have comprehensive information from multiple authoritative surgical and gastroenterology textbooks. Here is a thorough, well-organized answer:
Management of Ruptured Hepatic Adenoma
Ruptured hepatic adenoma is a surgical emergency. About 20-25% of patients with hepatic adenoma present with hemoperitoneum from tumor rupture. The approach is dictated by hemodynamic status, and is a two-phase strategy: hemorrhage control first, then definitive resection.
Background: Why Adenomas Rupture
Hepatic adenomas lack a true fibrous capsule and contain prominent peripheral arteries with thin veins and no biliary or portal architecture. This makes them prone to spontaneous hemorrhage. Inflammatory adenomas (up to 50% of all adenomas, associated with JAK/STAT pathway activation, obesity, and NASH) carry the highest hemorrhage risk due to sinusoidal dilation and intratumoral hemorrhage. Lesions >5 cm carry substantially higher rupture risk.
Phase 1: Acute Hemorrhage Control
Hemodynamically Stable Patient
Transarterial Embolization (TAE) is the treatment of choice for bleeding control in acute rupture when the patient can tolerate it and IR is available.
- TAE can rapidly arrest hemorrhage with high technical success
- It allows the patient to be resuscitated and stabilized before definitive surgery
- After successful TAE and stabilization, the patient is referred for elective surgical resection (usually 4-8 weeks later)
- In rare cases where follow-up MRI shows no residual lesion post-embolization, resection may be deferred
"Transarterial embolization may be used before surgery to reduce the size of the lesion and is the treatment of choice for bleeding control in cases of acute rupture. After the bleeding is controlled, the patient is referred for surgical resection..." - Current Surgical Therapy 14e
Hemodynamically Unstable Patient / TAE Not Available
When embolization fails, is unavailable (remote setting), or the patient is in refractory hemorrhagic shock:
Emergent laparotomy is indicated with:
- Abdominal packing (damage control) - perihepatic packs to tamponade bleeding
- Pringle maneuver (hepatoduodenal ligament inflow occlusion) for intraoperative bleeding control
- Hepatic artery ligation as a last resort if packing fails
Damage control surgery (DCS) principles apply when the patient has the lethal triad (acidosis + coagulopathy + hypothermia):
- Pack and close temporarily
- Transfer to ICU for aggressive resuscitation and correction of coagulopathy
- Return to OR for definitive resection once physiologically optimized
"For patients who present with acute hemorrhage from a ruptured adenoma for which embolization fails or is not an option, emergent laparotomy is indicated. Liver packing and inflow control with Pringle's maneuver are used for bleeding control. Resection may be performed at the same operation, but patients with acidosis, coagulopathy, or hypothermia may require resuscitation before the definitive operation." - Current Surgical Therapy 14e
Phase 2: Definitive Surgical Resection
Once the patient is stabilized (typically weeks after acute hemorrhage control), elective surgical resection is recommended for virtually all ruptured adenomas, regardless of size. Resection also serves to:
- Prevent recurrent hemorrhage
- Exclude malignant transformation (especially beta-catenin subtype)
- Provide histologic diagnosis
Surgical Options
| Technique | Notes |
|---|---|
| Formal liver resection | Standard approach; anatomic or non-anatomic |
| Enucleation | Acceptable for peripheral lesions; low recurrence |
| Minimally invasive (laparoscopic/robotic) | Preferred when location and size permit |
Resection should be parenchymal-sparing while achieving complete excision. Laparoscopic/robotic left hepatectomy for hemorrhagic adenoma has been reported as feasible in the semi-acute setting (PMID: 37490115).
Management Algorithm (Fischer's Mastery of Surgery)
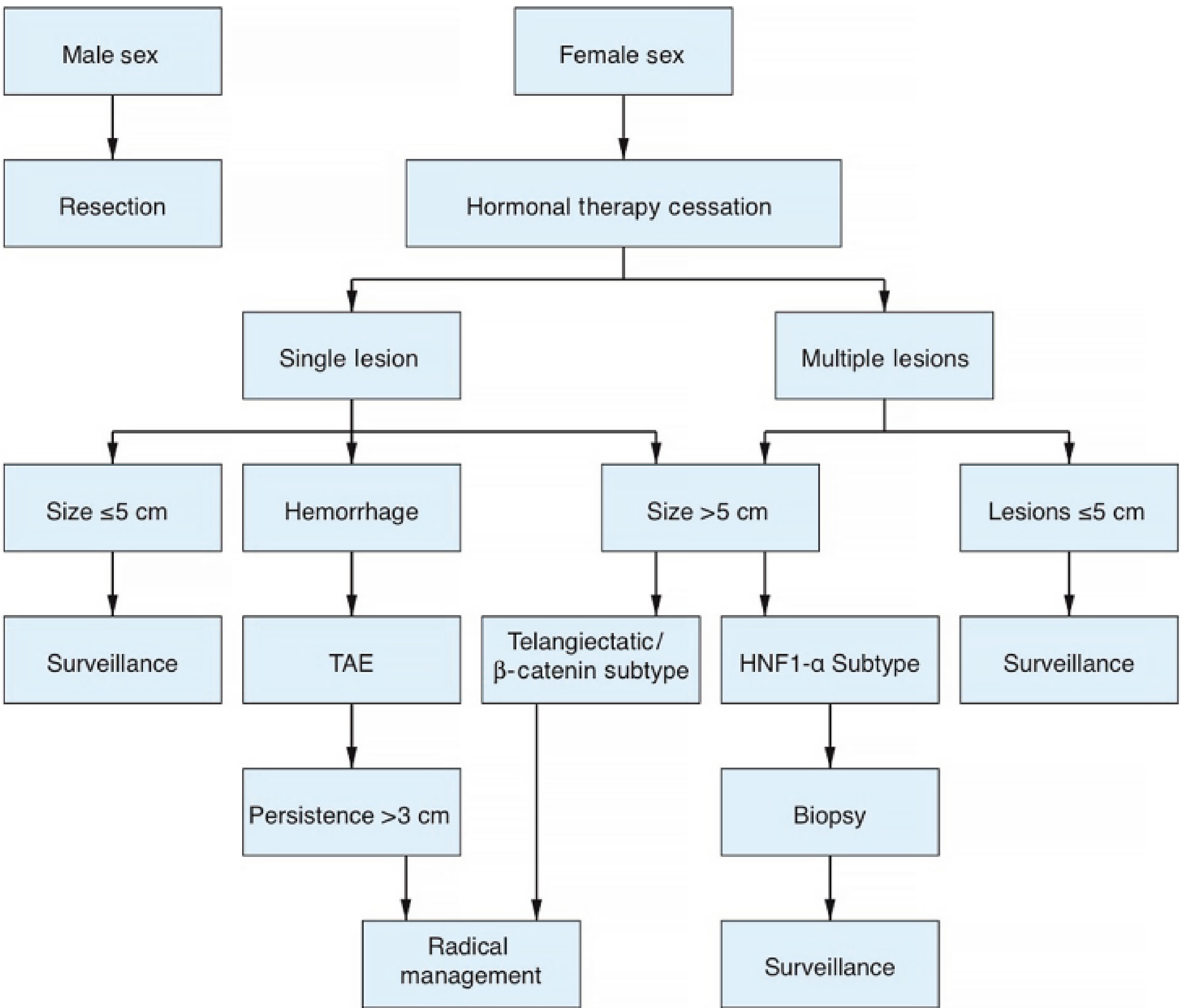
Figure 160.7 - Diagnostic and therapeutic algorithm for hepatic adenoma (adapted from Agrawal et al., Clin Gastroenterol Hepatol 2015). For hemorrhage: TAE → if persistence >3 cm or other high-risk features → radical management (resection).
Special Scenario: Ruptured Adenoma in Pregnancy
This is a particularly high-risk situation:
- Rupture during pregnancy carries ~60% maternal and fetal mortality, even with operative intervention
- Presentation: right upper quadrant pain, right shoulder pain (diaphragmatic irritation), rapid progression to shock
- Immediate laparotomy is the standard of care: cesarean delivery + control of hemorrhage + adenoma resection if feasible
- Angioembolization can be considered if the patient is relatively stable or postpartum
- After recovery, elective resection during the second trimester minimizes operative risk while protecting the remainder of the pregnancy
"The major risk of a hepatic adenoma during pregnancy is spontaneous rupture, which carries a mortality rate of approximately 60% for mother and fetus, even with operative intervention... Immediate laparotomy is performed with cesarean birth, control of hemorrhage, and resection of the adenoma, if possible." - Sabiston Textbook of Surgery
Summary: Management Steps
RUPTURED HEPATIC ADENOMA
|
Hemodynamically?
/ \
STABLE UNSTABLE
| |
TAE Laparotomy
(1st line) + Packing/Pringle
| |
Resuscitate DCS if lethal triad
| |
+-----> Elective Resection (4-8 weeks) <----+
After resection:
- Cessation of oral contraceptives / anabolic steroids
- Avoid future OCP use and counsel on pregnancy risks
- Surveillance imaging to confirm no recurrence
Sources
- Current Surgical Therapy, 14e - Management section on hepatic adenoma
- Fischer's Mastery of Surgery, 8e - Chapter 160, Figure 160.7
- Sabiston Textbook of Surgery - Liver Disorders / Liver Disease in Pregnancy
- Mulholland and Greenfield's Surgery, 7e - Hepatic Adenoma
- Yamada's Textbook of Gastroenterology, 7e - Benign hepatic lesions
- PMID 37490115 (Robotic hepatectomy for hemorrhagic adenoma, Am Surg 2023)
This is a shared conversation. Sign in to Orris to start your own chat.