maps OG8.1 ENUMERATE, DESCRIBE AND DISCUSS THE OBJECTIVES OF ANTENATAL CARE, ASSESSMENT OF PERIOD OF GESTATION; SCREENING FOR HIGH-RISK FACTORS. THE OBJECTIVES OF ANTENATAL CARE
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have all the content needed to give a thorough, structured answer. Here is the complete response:
OG8.1 - Antenatal Care: Objectives, Assessment of Period of Gestation, and Screening for High-Risk Factors
(Source: Park's Textbook of Preventive and Social Medicine)
DEFINITION OF ANTENATAL CARE
Antenatal care (ANC) is defined as the care provided by skilled health-care professionals to pregnant women and adolescent girls in order to ensure the best health conditions for both mother and baby during pregnancy. Its components include:
- Risk identification
- Prevention and management of pregnancy-related or concurrent diseases
- Health education and health promotion
ANC reduces maternal and perinatal morbidity and mortality both directly (through detection) and indirectly (by identifying women at increased risk of complications during labour/delivery and ensuring referral to an appropriate level of care).
I. OBJECTIVES OF ANTENATAL CARE
The objectives of ANC are:
| # | Objective |
|---|---|
| 1 | Promote, protect and maintain health of the mother during pregnancy |
| 2 | Detect "high-risk" cases and give them special attention |
| 3 | Foresee complications and prevent them |
| 4 | Remove anxiety and dread associated with delivery |
| 5 | Reduce maternal and infant mortality and morbidity |
| 6 | Teach the mother elements of child care, nutrition, personal hygiene, and environmental sanitation |
| 7 | Sensitize the mother to the need for family planning, including advice to cases seeking medical termination of pregnancy |
| 8 | Attend to under-fives accompanying the mother |
II. ANTENATAL VISITS - SCHEDULE
These objectives are achieved through a programme of health care services. The ideal schedule:
- Months 1-7: Once a month
- Month 8: Twice a month
- Month 9 onward: Once a week (if everything is normal)
Minimum 4 visits (as per Government of India guidelines):
| Visit | When |
|---|---|
| 1st | Within 12 weeks (as soon as pregnancy is suspected) |
| 2nd | Between 14 and 26 weeks |
| 3rd | Between 28 and 34 weeks (medical officer check at PHC advised) |
| 4th | Between 36 weeks and term |
III. ASSESSMENT OF PERIOD OF GESTATION
A. History-Taking (I. component of antenatal check-up)
- Record the date of 1st day of last menstrual period (LMP)
- Calculate Expected Date of Delivery (EDD) by adding 9 months and 7 days to the 1st day of LMP (Naegele's rule)
- Record symptoms indicating complications (fever, bleeding, absent foetal movements, etc.)
B. Physical Examination - Abdominal Palpation (III. component)
Key findings used to assess gestational age clinically:
- Fundal height - The level of the uterine fundus correlates with weeks of gestation (see figure below)
- Foetal heart sounds - Heard with a stethoscope/Doppler
- Foetal movements - Noted from around 20 weeks
- Foetal parts - Can be distinguished from the 28th week onward
- Multiple pregnancy - Suspected if uterus is larger than estimated gestational age, or palpation of multiple foetal parts
- Foetal lie and presentation - Relevant only after 32 weeks
- Abdominal scars - Inspection for any relevant abdominal findings
C. Uterine Fundal Height - Key Clinical Landmarks
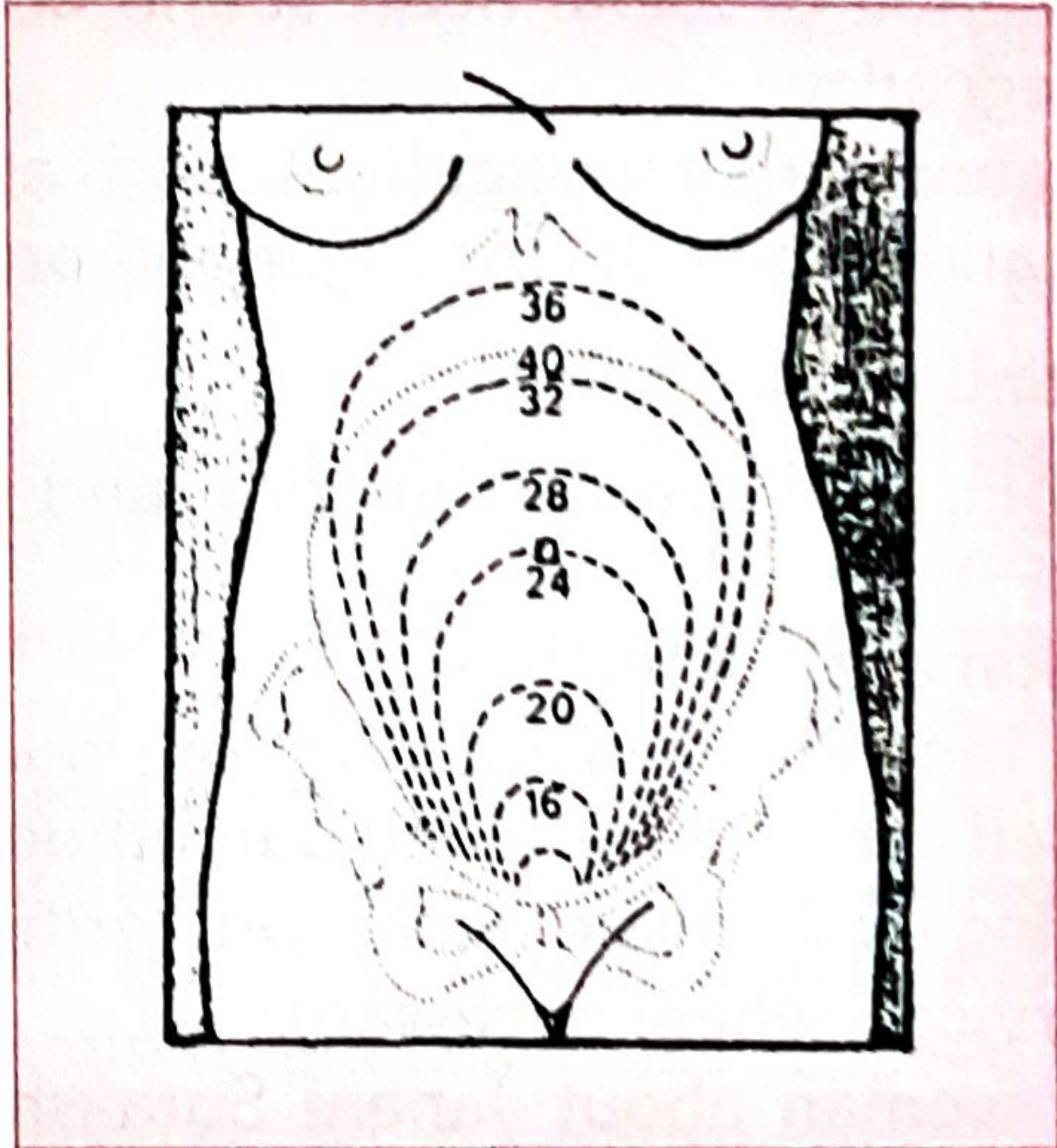
Fig. 1 - Uterine fundal height at various stages of pregnancy. Numbers indicate weeks of gestation (16, 20, 24, 28, 32, 36, 40).
D. Assessment of Gestational Age (IV. component)
| Method | Details |
|---|---|
| LMP-based | Previously most widespread; remains the only available method in many low-income settings |
| Ultrasound (gold standard) | Routine early ultrasound + foetal measurements, ideally in the first trimester |
| "Best obstetric estimate" | Combines ultrasound and LMP - now used by many countries |
| Alternative methods (low-resource settings) | Fundal height, clinical assessment of newborn after birth, or birth weight as a surrogate |
Ultrasound requires skilled technicians, equipment, and first-trimester ANC attendance - not always feasible in low-income settings where the majority of preterm births occur.
IV. LABORATORY INVESTIGATIONS
At Sub-centre level:
- Pregnancy detection test
- Haemoglobin estimation
- Urine test for albumin and sugar
- Rapid malaria test
At PHC/CHC/FRU level:
- Blood group including Rh factor
- VDRL/RPR (syphilis)
- HIV testing
- Blood sugar
- Thyroid function (where indicated)
- Ultrasound
V. SCREENING FOR HIGH-RISK FACTORS - THE RISK APPROACH
"The central purpose of antenatal care is to identify 'high risk' cases (as early as possible) from a large group of antenatal mothers and arrange for them skilled care, while continuing to provide appropriate care for all mothers."
- Park's Textbook of Preventive and Social Medicine
High-Risk Factors (to be screened for):
| Category | High-Risk Factors |
|---|---|
| Age/Parity | Elderly primi (≥30 years); Elderly grandmultiparas |
| Anthropometric | Short-statured primi (≤140 cm) |
| Obstetric - Current | Malpresentations (breech, transverse lie); Antepartum haemorrhage / threatened abortion; Pre-eclampsia and eclampsia; Twins, hydramnios; Prolonged pregnancy (>14 days after EDD) |
| Obstetric - Past | Previous stillbirth, intrauterine death, manual removal of placenta; Previous abortion; Previous caesarean or instrumental delivery; Three or more spontaneous consecutive abortions |
| Medical | Cardiovascular disease, kidney disease, diabetes, tuberculosis, liver disease, malaria, convulsions, asthma, HIV, RTI, STI |
| Reproductive | Treatment for infertility |
| Haematological | Anaemia |
The Risk Approach - Purpose and Philosophy
The "risk approach" is a managerial tool for improved MCH care. Its purpose is to provide better services for all, but with special attention to those who need them most. Key principles:
- Maximum utilization of all resources - including non-conventional human resources (traditional birth attendants, community health workers, women's groups)
- Far-reaching effects on the whole organization of MCH/FP services
- Improvements in both coverage and quality of health care at all levels, particularly at the primary health care level
VI. INTERVENTIONS AND COUNSELLING AT EACH VISIT
- Iron and folic acid (IFA) supplementation
- Immunization against tetanus (TT injection)
- Group or individual instruction on nutrition, family planning, self-care, delivery, and parenthood
- Home visiting by a female health worker/trained dai
- Referral services where necessary
- Inform the woman about Janani Suraksha Yojana (JSY) and other government incentives
SUMMARY TABLE
| Component | Key Points |
|---|---|
| ANC Definition | Care by skilled professionals during pregnancy to ensure best health for mother and baby |
| Objectives | 8 objectives - from maternal health promotion to family planning sensitization |
| Visit Schedule | Minimum 4 visits; ideally monthly in 1st 7 months |
| Gestational Age | LMP (Naegele's rule), fundal height clinically, ultrasound is gold standard |
| High-Risk Screening | 14 categories screened at every ANC visit |
| Risk Approach | Managerial tool - special attention to high-risk while covering all mothers |
- Park's Textbook of Preventive and Social Medicine, pp. 611-616
This is a shared conversation. Sign in to Orris to start your own chat.