Important disease that can be diagnosed with ecg
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
I now have rich, authoritative content from Tintinalli's Emergency Medicine and multiple other textbooks. Let me compile a comprehensive, well-structured answer.
Important Diseases Diagnosed with the ECG
The 12-lead ECG is one of the most powerful, non-invasive tests in medicine. Below is a comprehensive breakdown of the most important conditions it can identify, with key ECG findings for each.
1. Ischemic Heart Disease (Most Important Use)
The standard 12-lead ECG is described as "the single best test - although it can be fallible - to identify patients with AMI upon ED presentation." Guidelines recommend obtaining it within 10 minutes of arrival for chest pain.
| Condition | Key ECG Findings |
|---|---|
| STEMI (ST-elevation MI) | ST elevation ≥1 mm in ≥2 contiguous leads; new LBBB |
| NSTEMI | ST depression, T-wave inversions, or non-specific changes |
| Unstable Angina | May be normal, or show transient ST/T changes |
| Old (prior) MI | Pathological Q waves |
| Right Ventricular MI | ST elevation in V4R (right-sided leads); often with inferior STEMI |
| Posterior MI | Tall R wave + ST depression in V1-V2; ST elevation in posterior leads (V7-V9) |
Localization of STEMI by leads (from Tintinalli's Emergency Medicine):
- Anteroseptal: V1, V2 (±V3)
- Anterior: V1-V4
- Anterolateral: V1-V6, I, aVL
- Lateral: I, aVL
- Inferior: II, III, aVF
- Right ventricular: ST elevation in II, III, aVF + right-sided leads
"New ST-segment elevation of ≥1 mm in at least two contiguous leads represents an AMI that will benefit from rapid reperfusion interventions." - Tintinalli's Emergency Medicine
2. Cardiac Arrhythmias
| Condition | Key ECG Findings |
|---|---|
| Atrial fibrillation | Absent P waves, irregularly irregular RR intervals, fibrillatory baseline |
| Atrial flutter | Sawtooth flutter waves at ~300 bpm; 2:1, 3:1, or 4:1 block |
| SVT (AVNRT/AVRT) | Regular narrow-complex tachycardia ~150-250 bpm; P waves hidden in QRS or retrograde |
| Ventricular tachycardia (VT) | Wide-complex (>120 ms) tachycardia ≥3 beats; AV dissociation |
| Ventricular fibrillation | Chaotic irregular waveform; no recognizable QRS |
| Sinus node dysfunction / Sick sinus syndrome | Inappropriate bradycardia, sinus pauses, tachycardia-bradycardia alternation |
3. Conduction Defects & Heart Blocks
| Condition | Key ECG Findings |
|---|---|
| 1st degree AV block | PR interval >200 ms, every P conducts |
| 2nd degree - Mobitz I (Wenckebach) | Progressive PR prolongation until a P wave drops |
| 2nd degree - Mobitz II | Fixed PR with sudden dropped beats - higher risk of complete block |
| 3rd degree (complete) AV block | Complete AV dissociation; P and QRS independent |
| LBBB | Wide QRS >120 ms; broad notched R in I, V5-V6; QS in V1 |
| RBBB | RSR' ("M" pattern) in V1-V2; wide S in I, V5-V6 |
4. Hereditary Channelopathies
These are critical to identify as they cause sudden cardiac death in young patients.
| Condition | Key ECG Findings |
|---|---|
| Brugada syndrome | Coved ST-segment elevation in V1-V3 resembling RBBB; often intermittent or fever-unmasked |
| Long QT syndrome (LQTS) | Corrected QT (QTc) >460-480 ms; risk for Torsades de Pointes |
| Short QT syndrome | QTc <340-360 ms; peaked T waves |
| Catecholaminergic polymorphic VT (CPVT) | Normal resting ECG; exercise-provoked bidirectional VT |
"Many cases [of sudden arrhythmic death syndrome] can be identified clinically based on their characteristic ECG patterns." - Tintinalli's Emergency Medicine
5. Wolff-Parkinson-White (WPW) Syndrome
- Short PR interval (<120 ms)
- Delta wave (slurred upstroke of QRS)
- Wide QRS complex
- Risk: if atrial fibrillation develops + rapid conduction via accessory pathway → ventricular fibrillation
6. Cardiomyopathies & Structural Conditions
| Condition | Key ECG Findings |
|---|---|
| Left ventricular hypertrophy (LVH) | High voltage (Sokolow-Lyon: SV1 + RV5 >35 mm), ST/T changes |
| Right ventricular hypertrophy (RVH) | Right axis deviation, dominant R in V1, S waves in I/V6 |
| Hypertrophic cardiomyopathy (HCM) | LVH pattern, deep Q waves in lateral leads, ST changes |
| Dilated cardiomyopathy | LBBB, poor R-wave progression, non-specific ST changes |
7. Pericarditis & Myocarditis
| Condition | Key ECG Findings |
|---|---|
| Acute pericarditis | Diffuse saddle-shaped ST elevation (all leads except aVR, V1); PR depression; stage progression over days |
| Cardiac tamponade | Electrical alternans (alternating QRS axis/amplitude) + sinus tachycardia |
| Myocarditis | Non-specific ST/T changes; may mimic MI; arrhythmias |
8. Pulmonary Conditions
| Condition | Key ECG Findings |
|---|---|
| Pulmonary embolism (PE) | S1Q3T3 pattern (S wave in I, Q wave + T inversion in III); sinus tachycardia; new RBBB; right heart strain pattern |
| Pulmonary hypertension | RVH pattern, right axis deviation, P pulmonale |
| Pneumothorax | Decreased QRS voltage on affected side; axis changes |
9. Electrolyte & Metabolic Disorders
| Condition | Key ECG Findings |
|---|---|
| Hyperkalemia | Peaked narrow T waves → widened QRS → sine wave → asystole (progressive with rising K+) |
| Hypokalemia | Flattened T waves, prominent U waves, QT prolongation |
| Hypercalcemia | Shortened QT interval |
| Hypocalcemia | Prolonged QT interval |
| Hypothermia | Osborn (J) waves (positive deflection at J point), bradycardia, prolonged PR/QRS/QT |
| Hypothyroidism | Sinus bradycardia, low voltage, prolonged QT |
| Digitalis toxicity | "Scooped" ST depression; various arrhythmias; AV block |
10. Other Important Conditions
| Condition | Key ECG Findings |
|---|---|
| Dextrocardia | Inverted P/QRS in lead I; right axis deviation; reverse R-wave progression |
| Lown-Ganong-Levine syndrome | Short PR, normal QRS (no delta wave) |
| Aortic stenosis | LVH pattern |
| Sick sinus syndrome | Sinus pauses, inappropriate bradycardia, tachycardia-bradycardia pattern |
Quick ECG Pattern Summary
| ECG Finding | Think of... |
|---|---|
| ST elevation | STEMI, pericarditis, Brugada, LV aneurysm, early repolarization |
| ST depression | NSTEMI, ischemia, digitalis, LVH strain |
| Long QT | LQTS, drugs (amiodarone, sotalol, antibiotics), hypokalemia, hypocalcemia |
| Delta wave | WPW |
| Peaked T waves | Hyperkalemia, early MI (hyperacute) |
| Osborn (J) wave | Hypothermia |
| Electrical alternans | Cardiac tamponade |
| S1Q3T3 | Pulmonary embolism |
| Sawtooth P waves | Atrial flutter |
| PR depression | Pericarditis |
Sources:
- Tintinalli's Emergency Medicine: A Comprehensive Study Guide (chapters on ACS, chest pain, channelopathies, cardiac arrest)
- Fuster and Hurst's The Heart, 15th Edition (Brugada syndrome)
- Goldman-Cecil Medicine (sudden cardiac death, channelopathies)
- Braunwald's Heart Disease (syncope, ECG in structural disease)
Ecg image
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
I now have 6 excellent ECG images from authoritative textbooks. Let me compile the full answer with all images and their clinical explanations.
ECG Patterns of Important Diseases - Textbook Images
Here are real ECG tracings from medical textbooks, organized by disease category.
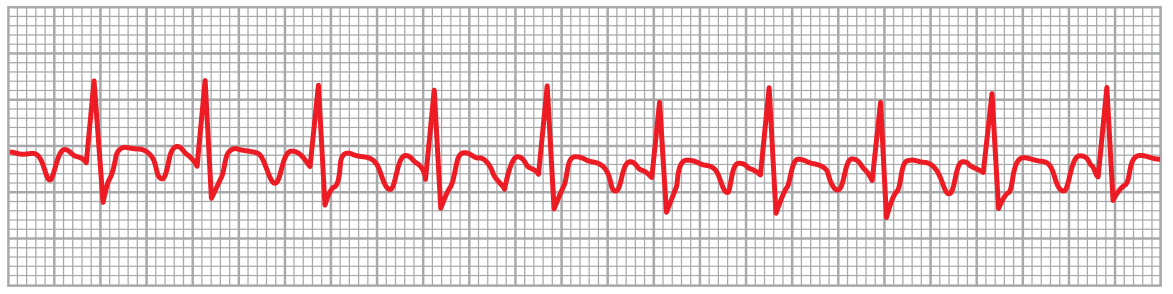
1. Atrial Fibrillation

What to see: No visible P waves, irregularly irregular RR intervals. The QRS-T complexes are normal but their spacing is completely unpredictable - this is the hallmark. Rate typically 125-150 bpm if uncontrolled.
Source: Guyton & Hall Textbook of Medical Physiology - Fig 13.20, Lead II
2. Atrial Flutter
What to see: Classic sawtooth (flutter) waves at ~250 bpm. The ventricles respond at half the rate (2:1 block) giving ~125 bpm. P waves are strong (coordinated atrial contraction) but too rapid to conduct 1:1 through the AV node.
Source: Guyton & Hall Textbook of Medical Physiology - Fig 13.21, Lead II
3. Brugada Syndrome
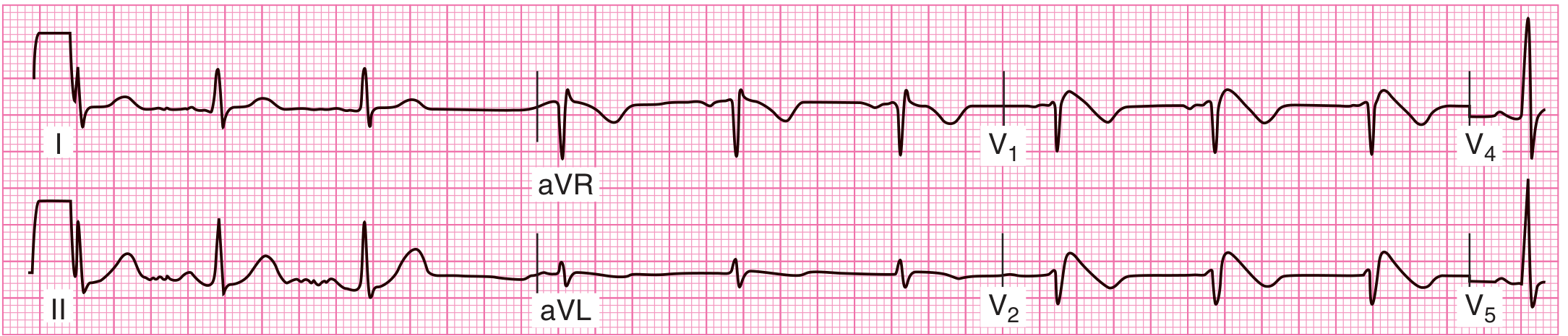
What to see: Characteristic downsloping (coved) ST-segment elevation in leads V1-V2, with QRS morphology resembling a right bundle branch block. This is a sodium channelopathy associated with 40-60% risk of life-threatening ventricular arrhythmias and sudden cardiac death - most common during sleep in Southeast Asian males.
Source: Tintinalli's Emergency Medicine - Fig 11-1
4. Atrial Fibrillation with Pulmonary Hypertension / Right Heart Strain
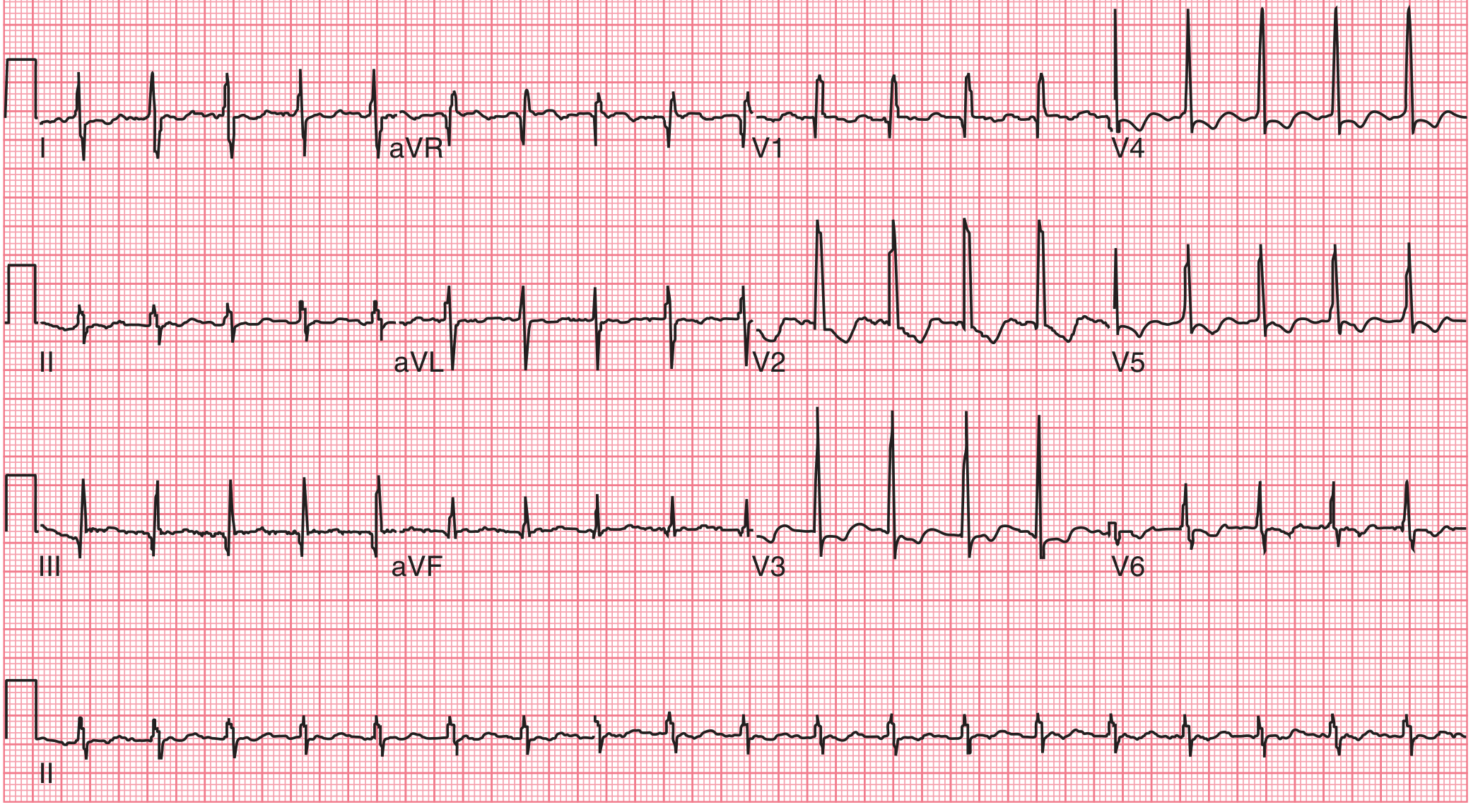
What to see: Atrial fibrillation (irregular rhythm, no P waves) plus signs of right ventricular strain: R/S ratio >1 in V1, right axis deviation (dominant deflection in III/aVF), ST depressions in V1-V3 indicating RV ischemia/strain. This pattern raises suspicion for pulmonary hypertension or pulmonary embolism.
Source: Tintinalli's Emergency Medicine - Fig 58-1
5. Hypokalemia ECG (K+ = 1.4 mEq/L)
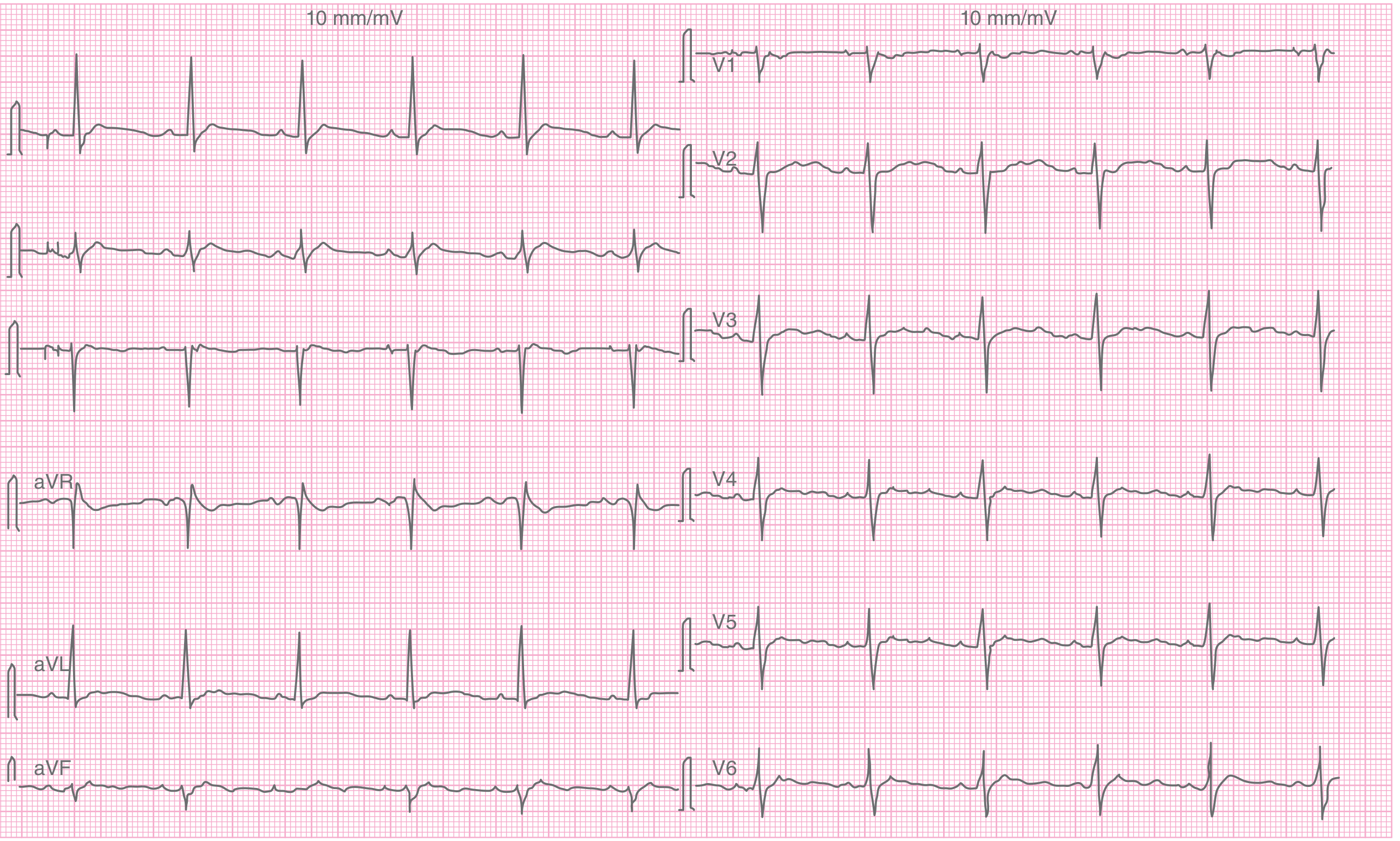
What to see: Prolonged QT interval, flattened T waves, and visible U waves (positive deflection after T wave, most prominent in V1-V3). This patient had severe hypokalemia (K+ 1.4 mEq/L) from thiazide diuretic use, presenting with leg paralysis and fatigue.
Source: Tintinalli's Emergency Medicine - Fig 17-4
6. Severe Hyperkalemia (K+ = 9.1 mEq/L) - Pre-cardiac Arrest
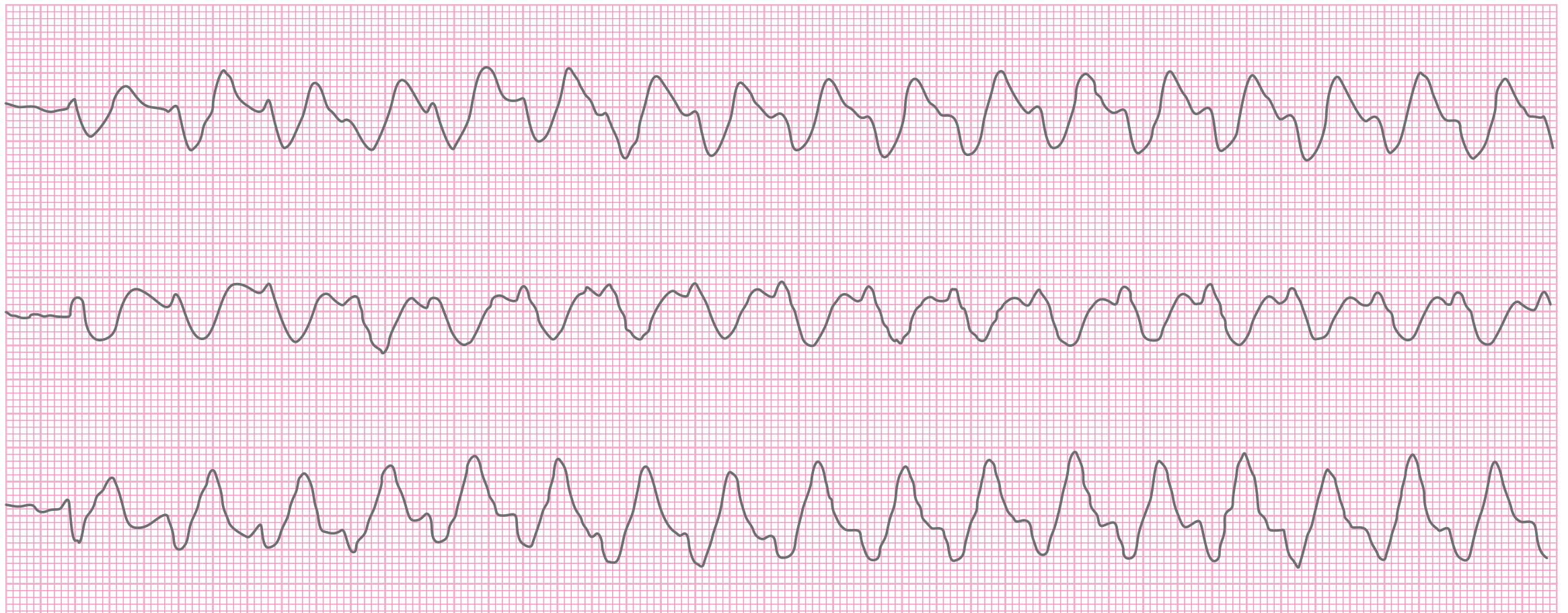
What to see: With extreme hyperkalemia (K+ 9.1 mEq/L), the ECG shows wide, bizarre, sinusoidal waveforms - the P waves disappear, the QRS broadens dramatically and merges with the T wave ("sine wave" pattern). This patient was hypotensive and deteriorating into cardiac arrest. This is a medical emergency requiring immediate calcium administration.
Source: Tintinalli's Emergency Medicine - Fig 17-5 (monitor strip, leads V, Y)
Summary: Key ECG Features at a Glance
| Disease | Signature ECG Finding |
|---|---|
| Atrial fibrillation | No P waves, irregularly irregular RR |
| Atrial flutter | Sawtooth waves ~300 bpm, regular ventricular rhythm |
| Brugada syndrome | Coved ST elevation V1-V2, RBBB-like pattern |
| STEMI | ST elevation ≥1 mm in ≥2 contiguous leads |
| Pulmonary hypertension | RVH pattern, right axis deviation, S1Q3T3 (if PE) |
| Hypokalemia | Flat T waves, U waves, prolonged QT |
| Hyperkalemia (severe) | Wide sine-wave QRS, absent P waves |
| Pericarditis | Diffuse saddle-shaped ST elevation + PR depression |
| Long QT / Brugada | QTc >460 ms / Coved V1-V2 elevation |
| WPW | Short PR + delta wave + wide QRS |
Management of Hyperkalemia
Reading File
You've run out of free credits. Sign up for a free account to continue using Orris.
This is a shared conversation. Sign in to Orris to start your own chat.