Who cns tumors classification with histopathological images for pathologist
"CNS tumors"[MeSH Terms] AND "WHO classification"
"brain tumor" AND "WHO classification" AND histopathology
PMID: 39724142
WHO Classification of CNS Tumors: A Histopathologist's Guide
Framework of the WHO 2021 CNS Classification
- Tumor type is defined by morphology + molecular markers together
- CNS WHO grading is intratype (grade 2 astrocytoma vs. grade 3 astrocytoma are within the same entity, not a spectrum that includes glioblastoma)
- Arabic numerals are used for grades (grade 2, 3, 4 - not II, III, IV)
- Molecular features can override morphology for grading (e.g., IDH-wildtype diffuse astrocytoma with TERT mutation = glioblastoma grade 4, even without necrosis)
1. Diffuse Gliomas (Intraparenchymal, Infiltrating)
| Feature | Astrocytoma, IDH-mutant | Oligodendroglioma | Glioblastoma, IDH-wt |
|---|---|---|---|
| IDH status | Mutant | Mutant | Wildtype |
| Other genetics | TP53 mut, ATRX mut, CDKN2A-HD (grade 4) | 1p/19q codeletion | +7/-10, TERT-promoter mut, EGFR amp |
| Grades | 2, 3, 4 | 2 or 3 | 4 (by definition) |
| Morphology | Nuclear atypia; mitoses (grade 3); MVP/necrosis (grade 4) | Round nuclei, clear halos; mitoses + MVP/necrosis (grade 3) | Nuclear atypia, mitoses, MVP, necrosis |
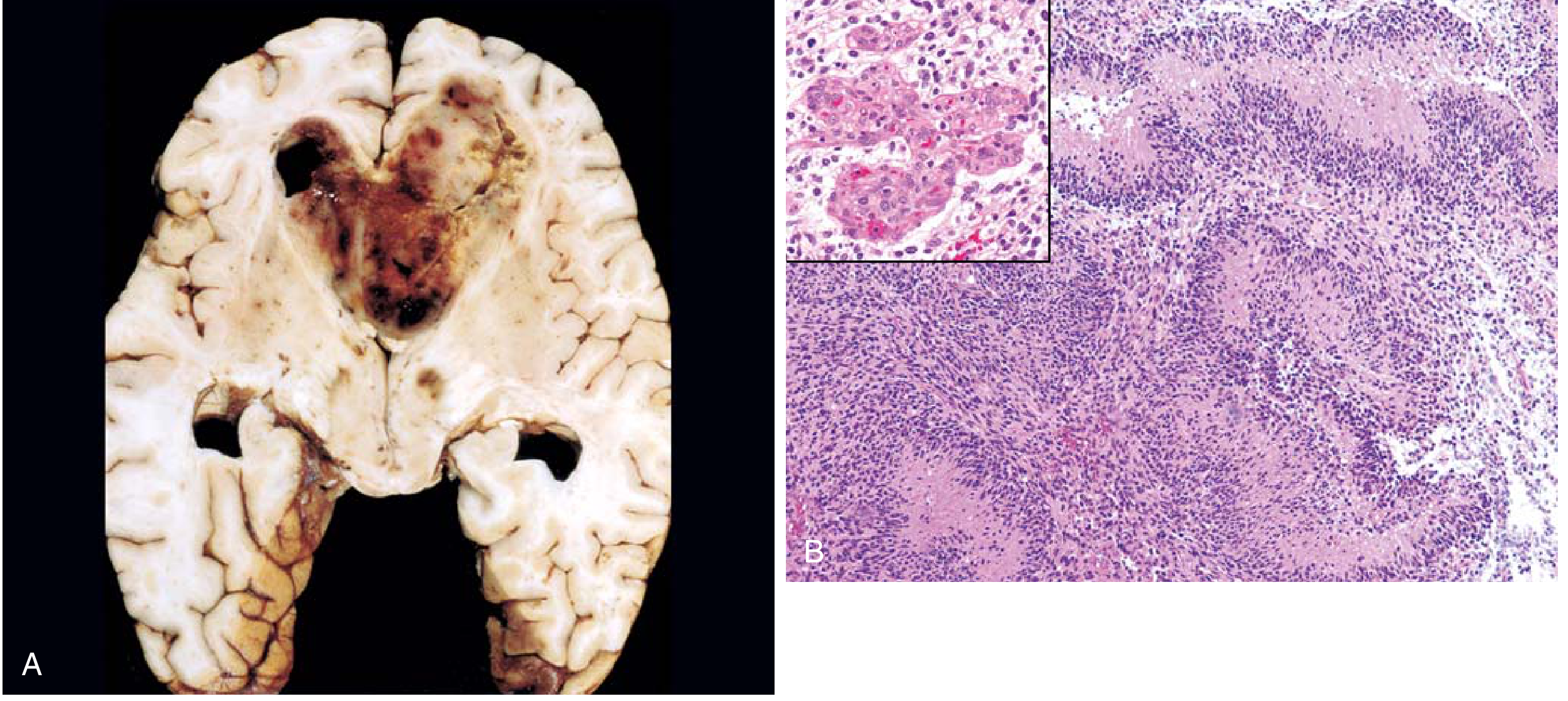
1a. Astrocytoma, IDH-mutant (WHO Grades 2-4)
- Poorly demarcated, infiltrative gray tumor expanding white matter
- Hypercellularity with enlarged, elongated or irregular hyperchromatic nuclei embedded in a fibrillary background
- GFAP-positive fibrillary matrix; tumor cells show IDH1 R132H immunopositivity (inset)
- Grade 3: increased cellularity + readily detectable mitoses
- Grade 4: microvascular proliferation (multilayered small vessels) + necrosis and/or homozygous CDKN2A deletion

1b. Glioblastoma, IDH-wildtype (WHO Grade 4)
- Pseudopalisading necrosis: serpentine bands of necrosis with viable hypercellular tumor arranged in palisades along the necrotic edge
- Microvascular proliferation: tufts of cells piling up within vessel lumens (glomeruloid bodies)
- High cellularity, marked nuclear pleomorphism, brisk mitoses
- Ring-enhancing on MRI
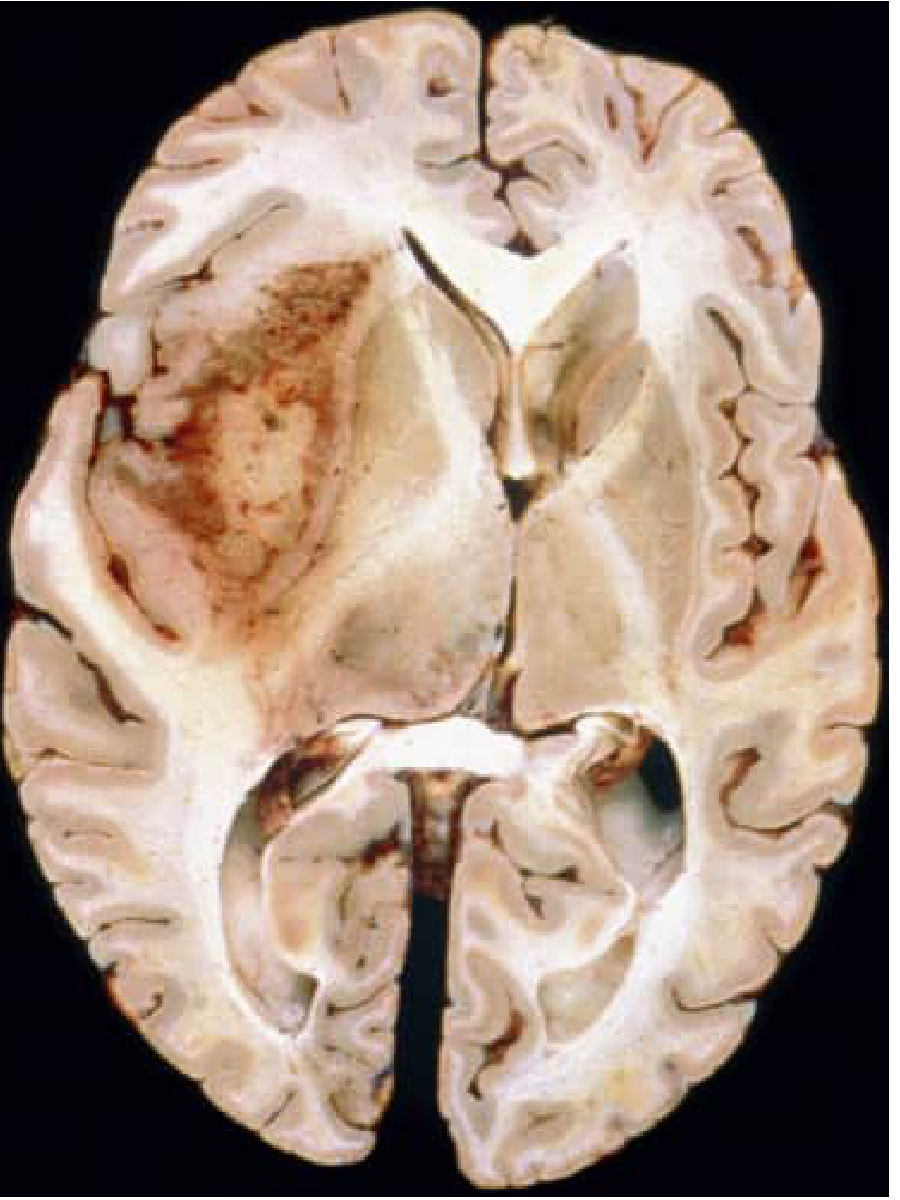
1c. Oligodendroglioma, IDH-mutant and 1p/19q-codeleted (WHO Grades 2-3)
- Uniformly round nuclei with bland chromatin
- "Fried-egg" appearance: clear perinuclear halo (formalin fixation artifact; absent in frozen sections)
- "Chicken-wire" vasculature: rich branching delicate capillary network
- Cortical involvement, microcalcifications, mucin-rich microcystic spaces, perineuronal satellitosis
- Grade 3 (anaplastic): hypercellularity, numerous mitoses, microvascular proliferation
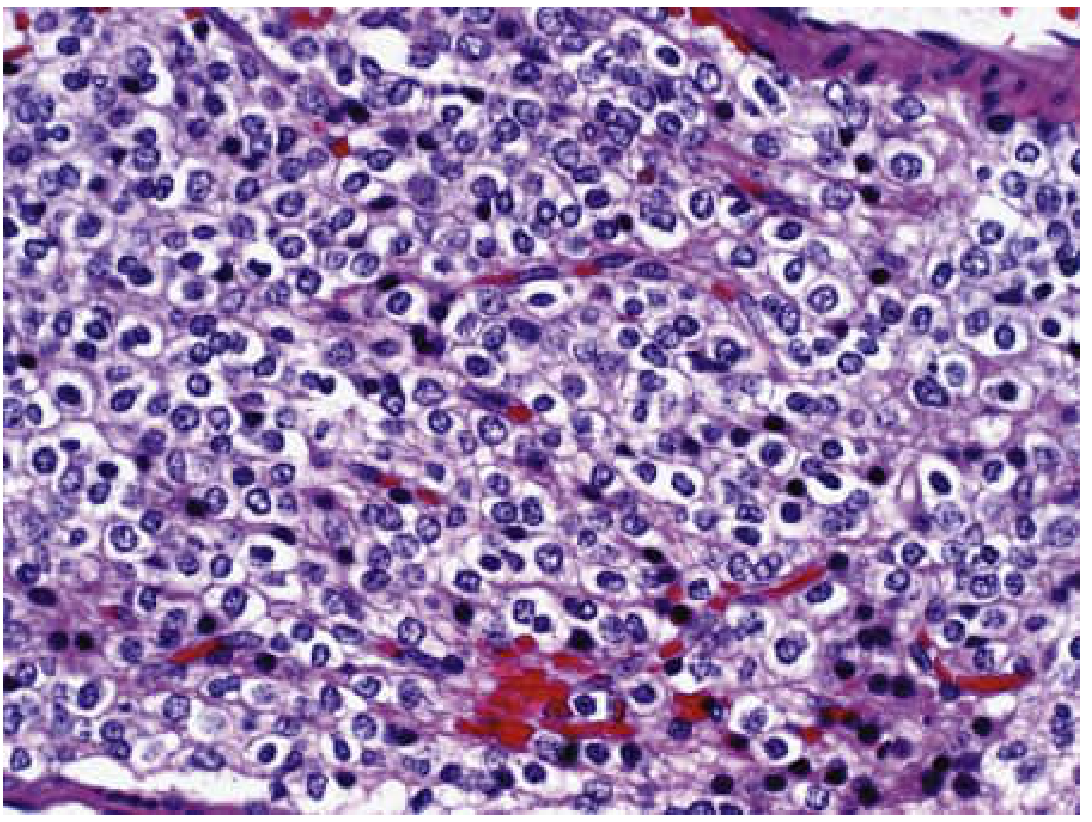
2. Pilocytic Astrocytoma (WHO Grade 1)
- KIAA1549::BRAF fusion in >70% - a defining molecular feature
- Grossly: well-demarcated cystic mass with enhancing mural nodule
- Biphasic architecture: alternating loose "microcystic" and compact densely fibrillar areas
- Bipolar cells with long thin "hair-like" (pilocytic) processes, GFAP-positive
- Rosenthal fibers: eosinophilic corkscrew-shaped inclusions (pathognomonic in context)
- Eosinophilic granular bodies (mulberry-like inclusions)
- Microvascular proliferation and necrosis do NOT imply worse prognosis (unlike diffuse gliomas)
3. Ependymoma (WHO Grades 2-3; Subependymoma Grade 1)
- Supratentorial: often ZFTA::RELA fusion (poor prognosis) or YAP1 fusion (better prognosis)
- Posterior fossa type A (PFA): H3K27me3 loss by IHC (poor prognosis)
- Posterior fossa type B (PFB): H3K27me3 retained (better prognosis)
- Spinal: NF2 mutation; rare MYCN-amplified (poor prognosis)
- Perivascular pseudorosettes: tumor cells arranged around blood vessels with anuclear fibrillary zones (most common)
- True ependymal rosettes/canals: tumor cells around central lumen (pathognomonic but less common)
- GFAP-positive fibrillary background
- Solid, non-infiltrative masses (unlike diffuse gliomas)
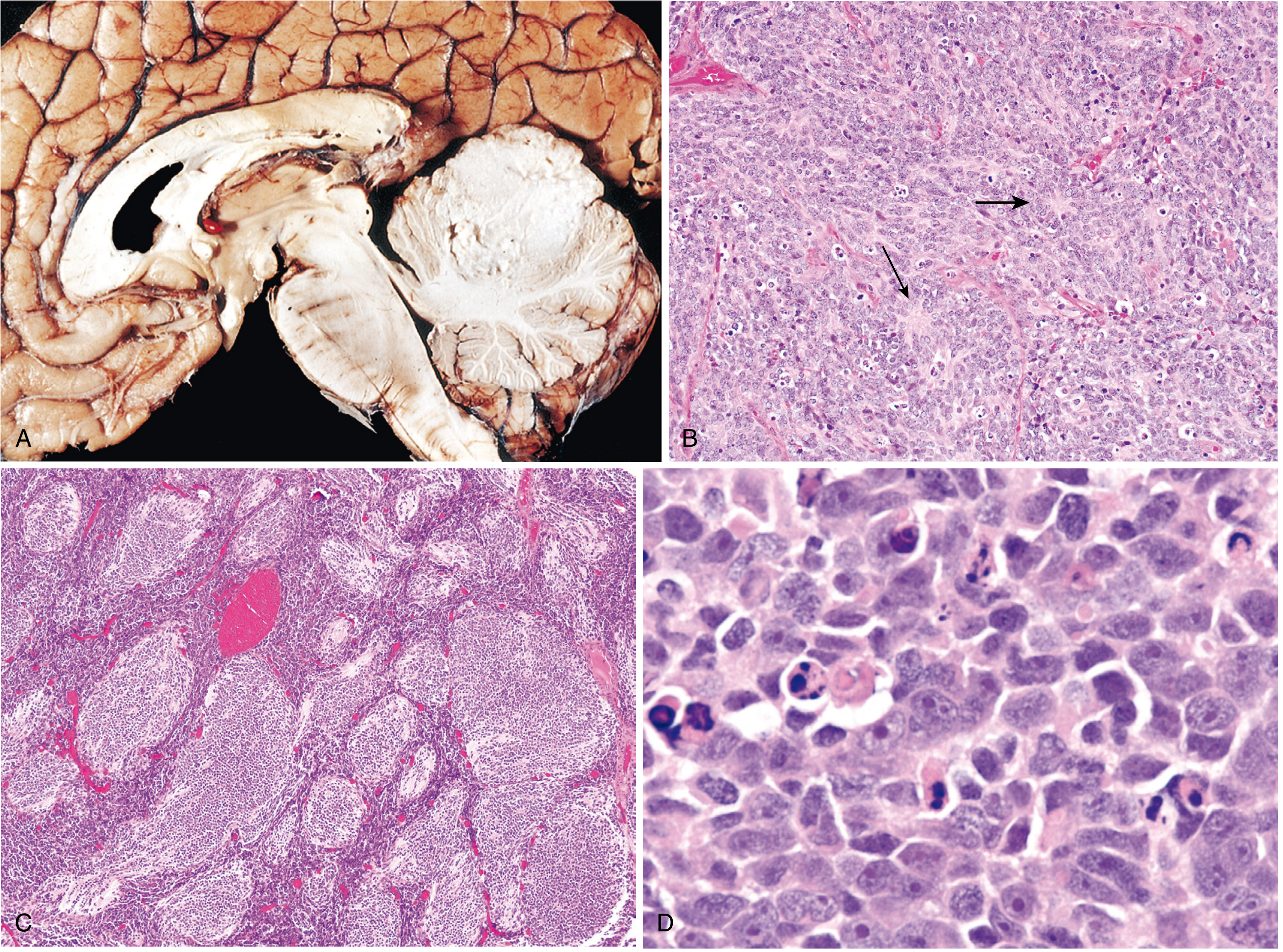
4. Medulloblastoma (WHO Grades 3-4 equivalent)
| Group | Prognosis | Key Features |
|---|---|---|
| WNT-activated | ~100% 5-year survival | CTNNB1 mutation, monosomy 6 |
| SHH-activated | Intermediate | PTCH1/SMO mutations; TP53 mut (worse) |
| Group 3 | Poor (20-30% survival) | MYC amplification; metastatic |
| Group 4 | Intermediate | Most common; isochromosome 17q |
- Classic: sheets of small round blue cells (SRBCT), Homer-Wright rosettes (incomplete rosettes around neuropil)
- Desmoplastic/nodular: pale "islands" surrounded by dense desmoplastic stroma (nodules = reticulin-poor)
- Large cell/anaplastic: large cells with prominent nucleoli + nuclear molding (worst prognosis)
- MBEN (medulloblastoma with extensive nodularity): florid nodular pattern, excellent prognosis in infants
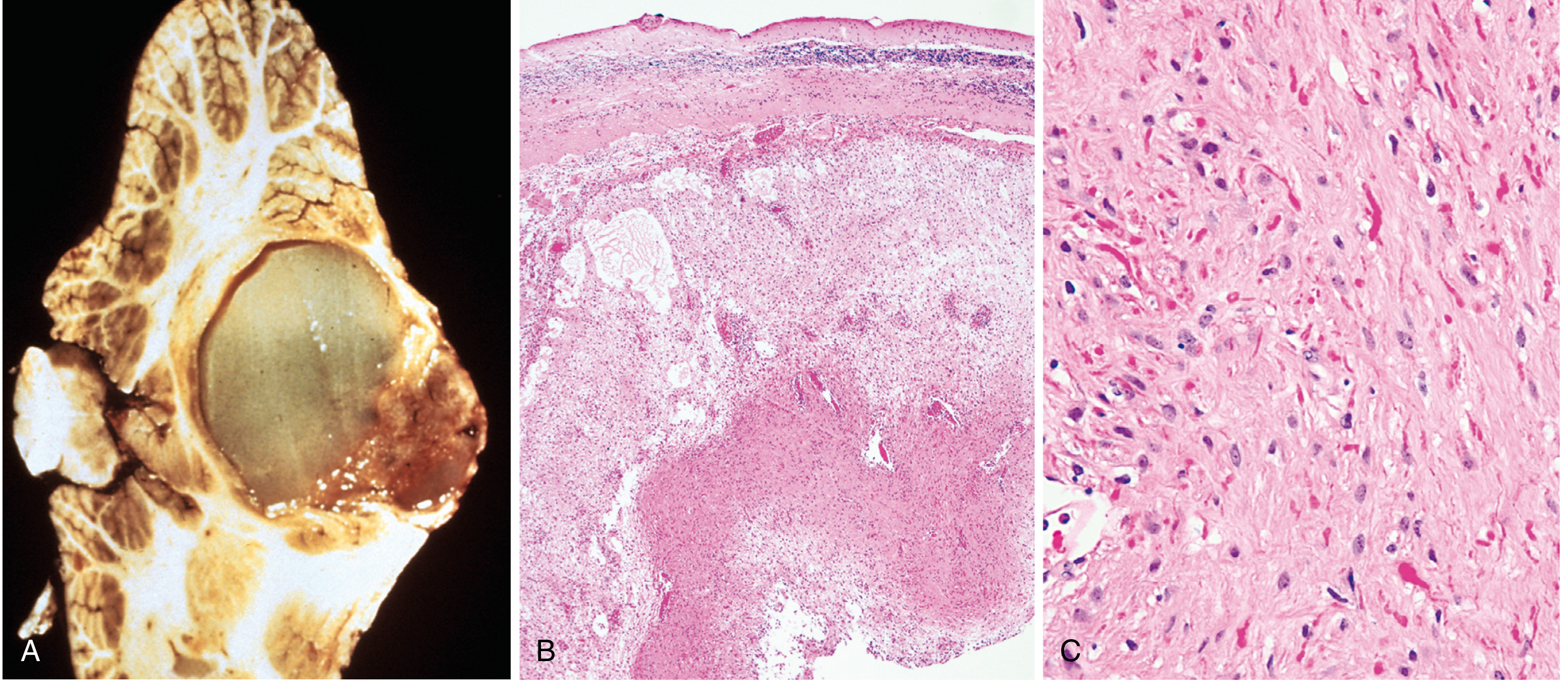
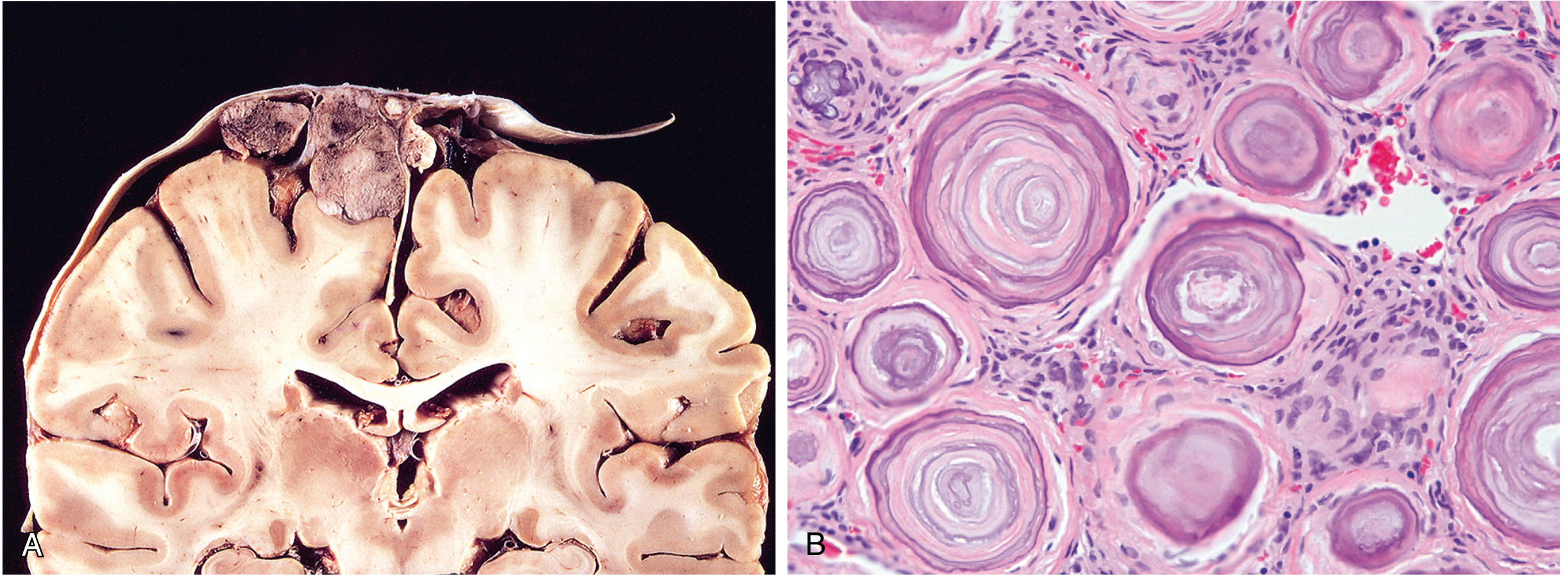
5. Meningioma (WHO Grades 1-3)
- Meningothelial: clusters of epithelioid cells with indiscernible cell membranes
- Fibroblastic: intersecting fascicles of spindled cells + abundant collagen
- Transitional: mixed features with numerous whorls
- Psammomatous: abundant psammoma bodies (concentric calcified rings)
- Secretory, microcystic, lymphoplasmacyte-rich, angiomatous (others)
6. Primary CNS Lymphoma
- 2% of extranodal lymphomas; most common CNS neoplasm in immunosuppressed patients
- Virtually always diffuse large B-cell lymphoma (DLBCL)
- Multifocal, periventricular, deep subcortical
- Malignant cells accumulate around blood vessels (angiocentric pattern), express CD20
- In immunosuppressed: necrosis prominent; EBV positive (EBER ISH)
- In immunocompetent: PDL1 gene amplification common; worse prognosis than nodal DLBCL
7. Metastatic Tumors
Key Molecular Tests for Pathologists (WHO 2021)
| Marker | Significance |
|---|---|
| IDH1/2 mutation | Distinguishes astrocytoma/oligodendroglioma from GBM and reactive gliosis |
| 1p/19q codeletion | Defines oligodendroglioma (combined with IDH mutation) |
| ATRX/TP53 | Supports astrocytoma lineage (mutually exclusive with 1p/19q codeletion) |
| TERT promoter mutation | Marks GBM (IDH-wt), oligodendroglioma; prognostic |
| EGFR amplification / +7/-10 | Molecular hallmarks of GBM |
| CDKN2A homozygous deletion | Upgrades IDH-mutant astrocytoma to grade 4 |
| MGMT promoter methylation | Predicts temozolomide sensitivity in GBM |
| H3K27me3 loss (IHC) | Identifies PFA ependymoma |
| KIAA1549::BRAF fusion | Diagnostic for pilocytic astrocytoma |
| CTNNB1 / WNT pathway | WNT medulloblastoma (best prognosis) |
| DNA methylation profiling | Gold standard for difficult cases; supersedes histology in ambiguous tumors |
Grading Summary Table
| Tumor | WHO Grade | Key Histologic Hallmark |
|---|---|---|
| Pilocytic astrocytoma | 1 | Biphasic, Rosenthal fibers, well-circumscribed |
| Astrocytoma, IDH-mutant | 2 | Hypercellular, nuclear atypia, infiltrative |
| Astrocytoma, IDH-mutant | 3 | + Mitoses |
| Astrocytoma, IDH-mutant | 4 | + MVP/necrosis or CDKN2A HD |
| Glioblastoma, IDH-wt | 4 | Palisading necrosis, MVP, pleomorphism |
| Oligodendroglioma | 2 | Fried-egg cells, chicken-wire vessels |
| Oligodendroglioma | 3 | + Mitoses, MVP/necrosis |
| Ependymoma | 2-3 | Perivascular pseudorosettes |
| Medulloblastoma | 4 (aggressive) | Small blue cells, Homer-Wright rosettes |
| Meningioma | 1 | Whorls, psammoma bodies |
| Meningioma | 2 (atypical) | ≥4 mitoses/10 HPF or brain invasion |
| Meningioma | 3 (anaplastic) | Carcinoma/sarcoma-like, high mitoses |
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease, p.1192-1200; Robbins & Kumar Basic Pathology, p.877; Bradley and Daroff's Neurology in Clinical Practice; Horbinski et al., JAMA Oncol 2025 (PMID: 39724142)
Make a presentation on CNS tumor classification and grading for residents
ls /home/daytona/workspace/ 2>/dev/null || echo "workspace empty or missing"
mkdir -p /home/daytona/workspace/cns-tumor-ppt
node /home/daytona/skills/shared/scripts/fetch_images.js \ "https://cdn.orris.care/cdss_images/6f73577c9233e3adefd0c9b53ef0eb6a7bcfe75d43c789bbac1b181317f8a11a.png" \ "https://cdn.orris.care/cdss_images/5833f33aa53e57e77a4a03ddd2e82641b148aa2a21088a4ad06a42800b7edea0.png" \ "https://cdn.orris.care/cdss_images/37f96dbc44eeb11f38631c2a3ab841d63066a0fb5f7e32f08568c6e99109eebc.png" \ "https://cdn.orris.care/cdss_images/f62b70f2e4b792b3b8884f75603c75c22249b01994d673ad7c62f2f3133b013b.png" \ "https://cdn.orris.care/cdss_images/a6c268be287fee328ed484f386ad2a7a9e11578826ef3453fefd365d4648cf2a.png" \ "https://cdn.orris.care/cdss_images/597da96f78bb07db065265d59617ed66fddebe4ae5f52295253ba90ef9892f2f.png" \ 2>/dev/null | node -e " const d = JSON.parse(require('fs').readFileSync('/dev/stdin','utf8')); d.forEach((r,i)=>{ if(r.error) console.log(i+': ERROR '+r.error); else console.log(i+': OK, len='+r.base64.length); }); "
~/cns-tumor-ppt/build.js
const pptxgen = require("pptxgenjs");
const { execSync } = require("child_process");
// ── Fetch all histopath images ──────────────────────────────────────────────
const imageUrls = [
"https://cdn.orris.care/cdss_images/6f73577c9233e3adefd0c9b53ef0eb6a7bcfe75d43c789bbac1b181317f8a11a.png", // 0 astrocytoma
"https://cdn.orris.care/cdss_images/5833f33aa53e57e77a4a03ddd2e82641b148aa2a21088a4ad06a42800b7edea0.png", // 1 glioblastoma
"https://cdn.orris.care/cdss_images/37f96dbc44eeb11f38631c2a3ab841d63066a0fb5f7e32f08568c6e99109eebc.png", // 2 oligodendroglioma
"https://cdn.orris.care/cdss_images/f62b70f2e4b792b3b8884f75603c75c22249b01994d673ad7c62f2f3133b013b.png", // 3 pilocytic
"https://cdn.orris.care/cdss_images/a6c268be287fee328ed484f386ad2a7a9e11578826ef3453fefd365d4648cf2a.png", // 4 medulloblastoma
"https://cdn.orris.care/cdss_images/597da96f78bb07db065265d59617ed66fddebe4ae5f52295253ba90ef9892f2f.png", // 5 meningioma
];
const imgs = JSON.parse(
execSync(
`node /home/daytona/skills/shared/scripts/fetch_images.js ${imageUrls.map(u => `"${u}"`).join(" ")}`
).toString()
);
// ── Color palette ───────────────────────────────────────────────────────────
// Deep navy (dominant) + warm white content + vivid teal accent + amber highlight
const C = {
navy: "0D1B2A", // dominant bg
navyMid: "1A2E42", // card bg
navyLight: "1E3A5F", // lighter panel
teal: "00B4D8", // primary accent
tealDark: "0077A8", // secondary accent
amber: "F4A261", // warning / highlight
red: "E05A5A", // danger / malignant
green: "52B788", // good prognosis
white: "FFFFFF",
lightGray: "D0DDE8",
mutedGray: "8AA5BD",
};
// ── Helpers ─────────────────────────────────────────────────────────────────
function darkSlide(pres) {
const s = pres.addSlide();
s.background = { color: C.navy };
return s;
}
function midSlide(pres) {
const s = pres.addSlide();
s.background = { color: C.navyMid };
return s;
}
function addSlideHeader(s, title, sub) {
// top accent bar
s.addShape("rect", { x: 0, y: 0, w: 10, h: 0.08, fill: { color: C.teal }, line: { type: "none" } });
s.addText(title, {
x: 0.4, y: 0.15, w: 9.2, h: 0.55,
fontSize: 22, bold: true, color: C.teal, fontFace: "Calibri",
});
if (sub) {
s.addText(sub, {
x: 0.4, y: 0.68, w: 9.2, h: 0.32,
fontSize: 12, color: C.mutedGray, italic: true, fontFace: "Calibri",
});
}
// divider
s.addShape("rect", { x: 0.4, y: 1.0, w: 9.2, h: 0.02, fill: { color: C.navyLight }, line: { type: "none" } });
}
function badge(s, text, x, y, color) {
s.addShape("roundRect", { x, y, w: text.length * 0.095 + 0.3, h: 0.3, fill: { color }, rectRadius: 0.08, line: { type: "none" } });
s.addText(text, { x, y, w: text.length * 0.095 + 0.3, h: 0.3, fontSize: 9, bold: true, color: C.white, align: "center", valign: "middle", fontFace: "Calibri" });
}
// ── Build presentation ───────────────────────────────────────────────────────
const pres = new pptxgen();
pres.layout = "LAYOUT_16x9";
pres.title = "CNS Tumor Classification & Grading";
pres.author = "Orris Medical Education";
// ━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
// SLIDE 1 — TITLE
// ━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
{
const s = darkSlide(pres);
s.background = { color: C.navy };
// left dark panel
s.addShape("rect", { x: 0, y: 0, w: 0.18, h: 5.625, fill: { color: C.teal }, line: { type: "none" } });
// decorative circle
s.addShape("ellipse", { x: 7.8, y: -0.6, w: 3.5, h: 3.5, fill: { color: C.navyLight }, line: { type: "none" } });
s.addShape("ellipse", { x: 8.1, y: -0.3, w: 2.9, h: 2.9, fill: { color: C.teal }, line: { type: "none" }, transparency: 85 });
s.addText("CNS TUMOR", {
x: 0.5, y: 0.9, w: 9, h: 1.0,
fontSize: 52, bold: true, color: C.white, fontFace: "Calibri",
charSpacing: 4,
});
s.addText("CLASSIFICATION & GRADING", {
x: 0.5, y: 1.85, w: 9, h: 0.75,
fontSize: 28, bold: false, color: C.teal, fontFace: "Calibri",
charSpacing: 2,
});
// subtitle bar
s.addShape("rect", { x: 0.5, y: 2.75, w: 5.5, h: 0.04, fill: { color: C.amber }, line: { type: "none" } });
s.addText("WHO 5th Edition (2021) | For Residents", {
x: 0.5, y: 2.9, w: 9, h: 0.4,
fontSize: 14, color: C.mutedGray, fontFace: "Calibri", italic: true,
});
// bottom bullets
const topics = [
"Gliomas (Astrocytoma · Glioblastoma · Oligodendroglioma)",
"Pilocytic Astrocytoma · Ependymoma · Medulloblastoma",
"Meningioma · CNS Lymphoma · Metastases",
];
s.addText(topics.map((t, i) => ({
text: "▸ " + t,
options: { breakLine: i < topics.length - 1, fontSize: 13, color: C.lightGray, fontFace: "Calibri" }
})), { x: 0.5, y: 3.55, w: 8.5, h: 1.5 });
// bottom bar
s.addShape("rect", { x: 0, y: 5.35, w: 10, h: 0.275, fill: { color: C.navyLight }, line: { type: "none" } });
s.addText("Source: Robbins & Cotran Pathologic Basis of Disease, 10e | WHO CNS Tumors 5th Ed, 2021", {
x: 0.3, y: 5.36, w: 9.4, h: 0.25, fontSize: 8, color: C.mutedGray, fontFace: "Calibri",
});
}
// ━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
// SLIDE 2 — WHY CLASSIFICATION CHANGED
// ━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
{
const s = darkSlide(pres);
addSlideHeader(s, "Why Classification Changed: WHO 2021", "The biggest shift in CNS neuropathology in decades");
// two column panels
const panels = [
{ title: "BEFORE (WHO 2016 & earlier)", color: C.navyLight, items: [
"Diagnosis based mainly on H&E morphology",
"Astrocytoma vs. Oligodendroglioma was subjective",
'Mixed "oligoastrocytoma" category existed',
"Grade determined histology alone",
"Poor reproducibility between pathologists",
]},
{ title: "NOW (WHO 2021 — 5th Edition)", color: C.tealDark, items: [
"Molecular markers are REQUIRED for diagnosis",
"IDH, 1p/19q, ATRX define tumor type",
"Oligoastrocytoma eliminated",
"Molecular features can OVERRIDE morphology for grading",
"Arabic numerals for grades (2, 3, 4 — not II, III, IV)",
]},
];
panels.forEach((p, i) => {
const x = 0.3 + i * 4.9;
s.addShape("rect", { x, y: 1.1, w: 4.6, h: 4.1, fill: { color: p.color }, line: { type: "none" }, rectRadius: 0 });
s.addText(p.title, { x: x + 0.15, y: 1.15, w: 4.3, h: 0.45, fontSize: 11, bold: true, color: i === 0 ? C.mutedGray : C.teal, fontFace: "Calibri" });
s.addText(
p.items.map((it, j) => ({ text: (i === 0 ? "✗ " : "✓ ") + it, options: { breakLine: j < p.items.length - 1, fontSize: 12.5, color: i === 0 ? C.lightGray : C.white, fontFace: "Calibri" } })),
{ x: x + 0.15, y: 1.65, w: 4.3, h: 3.3 }
);
});
// bottom callout
s.addShape("rect", { x: 0, y: 5.35, w: 10, h: 0.275, fill: { color: C.navyLight }, line: { type: "none" } });
s.addText("Key principle: Diagnosis = Histology + Molecular markers. Each confirms the other.", {
x: 0.3, y: 5.36, w: 9.4, h: 0.25, fontSize: 9, color: C.amber, bold: true, fontFace: "Calibri",
});
}
// ━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
// SLIDE 3 — OVERVIEW MAP
// ━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
{
const s = darkSlide(pres);
addSlideHeader(s, "CNS Tumor Categories — Overview", "Primary vs. secondary; parenchymal vs. extra-axial");
const cats = [
{ label: "GLIOMAS", sub: "Astrocytoma · GBM · Oligodendroglioma · Ependymoma · Pilocytic", color: C.tealDark, grade: "Gr 1–4" },
{ label: "EMBRYONAL", sub: "Medulloblastoma · ATRT · Other embryonal", color: "6B3FA0", grade: "Gr 4" },
{ label: "MENINGEAL", sub: "Meningioma (Gr 1–3) · Hemangiopericytoma", color: "2E7D5E", grade: "Gr 1–3" },
{ label: "CNS LYMPHOMA", sub: "Primary DLBCL · EBV+ in immunosuppressed", color: "8B2635", grade: "Aggressive" },
{ label: "METASTASES", sub: "Lung > Breast > Melanoma > Kidney > GI", color: "5C4A1E", grade: "Variable" },
{ label: "SELLAR / NERVE", sub: "Craniopharyngioma · Schwannoma · Pituitary adenoma", color: "1A5276", grade: "Gr 1–2" },
];
cats.forEach((c, i) => {
const col = i % 3;
const row = Math.floor(i / 3);
const x = 0.25 + col * 3.25;
const y = 1.15 + row * 2.1;
s.addShape("rect", { x, y, w: 3.0, h: 1.85, fill: { color: c.color }, line: { type: "none" } });
// top accent line
s.addShape("rect", { x, y, w: 3.0, h: 0.06, fill: { color: C.amber }, line: { type: "none" } });
s.addText(c.label, { x: x + 0.12, y: y + 0.1, w: 2.76, h: 0.42, fontSize: 13, bold: true, color: C.white, fontFace: "Calibri" });
badge(s, c.grade, x + 0.12, y + 0.52, C.navy);
s.addText(c.sub, { x: x + 0.12, y: y + 0.88, w: 2.76, h: 0.82, fontSize: 9.5, color: C.lightGray, fontFace: "Calibri", wrap: true });
});
s.addShape("rect", { x: 0, y: 5.35, w: 10, h: 0.275, fill: { color: C.navyLight }, line: { type: "none" } });
s.addText("Even low-grade tumors in eloquent locations can be fatal — location matters as much as grade.", {
x: 0.3, y: 5.36, w: 9.4, h: 0.25, fontSize: 9, color: C.mutedGray, fontFace: "Calibri",
});
}
// ━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
// SLIDE 4 — DIFFUSE GLIOMAS COMPARISON TABLE
// ━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
{
const s = darkSlide(pres);
addSlideHeader(s, "Diffuse Gliomas — Diagnostic Comparison", "Three separate entities; defined by both morphology and molecular markers");
const rows = [
["Feature", "Astrocytoma, IDH-mutant", "Oligodendroglioma", "Glioblastoma, IDH-wt"],
["IDH status", "Mutant (IDH1/2)", "Mutant (IDH1/2)", "Wildtype"],
["Other key markers", "TP53 mut + ATRX loss", "1p/19q codeletion (BOTH required)", "+7/−10, TERT-mut, EGFR-amp"],
["WHO grades", "2, 3, 4", "2 or 3 only", "4 (by definition)"],
["Typical location", "Cerebral hemispheres", "Frontal / temporal lobes", "Cerebral hemispheres, BG, thalamus"],
["Peak age", "Young-middle adult (med. 38 yr)", "4th–5th decade", "Adults >55 yr"],
["Key histology", "Nuclear atypia, mitoses (Gr3), MVP+necrosis (Gr4)", "Fried-egg cells, chicken-wire vessels", "Palisading necrosis, glomeruloid MVP"],
["Prognosis", "Gr2 >10 yr; Gr4 ~2–4 yr", "Gr2 >10 yr (best among diffuse)", "~15 months median"],
];
const colW = [2.2, 2.4, 2.4, 2.5];
const colX = [0.25, 2.5, 4.95, 7.4];
const rowH = 0.48;
const headerY = 1.1;
rows.forEach((row, ri) => {
const isHeader = ri === 0;
row.forEach((cell, ci) => {
const y = headerY + ri * rowH;
const fillColor = isHeader ? C.tealDark : (ri % 2 === 0 ? C.navyLight : C.navy);
s.addShape("rect", { x: colX[ci], y, w: colW[ci] - 0.05, h: rowH - 0.03, fill: { color: fillColor }, line: { type: "none" } });
s.addText(cell, {
x: colX[ci] + 0.1, y: y + 0.04, w: colW[ci] - 0.25, h: rowH - 0.08,
fontSize: isHeader ? 11 : 10,
bold: isHeader || ci === 0,
color: isHeader ? C.white : (ci === 0 ? C.teal : C.lightGray),
fontFace: "Calibri", valign: "middle", wrap: true,
});
});
});
s.addShape("rect", { x: 0, y: 5.35, w: 10, h: 0.275, fill: { color: C.navyLight }, line: { type: "none" } });
s.addText("MGMT promoter methylation (GBM) predicts temozolomide sensitivity — must report in GBM. | Robbins & Cotran Table 28.5", {
x: 0.3, y: 5.36, w: 9.4, h: 0.25, fontSize: 8, color: C.mutedGray, fontFace: "Calibri",
});
}
// ━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
// SLIDE 5 — ASTROCYTOMA HISTOPATHOLOGY
// ━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
{
const s = darkSlide(pres);
addSlideHeader(s, "Astrocytoma, IDH-mutant — Histopathology", "Infiltrative glioma; grading within a single entity (Grades 2–4)");
// image left
if (!imgs[0].error) {
s.addImage({ data: imgs[0].base64, x: 0.25, y: 1.1, w: 5.2, h: 3.3 });
}
// caption under image
s.addText("Fig. A: Coronal section — left frontal WM expansion; blurred GM-WM junction\nFig. B: Hyperchromatic irregular nuclei in fibrillary matrix; IDH1 R132H immunostain (inset)", {
x: 0.25, y: 4.45, w: 5.2, h: 0.75, fontSize: 8.5, color: C.mutedGray, fontFace: "Calibri", italic: true,
});
// right panel — grading criteria
const grades = [
{ g: "Grade 2", items: ["Nuclear atypia (enlarged, irregular, hyperchromatic nuclei)", "Hypercellular vs. normal white matter", "GFAP+ fibrillary background", "IDH1 R132H IHC positive in ~90%"] },
{ g: "Grade 3", items: ["+ Readily detectable mitotic activity", "Increased cell density"] },
{ g: "Grade 4", items: ["+ Microvascular proliferation (MVP)", "+ Necrosis", "OR homozygous CDKN2A deletion (even without MVP/necrosis)"] },
];
const gradeColors = [C.green, C.amber, C.red];
let yOffset = 1.1;
grades.forEach((gr, i) => {
s.addShape("rect", { x: 5.65, y: yOffset, w: 4.1, h: 0.35, fill: { color: gradeColors[i] }, line: { type: "none" } });
s.addText(gr.g, { x: 5.75, y: yOffset + 0.04, w: 3.9, h: 0.28, fontSize: 13, bold: true, color: C.navy, fontFace: "Calibri" });
yOffset += 0.38;
s.addShape("rect", { x: 5.65, y: yOffset, w: 4.1, h: gr.items.length * 0.32 + 0.1, fill: { color: C.navyLight }, line: { type: "none" } });
s.addText(
gr.items.map((it, j) => ({ text: "• " + it, options: { breakLine: j < gr.items.length - 1, fontSize: 10.5, color: C.lightGray, fontFace: "Calibri" } })),
{ x: 5.78, y: yOffset + 0.05, w: 3.85, h: gr.items.length * 0.32 }
);
yOffset += gr.items.length * 0.32 + 0.2;
});
s.addShape("rect", { x: 0, y: 5.35, w: 10, h: 0.275, fill: { color: C.navyLight }, line: { type: "none" } });
s.addText("Robbins, Cotran & Kumar Pathologic Basis of Disease, Fig. 28.46", {
x: 0.3, y: 5.36, w: 9.4, h: 0.25, fontSize: 8, color: C.mutedGray, fontFace: "Calibri",
});
}
// ━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
// SLIDE 6 — GLIOBLASTOMA HISTOPATHOLOGY
// ━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
{
const s = darkSlide(pres);
addSlideHeader(s, "Glioblastoma, IDH-wildtype (WHO Grade 4)", "Most common primary malignant brain tumor in adults; ~15 months median survival");
if (!imgs[1].error) {
s.addImage({ data: imgs[1].base64, x: 0.25, y: 1.1, w: 5.6, h: 3.7 });
}
s.addText("Fig. A: Necrotic, hemorrhagic infiltrating mass\nFig. B: Serpiginous palisading necrosis; inset — microvascular proliferation (glomeruloid bodies)\n\nRobbins & Kumar Basic Pathology, Fig. 21.31", {
x: 0.25, y: 4.85, w: 5.6, h: 0.65, fontSize: 8.5, color: C.mutedGray, fontFace: "Calibri", italic: true,
});
// right panel
const features = [
{ title: "Hallmark Histologic Features", items: ["Serpiginous / pseudopalisading necrosis", "Microvascular proliferation (glomeruloid bodies)", "High cellularity + marked nuclear pleomorphism", "Brisk mitotic activity"] },
{ title: "Molecular Criteria (any 1 = Grade 4)", items: ["TERT promoter mutation", "EGFR amplification", "+7/−10 chromosome copy-number change", "IDH-wildtype (required — if IDH mut → astrocytoma)"] },
{ title: "Clinical Pearls", items: ["Ring-enhancing on MRI (leaky BBB)", '"Butterfly glioma" — crosses corpus callosum', "MGMT methylation → better TMZ response", "Median OS ~15–18 months with maximal therapy"] },
];
let yy = 1.1;
features.forEach((f, i) => {
const ht = f.items.length * 0.31 + 0.44;
s.addShape("rect", { x: 6.1, y: yy, w: 3.65, h: ht, fill: { color: C.navyLight }, line: { type: "none" } });
s.addShape("rect", { x: 6.1, y: yy, w: 3.65, h: 0.03, fill: { color: i === 0 ? C.red : i === 1 ? C.teal : C.amber }, line: { type: "none" } });
s.addText(f.title, { x: 6.2, y: yy + 0.06, w: 3.45, h: 0.3, fontSize: 10, bold: true, color: i === 0 ? C.red : i === 1 ? C.teal : C.amber, fontFace: "Calibri" });
s.addText(
f.items.map((it, j) => ({ text: "• " + it, options: { breakLine: j < f.items.length - 1, fontSize: 9.8, color: C.lightGray, fontFace: "Calibri" } })),
{ x: 6.2, y: yy + 0.38, w: 3.45, h: f.items.length * 0.31 }
);
yy += ht + 0.08;
});
s.addShape("rect", { x: 0, y: 5.35, w: 10, h: 0.275, fill: { color: C.navyLight }, line: { type: "none" } });
s.addText("Even without necrosis/MVP: IDH-wt + TERT-mut OR EGFR-amp OR +7/−10 = GBM Grade 4 by molecular criteria", {
x: 0.3, y: 5.36, w: 9.4, h: 0.25, fontSize: 8.5, color: C.amber, bold: true, fontFace: "Calibri",
});
}
// ━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
// SLIDE 7 — OLIGODENDROGLIOMA
// ━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
{
const s = darkSlide(pres);
addSlideHeader(s, "Oligodendroglioma, IDH-mutant & 1p/19q-codeleted", "Best prognosis among diffuse gliomas; defined by a DUAL molecular signature");
if (!imgs[2].error) {
s.addImage({ data: imgs[2].base64, x: 0.25, y: 1.1, w: 4.8, h: 4.0 });
}
s.addText('"Fried-egg" cells: uniform round nuclei + clear perinuclear halos\n"Chicken-wire" capillary network | H&E ×200\nBradley & Daroff Neurology in Clinical Practice, Fig. 72.2', {
x: 0.25, y: 5.1, w: 4.8, h: 0.45, fontSize: 8, color: C.mutedGray, fontFace: "Calibri", italic: true,
});
// right side
const points = [
{ head: "DIAGNOSTIC CRITERIA (both required)", col: C.teal, items: ["IDH1 or IDH2 mutation", "1p/19q codeletion (chromosomal)"] },
{ head: "KEY HISTOLOGIC FEATURES", col: C.amber, items: ['"Fried-egg" appearance (formalin artifact — absent on frozen!)', '"Chicken-wire" branching capillaries', "Uniform round nuclei, bland chromatin", "Cortical involvement, microcalcifications", "Perineuronal satellitosis, mucin-rich microcysts"] },
{ head: "GRADE 3 (Anaplastic) Criteria", col: C.red, items: ["Hypercellularity + numerous mitoses", "Microvascular proliferation and/or necrosis"] },
{ head: "CLINICAL", col: C.green, items: ["5–15% of gliomas; 4th–5th decade", "Frontal > temporal lobe; gyriform calcifications on CT", "Grade 2 median OS >10 years; responds well to PCV chemo"] },
];
let yy2 = 1.1;
points.forEach(p => {
const ht = p.items.length * 0.28 + 0.44;
s.addShape("rect", { x: 5.35, y: yy2, w: 4.4, h: ht, fill: { color: C.navyLight }, line: { type: "none" } });
s.addShape("rect", { x: 5.35, y: yy2, w: 4.4, h: 0.03, fill: { color: p.col }, line: { type: "none" } });
s.addText(p.head, { x: 5.45, y: yy2 + 0.06, w: 4.2, h: 0.3, fontSize: 10, bold: true, color: p.col, fontFace: "Calibri" });
s.addText(
p.items.map((it, j) => ({ text: "• " + it, options: { breakLine: j < p.items.length - 1, fontSize: 9.8, color: C.lightGray, fontFace: "Calibri" } })),
{ x: 5.45, y: yy2 + 0.38, w: 4.2, h: p.items.length * 0.28 }
);
yy2 += ht + 0.07;
});
s.addShape("rect", { x: 0, y: 5.35, w: 10, h: 0.275, fill: { color: C.navyLight }, line: { type: "none" } });
s.addText("The 'fried-egg' appearance is a fixation artifact — NOT present in intraoperative frozen sections. Don't let this trip you up!", {
x: 0.3, y: 5.36, w: 9.4, h: 0.25, fontSize: 8.5, color: C.amber, bold: true, fontFace: "Calibri",
});
}
// ━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
// SLIDE 8 — PILOCYTIC ASTROCYTOMA
// ━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
{
const s = darkSlide(pres);
addSlideHeader(s, "Pilocytic Astrocytoma (WHO Grade 1)", "Circumscribed glioma — NOT a diffuse glioma; excellent prognosis with surgery alone");
if (!imgs[3].error) {
s.addImage({ data: imgs[3].base64, x: 0.25, y: 1.1, w: 5.6, h: 3.6 });
}
s.addText("Fig. A: Cerebellar cyst with enhancing mural nodule | Fig. B: Biphasic architecture (loose + compact) | Fig. C: Rosenthal fibers (eosinophilic corkscrew inclusions)\nRobbins, Cotran & Kumar Pathologic Basis of Disease, Fig. 28.50", {
x: 0.25, y: 4.75, w: 5.6, h: 0.55, fontSize: 8, color: C.mutedGray, fontFace: "Calibri", italic: true,
});
const cols = [
{ head: "LOCATION & AGE", col: C.teal, items: ["Children & young adults (peak <20 yr)", "Cerebellum > optic pathway > hypothalamus > brainstem", "Associated with NF1 (optic pathway gliomas)"] },
{ head: "HISTOLOGIC HALLMARKS", col: C.amber, items: ["Biphasic pattern: loose microcystic + dense compact fibrillary", "Bipolar spindle cells with 'hairlike' GFAP+ processes", "Rosenthal fibers (corkscrew eosinophilic inclusions)", "Eosinophilic granular bodies (mulberry inclusions)", "⚠ MVP & necrosis do NOT indicate high grade here!"] },
{ head: "MOLECULAR & PROGNOSIS", col: C.green, items: ["KIAA1549::BRAF fusion in >70% (diagnostic marker)", "WHO grade 1 — curable by complete resection", "10-year OS >90% in most series", "Distinct from IDH-mutant astrocytoma — different entity entirely"] },
];
let yy3 = 1.1;
cols.forEach(c => {
const ht = c.items.length * 0.295 + 0.44;
s.addShape("rect", { x: 6.1, y: yy3, w: 3.65, h: ht, fill: { color: C.navyLight }, line: { type: "none" } });
s.addShape("rect", { x: 6.1, y: yy3, w: 3.65, h: 0.03, fill: { color: c.col }, line: { type: "none" } });
s.addText(c.head, { x: 6.2, y: yy3 + 0.06, w: 3.45, h: 0.3, fontSize: 10, bold: true, color: c.col, fontFace: "Calibri" });
s.addText(
c.items.map((it, j) => ({ text: "• " + it, options: { breakLine: j < c.items.length - 1, fontSize: 9.5, color: C.lightGray, fontFace: "Calibri" } })),
{ x: 6.2, y: yy3 + 0.38, w: 3.45, h: c.items.length * 0.295 }
);
yy3 += ht + 0.07;
});
s.addShape("rect", { x: 0, y: 5.35, w: 10, h: 0.275, fill: { color: C.navyLight }, line: { type: "none" } });
s.addText("MVP and necrosis in pilocytic astrocytoma do NOT upgrade it — unlike diffuse gliomas. Key distinction for residents!", {
x: 0.3, y: 5.36, w: 9.4, h: 0.25, fontSize: 8.5, color: C.amber, bold: true, fontFace: "Calibri",
});
}
// ━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
// SLIDE 9 — EPENDYMOMA
// ━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
{
const s = darkSlide(pres);
addSlideHeader(s, "Ependymoma — Location-Defined Classification", "WHO 2021: location + molecular subtype now part of the name");
// 3 location boxes top row
const locs = [
{ name: "SUPRATENTORIAL", items: ["ZFTA::RELA fusion (poor prognosis)", "YAP1 fusion (better prognosis)", "Hemispheric, may lack ventricular connection"], col: C.red },
{ name: "POSTERIOR FOSSA", items: ["PFA: H3K27me3 LOSS by IHC → poor prognosis", "PFB: H3K27me3 retained → better prognosis", "PFA: Children; PFB: Adults; floor of 4th ventricle"], col: C.amber },
{ name: "SPINAL CORD", items: ["NF2 mutation (spinal ependymoma)", "Most common CNS tumor in NF2", "MYCN-amplified: rare, poor prognosis"], col: C.green },
];
locs.forEach((l, i) => {
const x = 0.25 + i * 3.2;
s.addShape("rect", { x, y: 1.1, w: 3.0, h: 2.1, fill: { color: C.navyLight }, line: { type: "none" } });
s.addShape("rect", { x, y: 1.1, w: 3.0, h: 0.04, fill: { color: l.col }, line: { type: "none" } });
s.addText(l.name, { x: x + 0.1, y: 1.16, w: 2.8, h: 0.35, fontSize: 11, bold: true, color: l.col, fontFace: "Calibri" });
s.addText(
l.items.map((it, j) => ({ text: "• " + it, options: { breakLine: j < l.items.length - 1, fontSize: 9.8, color: C.lightGray, fontFace: "Calibri" } })),
{ x: x + 0.1, y: 1.55, w: 2.8, h: 1.55 }
);
});
// histology section
s.addText("HISTOLOGIC FEATURES", {
x: 0.25, y: 3.35, w: 9.5, h: 0.35, fontSize: 12, bold: true, color: C.teal, fontFace: "Calibri",
});
s.addShape("rect", { x: 0.25, y: 3.7, w: 9.5, h: 0.03, fill: { color: C.tealDark }, line: { type: "none" } });
const histItems = [
{ title: "Perivascular Pseudorosettes", desc: "Most common — tumor cells radiate around blood vessels with anuclear fibrillary zones (GFAP+). NOT specific to ependymoma but classic.", col: C.teal },
{ title: "True Ependymal Rosettes / Canals", desc: "Tumor cells arranged around a central lumen. Pathognomonic but less common. Present in about one-third of cases.", col: C.amber },
{ title: "Gross", desc: "Solid, non-infiltrative masses. Well-demarcated from surrounding brain. Arise from ventricular floor or wall.", col: C.green },
];
histItems.forEach((h, i) => {
const x = 0.25 + i * 3.2;
s.addShape("rect", { x, y: 3.78, w: 3.0, h: 1.45, fill: { color: C.navyLight }, line: { type: "none" } });
s.addText(h.title, { x: x + 0.1, y: 3.83, w: 2.8, h: 0.32, fontSize: 10, bold: true, color: h.col, fontFace: "Calibri" });
s.addText(h.desc, { x: x + 0.1, y: 4.18, w: 2.8, h: 1.0, fontSize: 9.5, color: C.lightGray, fontFace: "Calibri", wrap: true });
});
s.addShape("rect", { x: 0, y: 5.35, w: 10, h: 0.275, fill: { color: C.navyLight }, line: { type: "none" } });
s.addText("H3K27me3 loss by IHC is highly sensitive/specific for PFA ependymoma — a practical bench-side test.", {
x: 0.3, y: 5.36, w: 9.4, h: 0.25, fontSize: 8.5, color: C.amber, bold: true, fontFace: "Calibri",
});
}
// ━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
// SLIDE 10 — MEDULLOBLASTOMA
// ━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
{
const s = darkSlide(pres);
addSlideHeader(s, "Medulloblastoma — Molecular & Histologic Subtypes", "Most common malignant pediatric CNS tumor; cerebellar vermis; WHO grade 4 equivalent");
// image right
if (!imgs[4].error) {
s.addImage({ data: imgs[4].base64, x: 5.5, y: 1.1, w: 4.25, h: 3.5 });
}
s.addText("A: Cerebellar vermis mass | B: Classic type — dense SRBCT with Homer-Wright rosettes (arrows)\nC: Desmoplastic/nodular | D: Large cell/anaplastic (worst prognosis)\nRobbins, Cotran & Kumar Pathologic Basis of Disease, Fig. 28.52", {
x: 5.5, y: 4.65, w: 4.25, h: 0.6, fontSize: 7.5, color: C.mutedGray, fontFace: "Calibri", italic: true,
});
// left: molecular groups
const molGroups = [
{ name: "WNT-activated", prog: "~100% 5-yr OS", color: C.green, markers: "CTNNB1 mut, monosomy 6" },
{ name: "SHH-activated", prog: "Intermediate (TP53 mut = worse)", color: C.amber, markers: "PTCH1/SMO mut; infants + adults" },
{ name: "Group 3", prog: "20–30% 5-yr OS (worst)", color: C.red, markers: "MYC amplification; metastatic" },
{ name: "Group 4", prog: "Intermediate", color: "4A90D9", markers: "Most common; i17q; older children" },
];
s.addText("MOLECULAR GROUPS (prognosis-defining)", {
x: 0.25, y: 1.1, w: 5.0, h: 0.3, fontSize: 11, bold: true, color: C.teal, fontFace: "Calibri",
});
molGroups.forEach((mg, i) => {
const y = 1.48 + i * 0.73;
s.addShape("rect", { x: 0.25, y, w: 0.18, h: 0.6, fill: { color: mg.color }, line: { type: "none" } });
s.addShape("rect", { x: 0.48, y, w: 4.75, h: 0.6, fill: { color: C.navyLight }, line: { type: "none" } });
s.addText(mg.name, { x: 0.58, y: y + 0.04, w: 2.2, h: 0.28, fontSize: 11, bold: true, color: mg.color, fontFace: "Calibri" });
s.addText("Prognosis: " + mg.prog, { x: 0.58, y: y + 0.32, w: 4.55, h: 0.22, fontSize: 9.5, color: C.mutedGray, fontFace: "Calibri" });
s.addText(mg.markers, { x: 2.9, y: y + 0.04, w: 2.2, h: 0.28, fontSize: 9.5, color: C.lightGray, fontFace: "Calibri", italic: true });
});
// histologic subtypes
s.addText("HISTOLOGIC SUBTYPES", {
x: 0.25, y: 4.43, w: 5.0, h: 0.3, fontSize: 11, bold: true, color: C.teal, fontFace: "Calibri",
});
const hTypes = ["Classic: sheets of SRBCT + Homer-Wright rosettes | Desmoplastic/nodular: pale islands in desmoplastic stroma | MBEN: florid nodular (infants, excellent prognosis) | Large cell/anaplastic: large nuclei, nuclear molding (worst)"];
s.addText(hTypes[0], { x: 0.25, y: 4.75, w: 5.0, h: 0.5, fontSize: 9.5, color: C.lightGray, fontFace: "Calibri", wrap: true });
s.addShape("rect", { x: 0, y: 5.35, w: 10, h: 0.275, fill: { color: C.navyLight }, line: { type: "none" } });
s.addText("Medulloblastoma is exquisitely radiosensitive. WNT group may be undertreated; Group 3/4 may need intensification. Molecular subtyping is now clinical standard.", {
x: 0.3, y: 5.36, w: 9.4, h: 0.25, fontSize: 8, color: C.mutedGray, fontFace: "Calibri",
});
}
// ━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
// SLIDE 11 — MENINGIOMA
// ━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
{
const s = darkSlide(pres);
addSlideHeader(s, "Meningioma — Grading & Histologic Subtypes", "Arise from arachnoid (meningothelial) cells; most common primary intracranial tumor overall");
if (!imgs[5].error) {
s.addImage({ data: imgs[5].base64, x: 0.25, y: 1.1, w: 5.2, h: 3.4 });
}
s.addText("Fig. A: Parasagittal lobulated dural mass compressing brain (easily separable)\nFig. B: Psammomatous meningioma — whorled cells + concentric calcified psammoma bodies\nRobbins, Cotran & Kumar Pathologic Basis of Disease, Fig. 28.53", {
x: 0.25, y: 4.55, w: 5.2, h: 0.7, fontSize: 8, color: C.mutedGray, fontFace: "Calibri", italic: true,
});
const menGrades = [
{ grade: "Grade 1 (Benign) ~74%", col: C.green, items: ["Low recurrence risk; curable by resection", "Subtypes: meningothelial, fibroblastic, transitional, psammomatous, angiomatous, secretory, others", "Whorls and psammoma bodies are characteristic", "NF2 mutation most common genetic alteration"] },
{ grade: "Grade 2 (Atypical) ~25%", col: C.amber, items: ["≥4 mitoses/10 HPF OR brain invasion OR ≥3 of: hypercellularity, sheeting, macronucleoli, small cells, necrosis", "Clear cell or chordoid pattern = Grade 2 by definition", "Higher recurrence; radiation often required post-resection", "1p loss & 1q gain: emerging markers of aggressive behavior (JAMA Oncol 2025)"] },
{ grade: "Grade 3 (Anaplastic) 1–3%", col: C.red, items: ["Markedly elevated mitoses; resembles carcinoma or sarcoma", "Retains at least focal meningothelial features on IHC", "May arise de novo or from malignant progression of Grade 1/2", "Very aggressive; poor prognosis"] },
];
let yy = 1.1;
menGrades.forEach(mg => {
const ht = mg.items.length * 0.3 + 0.44;
s.addShape("rect", { x: 5.65, y: yy, w: 4.1, h: ht, fill: { color: C.navyLight }, line: { type: "none" } });
s.addShape("rect", { x: 5.65, y: yy, w: 4.1, h: 0.035, fill: { color: mg.col }, line: { type: "none" } });
s.addText(mg.grade, { x: 5.75, y: yy + 0.07, w: 3.9, h: 0.3, fontSize: 11, bold: true, color: mg.col, fontFace: "Calibri" });
s.addText(
mg.items.map((it, j) => ({ text: "• " + it, options: { breakLine: j < mg.items.length - 1, fontSize: 9.5, color: C.lightGray, fontFace: "Calibri" } })),
{ x: 5.75, y: yy + 0.4, w: 3.9, h: mg.items.length * 0.3 }
);
yy += ht + 0.07;
});
s.addShape("rect", { x: 0, y: 5.35, w: 10, h: 0.275, fill: { color: C.navyLight }, line: { type: "none" } });
s.addText("Female predominance 2:1 (spinal 10:1). Multiple meningiomas → think NF2. May grow rapidly during pregnancy (progesterone receptors).", {
x: 0.3, y: 5.36, w: 9.4, h: 0.25, fontSize: 8.5, color: C.mutedGray, fontFace: "Calibri",
});
}
// ━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
// SLIDE 12 — CNS LYMPHOMA & METASTASES
// ━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
{
const s = darkSlide(pres);
addSlideHeader(s, "CNS Lymphoma & Metastatic Tumors", "Two critically important non-glial diagnoses — know them well");
// two wide columns
const col1 = [
{ head: "PRIMARY CNS LYMPHOMA", col: C.teal },
{ text: "• 2% of extranodal lymphomas; 1% of intracranial tumors" },
{ text: "• Most common CNS neoplasm in immunosuppressed (HIV, post-transplant)" },
{ text: "• Virtually always DLBCL (diffuse large B-cell lymphoma)" },
{ text: "" },
{ subhead: "HISTOLOGY", col: C.teal },
{ text: "• Angiocentric pattern — malignant cells accumulate around blood vessels" },
{ text: "• CD20+ B-cells; high proliferative index (Ki-67)" },
{ text: "• Immunosuppressed: necrosis prominent + EBV+ by EBER ISH" },
{ text: "• Immunocompetent: PDL1 gene amplification common" },
{ text: "" },
{ subhead: "IMAGING / CLINICAL", col: C.teal },
{ text: "• Multifocal, periventricular, deep subcortical" },
{ text: "• Avid FDG-PET uptake; dense/homogeneous on CT" },
{ text: "• ⚠ DO NOT biopsy if on steroids — steroids lyse lymphoma cells, causing false negative" },
];
const col2 = [
{ head: "METASTATIC TUMORS", col: C.amber },
{ text: "• 25–50% of intracranial tumors in hospitalized patients" },
{ text: "• Top 5 primaries (80% combined):" },
{ text: " 1. Lung 2. Breast 3. Melanoma 4. Kidney 5. GI tract" },
{ text: "" },
{ subhead: "HISTOLOGY", col: C.amber },
{ text: "• Well-circumscribed masses at gray-white matter junction" },
{ text: "• Usually preserve primary tumor morphology (e.g., melanin in melanoma)" },
{ text: "• Ring-enhancing on MRI; marked surrounding edema" },
{ text: "• Multiple lesions in older patient = metastasis until proven otherwise" },
{ text: "" },
{ subhead: "IHC PANEL (to identify primary)", col: C.amber },
{ text: "• CK7/CK20, TTF-1, Napsin A (lung adeno), ER/PR/GATA3 (breast)" },
{ text: "• HMB-45, Melan-A, SOX10 (melanoma)" },
{ text: "• RCC, PAX8 (kidney); CDX2 (GI/colorectal)" },
];
[col1, col2].forEach((col, ci) => {
const x = ci === 0 ? 0.25 : 5.1;
let y = 1.12;
col.forEach(item => {
if (item.head) {
s.addShape("rect", { x, y, w: 4.6, h: 0.38, fill: { color: item.col === C.teal ? C.tealDark : "8B6914" }, line: { type: "none" } });
s.addText(item.head, { x: x + 0.1, y: y + 0.05, w: 4.4, h: 0.28, fontSize: 12, bold: true, color: C.white, fontFace: "Calibri" });
y += 0.43;
} else if (item.subhead) {
s.addText(item.subhead, { x: x + 0.1, y, w: 4.4, h: 0.28, fontSize: 10, bold: true, color: item.col, fontFace: "Calibri" });
y += 0.3;
} else if (item.text === "") {
y += 0.12;
} else {
s.addText(item.text, { x: x + 0.1, y, w: 4.4, h: 0.27, fontSize: 9.8, color: C.lightGray, fontFace: "Calibri" });
y += 0.28;
}
});
});
s.addShape("rect", { x: 0, y: 5.35, w: 10, h: 0.275, fill: { color: C.navyLight }, line: { type: "none" } });
s.addText("Never biopsy suspected CNS lymphoma while on steroids. Always check serology for systemic primary before brain biopsy.", {
x: 0.3, y: 5.36, w: 9.4, h: 0.25, fontSize: 8.5, color: C.amber, bold: true, fontFace: "Calibri",
});
}
// ━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
// SLIDE 13 — KEY MOLECULAR TESTS
// ━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
{
const s = darkSlide(pres);
addSlideHeader(s, "Essential Molecular Tests for Pathologists", "WHO 2021 requires molecular workup for most CNS tumor entities");
const tests = [
{ marker: "IDH1/2 mutation", method: "IHC (R132H) + sequencing", relevance: "Distinguishes astrocytoma/oligodendroglioma from GBM and reactive gliosis. Most important single test.", col: C.teal },
{ marker: "1p/19q codeletion", method: "FISH or NGS", relevance: "Defines oligodendroglioma (must have IDH mutation too). Both 1p AND 19q must be deleted.", col: C.teal },
{ marker: "ATRX + TP53", method: "IHC (ATRX loss + p53 overexpression)", relevance: "Supports astrocytoma lineage. Mutually exclusive with 1p/19q codeletion.", col: C.tealDark },
{ marker: "TERT promoter mutation", method: "Sequencing (hotspot C228T / C250T)", relevance: "Marks GBM (IDH-wt) and oligodendroglioma. In IDH-wt astrocytoma → upgrade to GBM.", col: C.amber },
{ marker: "EGFR amplification / +7/−10", method: "FISH / SNP array / NGS CNV", relevance: "Molecular hallmarks of GBM. Qualifies IDH-wt tumor as Grade 4 even without necrosis/MVP.", col: C.amber },
{ marker: "CDKN2A homozygous deletion", method: "FISH or NGS CNV", relevance: "Upgrades IDH-mutant astrocytoma to Grade 4, regardless of morphology.", col: C.red },
{ marker: "MGMT promoter methylation", method: "Methylation-specific PCR or pyrosequencing", relevance: "Predicts temozolomide response in GBM. Should be reported in all GBMs.", col: C.green },
{ marker: "H3K27me3 loss (IHC)", method: "IHC (H3K27me3 antibody)", relevance: "Identifies PFA ependymoma (poor prognosis). Highly sensitive and specific — practical bench test.", col: C.green },
{ marker: "KIAA1549::BRAF fusion", method: "RT-PCR or FISH or NGS RNA", relevance: "Diagnostic for pilocytic astrocytoma in >70% of cases. Guides targeted therapy (MEK/RAF inhibitors).", col: "6B3FA0" },
{ marker: "DNA methylation profiling", method: "850K array (Heidelberg classifier)", relevance: "Gold standard for difficult/ambiguous cases. Identifies >130 CNS tumor classes. Increasingly standard of care.", col: C.mutedGray },
];
const colHeaders = ["MARKER", "METHOD", "CLINICAL RELEVANCE"];
const colX = [0.25, 2.55, 4.5];
const colW = [2.2, 1.85, 5.25];
// header row
colHeaders.forEach((h, ci) => {
s.addShape("rect", { x: colX[ci], y: 1.08, w: colW[ci] - 0.05, h: 0.32, fill: { color: C.tealDark }, line: { type: "none" } });
s.addText(h, { x: colX[ci] + 0.1, y: 1.1, w: colW[ci] - 0.2, h: 0.28, fontSize: 10, bold: true, color: C.white, fontFace: "Calibri" });
});
tests.forEach((t, i) => {
const y = 1.45 + i * 0.41;
const bg = i % 2 === 0 ? C.navyLight : C.navy;
// row bg
s.addShape("rect", { x: 0.25, y, w: 9.5, h: 0.38, fill: { color: bg }, line: { type: "none" } });
// color indicator
s.addShape("rect", { x: 0.25, y, w: 0.06, h: 0.38, fill: { color: t.col }, line: { type: "none" } });
s.addText(t.marker, { x: colX[0] + 0.1, y: y + 0.05, w: colW[0] - 0.2, h: 0.28, fontSize: 9.5, bold: true, color: t.col, fontFace: "Calibri" });
s.addText(t.method, { x: colX[1] + 0.1, y: y + 0.05, w: colW[1] - 0.2, h: 0.28, fontSize: 9, color: C.lightGray, fontFace: "Calibri" });
s.addText(t.relevance, { x: colX[2] + 0.1, y: y + 0.05, w: colW[2] - 0.2, h: 0.28, fontSize: 9, color: C.lightGray, fontFace: "Calibri" });
});
s.addShape("rect", { x: 0, y: 5.35, w: 10, h: 0.275, fill: { color: C.navyLight }, line: { type: "none" } });
s.addText("Horbinski et al., JAMA Oncol 2025 (PMID 39724142): Molecular testing costs <5% of total CNS tumor care costs — yet enables accurate Dx, grading, and treatment selection.", {
x: 0.3, y: 5.36, w: 9.4, h: 0.25, fontSize: 8, color: C.mutedGray, fontFace: "Calibri",
});
}
// ━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
// SLIDE 14 — GRADING SUMMARY TABLE
// ━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
{
const s = darkSlide(pres);
addSlideHeader(s, "CNS Tumor Grading — Quick Reference Summary", "Histologic hallmarks and molecular anchors at a glance");
const rows = [
["Tumor", "Grade", "Key Histologic Hallmark", "Molecular Anchor", "Prognosis"],
["Pilocytic Astrocytoma", "1", "Biphasic; Rosenthal fibers; well-circumscribed", "KIAA1549::BRAF fusion", "Excellent (>90% OS)"],
["Astrocytoma, IDH-mutant", "2", "Nuclear atypia; fibrillary infiltrative", "IDH mut + ATRX + TP53", ">10 yr mean OS"],
["Astrocytoma, IDH-mutant", "3", "Grade 2 + mitoses", "IDH mut + ATRX + TP53", "~5–7 yr"],
["Astrocytoma, IDH-mutant", "4", "Grade 3 + MVP/necrosis OR CDKN2A HD", "IDH mut + CDKN2A HD", "~2–4 yr"],
["Glioblastoma, IDH-wt", "4", "Palisading necrosis + glomeruloid MVP", "IDH-wt + TERT/EGFR/+7−10", "~15 months"],
["Oligodendroglioma", "2", "Fried-egg + chicken-wire vessels", "IDH mut + 1p/19q codeletion", ">10 yr"],
["Oligodendroglioma", "3", "Grade 2 + mitoses + MVP/necrosis", "IDH mut + 1p/19q codeletion", "~3–5 yr"],
["Ependymoma (PFB/spinal)", "2", "Perivascular pseudorosettes", "NF2 mut (spinal); PFB", "Intermediate-good"],
["Ependymoma (PFA/RELA)", "2–3", "Pseudorosettes ± true rosettes", "H3K27me3 loss / ZFTA::RELA", "Poor"],
["Medulloblastoma (WNT)", "4 equiv.", "Sheets SRBCT + Homer-Wright rosettes", "CTNNB1 mut, monosomy 6", "~100% 5-yr OS"],
["Medulloblastoma (Gr3/LC-A)", "4 equiv.", "Large cells, nuclear molding", "MYC amplification", "20–30% 5-yr OS"],
["Meningioma", "1", "Whorls, psammoma bodies", "NF2 mut (most common)", "Curable by resection"],
["Meningioma (atypical)", "2", "≥4 mit/10HPF or brain invasion", "TERT mut, 1p loss emerging", "Higher recurrence"],
["Meningioma (anaplastic)", "3", "Sarcoma/carcinoma-like; high mitoses", "Complex genomics", "Poor"],
];
const colW2 = [2.2, 0.55, 2.55, 2.3, 1.95];
const colX2 = [0.15, 2.4, 3.0, 5.6, 7.95];
const rh = 0.305;
const gradeColors2 = { "1": C.green, "2": C.teal, "3": C.amber, "4": C.red, "4 equiv.": C.red, "2–3": C.amber };
rows.forEach((row, ri) => {
const isHeader = ri === 0;
const y = 1.1 + ri * rh;
const bg = isHeader ? C.tealDark : (ri % 2 === 0 ? C.navyLight : C.navy);
s.addShape("rect", { x: 0.15, y, w: 9.75, h: rh - 0.015, fill: { color: bg }, line: { type: "none" } });
row.forEach((cell, ci) => {
const isGrade = ci === 1 && !isHeader;
const gcol = isGrade ? (gradeColors2[cell] || C.teal) : null;
if (isGrade && gcol) {
s.addShape("rect", { x: colX2[ci], y: y + 0.03, w: colW2[ci], h: rh - 0.06, fill: { color: gcol }, line: { type: "none" }, rectRadius: 0 });
}
s.addText(cell, {
x: colX2[ci] + 0.05, y: y + 0.04, w: colW2[ci] - 0.1, h: rh - 0.08,
fontSize: isHeader ? 9.5 : 8.8,
bold: isHeader || ci === 0,
color: isHeader ? C.white : (ci === 0 ? C.lightGray : isGrade ? C.navy : C.lightGray),
fontFace: "Calibri", valign: "middle", wrap: true,
});
});
});
}
// ━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
// SLIDE 15 — SUMMARY & KEY TAKE-AWAYS
// ━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
{
const s = darkSlide(pres);
s.background = { color: C.navy };
s.addShape("rect", { x: 0, y: 0, w: 0.18, h: 5.625, fill: { color: C.teal }, line: { type: "none" } });
s.addShape("rect", { x: 0, y: 0, w: 10, h: 0.08, fill: { color: C.teal }, line: { type: "none" } });
s.addText("KEY TAKE-AWAYS", {
x: 0.4, y: 0.18, w: 9, h: 0.55,
fontSize: 26, bold: true, color: C.teal, fontFace: "Calibri", charSpacing: 3,
});
s.addShape("rect", { x: 0.4, y: 0.8, w: 4.5, h: 0.04, fill: { color: C.amber }, line: { type: "none" } });
const takeaways = [
["1", "Molecular + Morphology = Diagnosis", "H&E alone is insufficient. IDH, 1p/19q, ATRX, TERT, MGMT must be integrated for every diffuse glioma.", C.teal],
["2", "Grading is intratype, not spectrum", "GBM and astrocytoma are SEPARATE entities — not a continuum. IDH-wt astrocytoma = GBM grade 4 by definition.", C.amber],
["3", "Location defines ependymoma", "WHO 2021 renamed ependymoma subtypes by location + molecular group. H3K27me3 IHC is a practical tier-1 test.", C.green],
["4", "MVP/necrosis ≠ high grade in pilocytic", "Unlike diffuse gliomas, these features do NOT upgrade pilocytic astrocytoma. A critical exam distinction.", C.amber],
["5", "Medulloblastoma: WNT = cure; Group 3 = danger", "Molecular subtyping directly changes treatment intensity. Do not skip it.", C.red],
["6", "Steroids lyse lymphoma", "Never biopsy CNS DLBCL on steroids. Dense periventricular mass = think lymphoma first.", C.teal],
];
takeaways.forEach((t, i) => {
const col = Math.floor(i / 3);
const row = i % 3;
const x = 0.4 + col * 4.8;
const y = 1.0 + row * 1.45;
s.addShape("rect", { x, y, w: 4.5, h: 1.32, fill: { color: C.navyLight }, line: { type: "none" } });
s.addShape("rect", { x, y, w: 0.05, h: 1.32, fill: { color: t[3] }, line: { type: "none" } });
// number badge
s.addShape("ellipse", { x: x + 0.12, y: y + 0.08, w: 0.38, h: 0.38, fill: { color: t[3] }, line: { type: "none" } });
s.addText(t[0], { x: x + 0.12, y: y + 0.08, w: 0.38, h: 0.38, fontSize: 13, bold: true, color: C.navy, align: "center", valign: "middle", fontFace: "Calibri" });
s.addText(t[1], { x: x + 0.6, y: y + 0.08, w: 3.8, h: 0.35, fontSize: 11, bold: true, color: C.white, fontFace: "Calibri" });
s.addText(t[2], { x: x + 0.6, y: y + 0.46, w: 3.8, h: 0.78, fontSize: 9.8, color: C.lightGray, fontFace: "Calibri", wrap: true });
});
s.addShape("rect", { x: 0, y: 5.35, w: 10, h: 0.275, fill: { color: C.navyLight }, line: { type: "none" } });
s.addText("Sources: Robbins & Cotran Pathologic Basis of Disease 10e; Robbins Basic Pathology; Bradley & Daroff Neurology; WHO CNS Tumors 5th Ed (2021); Horbinski et al. JAMA Oncol 2025", {
x: 0.3, y: 5.36, w: 9.4, h: 0.25, fontSize: 7.5, color: C.mutedGray, fontFace: "Calibri",
});
}
// ── Write file ──────────────────────────────────────────────────────────────
const outPath = "/home/daytona/workspace/cns-tumor-ppt/CNS_Tumor_Classification_Residents.pptx";
pres.writeFile({ fileName: outPath }).then(() => {
console.log("DONE:", outPath);
}).catch(err => {
console.error("ERROR:", err.message);
process.exit(1);
});
cd /home/daytona/workspace/cns-tumor-ppt && node build.js 2>&1
cd /home/daytona/workspace/cns-tumor-ppt && \ node -e " const {execSync} = require('child_process'); const fs = require('fs'); const urls = [ 'https://cdn.orris.care/cdss_images/6f73577c9233e3adefd0c9b53ef0eb6a7bcfe75d43c789bbac1b181317f8a11a.png', 'https://cdn.orris.care/cdss_images/5833f33aa53e57e77a4a03ddd2e82641b148aa2a21088a4ad06a42800b7edea0.png', 'https://cdn.orris.care/cdss_images/37f96dbc44eeb11f38631c2a3ab841d63066a0fb5f7e32f08568c6e99109eebc.png', 'https://cdn.orris.care/cdss_images/f62b70f2e4b792b3b8884f75603c75c22249b01994d673ad7c62f2f3133b013b.png', 'https://cdn.orris.care/cdss_images/a6c268be287fee328ed484f386ad2a7a9e11578826ef3453fefd365d4648cf2a.png', 'https://cdn.orris.care/cdss_images/597da96f78bb07db065265d59617ed66fddebe4ae5f52295253ba90ef9892f2f.png', ]; urls.forEach((u,i)=>{ const out = \`img\${i}.png\`; execSync(\`curl -s -o \${out} \"\${u}\"\`); console.log(i, fs.statSync(out).size); }); " 2>&1
~/cns-tumor-ppt/build.js
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/cns-tumor-ppt/build.js'
~/cns-tumor-ppt/build.js
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/cns-tumor-ppt/build.js'
~/cns-tumor-ppt/build.js
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/cns-tumor-ppt/build.js'
~/cns-tumor-ppt/build.js
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/cns-tumor-ppt/build.js'
~/cns-tumor-ppt/build.js
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/cns-tumor-ppt/build.js'
~/cns-tumor-ppt/build.js
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/cns-tumor-ppt/build.js'
~/cns-tumor-ppt/build.js
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/cns-tumor-ppt/build.js'
grep -n "roundRect\|addShape.*round" /home/daytona/workspace/cns-tumor-ppt/build.js | head -20
~/cns-tumor-ppt/build.js
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/cns-tumor-ppt/build.js'
cd /home/daytona/workspace/cns-tumor-ppt && node build.js 2>&1
ls -lh /home/daytona/workspace/cns-tumor-ppt/CNS_Tumor_Classification_Residents.pptx
CNS Tumor Classification Residents
Presentation · PPTX
What's inside (15 slides, dark navy + teal + amber theme):
| Slide | Content |
|---|---|
| 1 | Title slide |
| 2 | Why WHO 2021 changed — before vs. after |
| 3 | CNS tumor categories overview map |
| 4 | Diffuse gliomas comparison table (Astrocytoma / Oligodendroglioma / GBM) |
| 5 | Astrocytoma, IDH-mutant — histopathology image + grading criteria (Gr 2/3/4) |
| 6 | Glioblastoma — gross + palisading necrosis histology + molecular criteria |
| 7 | Oligodendroglioma — "fried-egg" histology image + molecular/clinical details |
| 8 | Pilocytic Astrocytoma — biphasic/Rosenthal fiber histology + WHO Gr 1 pearls |
| 9 | Ependymoma — location-defined subtypes + pseudorosettes |
| 10 | Medulloblastoma — molecular groups (WNT/SHH/Gr3/Gr4) + histologic subtypes |
| 11 | Meningioma — psammoma body histology + Grade 1/2/3 criteria |
| 12 | CNS Lymphoma & Metastases — IHC panels, clinical traps |
| 13 | Essential molecular tests table (IDH, 1p/19q, TERT, MGMT, H3K27, BRAF, etc.) |
| 14 | Full grading summary table (all entities at a glance) |
| 15 | 6 key take-aways for residents |