Carcinoma tongue in detail
Reading File
Finding Sources
Finding Sources
Searching PubMed
"tongue neoplasms"[MeSH Terms] AND "squamous cell carcinoma"[MeSH Terms]
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Reading File
Reading File
I now have comprehensive material. Let me compile the full detailed answer on Carcinoma of the Tongue.
Carcinoma of the Tongue
Overview & Anatomy
The tongue is divided into two distinct anatomical and oncological regions:
- Oral tongue (anterior 2/3) — from the tip to the circumvallate papillae; part of the oral cavity
- Base of tongue (posterior 1/3) — from the circumvallate papillae to the vallecula; part of the oropharynx
The oral tongue is a muscular structure covered by non-keratinizing squamous epithelium. Subsites include the lateral tongue, anterior tip, ventral tongue, and dorsal surface. Carcinomas arise in the epithelium and invade the deeper musculature.
Epidemiology
- Oral tongue is the second most common site of oral cancer (30% of all oral cancers)
- Most lesions (≈75%) occur on the posterolateral aspect of the oral tongue; 20% on the anterolateral ventral surface; 3–5% on the dorsal surface
- Typical patient: male, 6th–7th decade, with history of tobacco and/or alcohol use
- Increasing incidence in young patients (18 years old in 1993, up from 4% in 1971) — no clear risk factors identified; increased genetic susceptibility postulated
- At diagnosis, majority (75%) are staged T2 or smaller
Histology
- Squamous cell carcinoma (SCC) accounts for the vast majority
- Dorsal tongue differential: amyloidosis, median rhomboid glossitis, granular cell myoblastoma, erosive lichen planus
- Submucosal tongue tumors: leiomyoma, leiomyosarcoma, rhabdomyosarcoma, neurofibroma (mesenchymal origin)
- Tonsil tissue at base of tongue → may also give rise to lymphoma
Risk Factors
| Factor | Details |
|---|---|
| Tobacco | Smoking and smokeless tobacco — major risk |
| Alcohol | Synergistic with tobacco |
| HPV | Especially HPV-16/18 for base of tongue (oropharyngeal SCC) |
| Immunosuppression | Post-transplant, HIV |
| Poor oral hygiene | Possible contributing factor |
| Genetic susceptibility | Young-onset cases without traditional risk factors |
| Reverse smoking | Associated with hard palate and tongue dorsum lesions in certain populations |
Clinical Presentation
Early
- Erythroplakia (red, inflammatory lesion) — most common presentation of early SCC
- Leukoplakia (white patch) — premalignant lesion
- Painless ulcer or exophytic mass
Late / Advanced
- Painful ulcerated or exophytic mass (see clinical photo below)
- Tongue fixation (invasion of intrinsic/extrinsic muscles)
- Decreased tongue sensation (lingual nerve invasion)
- Deviation on tongue protrusion, fasciculations, atrophy (hypoglossal nerve invasion)
- Alteration in speech and swallowing
- Referred otalgia (via lingual nerve → auriculotemporal nerve)
- Cervical lymphadenopathy
Base of Tongue (BOT) Specific
- Most common: referred otalgia and odynophagia
- Visualization is difficult → early detection is rare
- HPV+ BOT cancer: frequently presents with cervical lymphadenopathy with small primary (occult primary)

Local Invasion Patterns
- Anterolateral tongue → spreads medially across central raphe to contralateral side, posteriorly to tongue base, inferiorly into suprahyoid muscles
- Inferolateral spread → involves floor of mouth (common)
- Lingual nerve invasion → loss of dorsal tongue sensation
- Hypoglossal nerve invasion → deviation, atrophy, fasciculations
- Extreme lateral extension → direct invasion of mandible → requires composite resection
- BOT tumors → invade larynx, tonsil, soft palate, hypopharynx
Staging (AJCC 8th Edition)
T-Staging (Oral Cavity — incorporates Depth of Invasion)
| T | Criteria |
|---|---|
| Tis | Carcinoma in situ |
| T1 | ≤2 cm and DOI ≤5 mm |
| T2 | ≤2 cm with DOI >5 mm & ≤10 mm; OR >2 cm and ≤4 cm with DOI ≤10 mm |
| T3 | >4 cm in size; OR any tumor with DOI >10 mm |
| T4a | Invades cortical bone, deep tongue/extrinsic muscles, maxillary sinus, skin of face |
| T4b | Invades masticator space, pterygoid plates, skull base, or encases internal carotid artery |
Key update (AJCC 8th ed.): Depth of Invasion (DOI) was added to T-staging. Thin tumors (<2 mm DOI) have minimal regional metastatic potential; thick tumors (>8–9 mm) have significantly higher risk. - Mulholland & Greenfield's Surgery, p. 1997
N-Staging (Oral Cavity / HPV-negative)
| N | Criteria |
|---|---|
| N0 | No regional lymph node metastasis |
| N1 | Single ipsilateral node ≤3 cm, ENE(–) |
| N2a | Single ipsilateral node >3 cm and ≤6 cm, ENE(–) |
| N2b | Multiple ipsilateral nodes ≤6 cm, ENE(–) |
| N2c | Bilateral or contralateral nodes ≤6 cm, ENE(–) |
| N3a | Any node >6 cm, ENE(–) |
| N3b | Any node with clinically overt ENE(+) |
ENE = Extranodal Extension
Overall Stage Grouping
| Stage | T | N | M |
|---|---|---|---|
| I | T1 | N0 | M0 |
| II | T2 | N0 | M0 |
| III | T3 | N0 | M0; or T1–T3 N1 M0 |
| IVA | T4a N0–N1 M0; or T1–T4a N2 M0 | ||
| IVB | T4b any N M0; or any T N3 M0 | ||
| IVC | Any T, Any N, M1 |
Lymphatic Drainage & Regional Metastasis
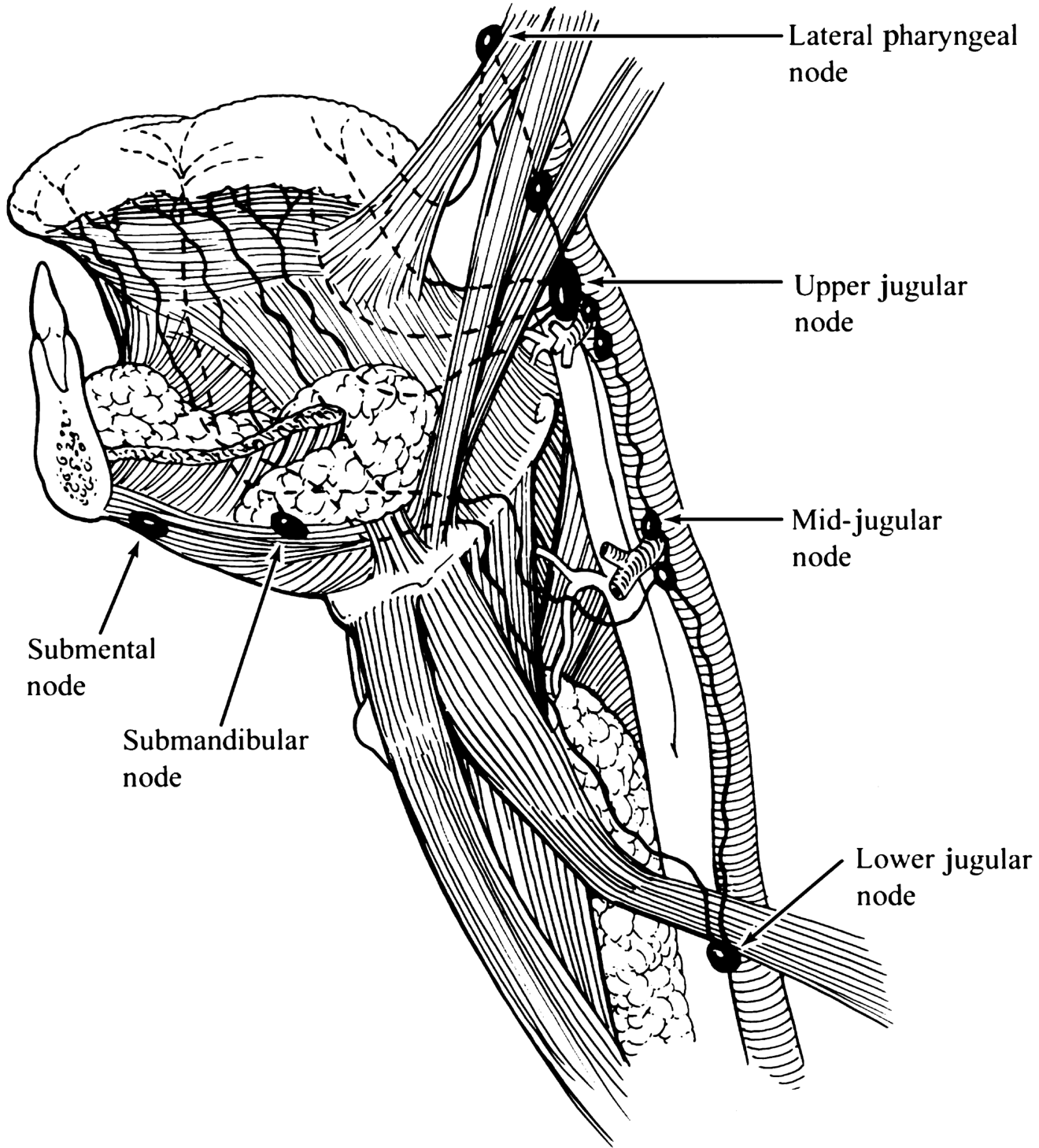
Primary drainage (oral tongue) → Levels I–III:
- Upper jugular nodes (73%)
- Submandibular nodes (18%)
- Middle jugular nodes (18%)
- Submental nodes (9%)
Key facts:
- 25–33% of lymph node metastases are clinically detectable; 20–25% are occult
- Incidence depends on tumor size and depth of invasion
- Midline dorsum or ventral tongue → bilateral cervical metastasis risk
- Base of tongue → levels II–IV; >60% have detectable nodes at presentation, 20% bilateral
- Distant metastasis in oropharyngeal cancer: ~15–20% (screen with chest CT or PET/CT)
Prognostic Factors
| Factor | Impact |
|---|---|
| Depth of invasion >2–4 mm | Higher regional metastasis, recurrence, mortality |
| Positive surgical margin | Major independent predictor of recurrence |
| Perineural invasion | Worse prognosis |
| Extracapsular spread (ECS/ENE) | Markedly worse survival |
| Nodal metastasis | Fivefold increased risk of dying of disease (occult mets) |
| Tumor differentiation | Poorly differentiated → higher occult nodal rate |
ECS and survival impact (from MSKCC data):
- pN–: 5-year DSS 88%, OS 75%
- pN+/ECS–: 5-year DSS 65%, OS 50%
- pN+/ECS+: 5-year DSS 48%, OS 30%
Diagnosis & Workup
- History & physical examination — thorough oral examination, bimanual palpation
- Biopsy — most lesions amenable to office biopsy; frozen sections intraoperatively
- Imaging:
- CT neck with contrast — assess primary extent, bone involvement, nodal disease
- MRI — superior for soft tissue invasion, perineural spread
- PET/CT — for advanced disease, detect distant metastasis
- Intraoral ultrasound — assess depth of invasion (hypoechoic irregular tumor)
- Panendoscopy — to rule out synchronous primaries
- Cranial nerve examination — CN V, VII, X, XII
Treatment
Oral Tongue
Surgery — Primary Modality
| Extent | Procedure |
|---|---|
| T1/T2 small | Transoral wide local excision (partial glossectomy) |
| Primary closure | For resection of ~1/4 to 1/3 of tongue |
| With floor of mouth | Skin graft or dermal graft to prevent tethering |
| ~1/2 tongue resection | Radial forearm or anterolateral thigh free flap |
| Near mandible | Pull-through or mandibulotomy approach |
| Cortical bone erosion | Marginal mandibulectomy (periosteum as deep margin) |
| Medullary bone invasion | Segmental mandibulectomy |
| Extensive local disease | Near-total or total glossectomy ± laryngectomy |
Reconstruction: Palatal augmentation prosthesis, fasciocutaneous free flaps (radial forearm, ALT), pectoralis major (pedicled) for bulk.
Radiation
- For patients unsuitable for surgery: external beam ± brachytherapy
- Postoperative chemoradiation: positive margins, ENE, multiple positive nodes
Chemotherapy
- T4 tumors: chemoradiation considered; bone involvement usually requires surgery
- Concurrent cisplatin-based chemoradiation is standard for unresectable/adjuvant settings
Management of the Neck
| Clinical Scenario | Recommendation |
|---|---|
| DOI ≥4 mm | Elective neck treatment (surgery or radiation) |
| DOI 2–4 mm, N0 | Elective neck dissection preferred over observation |
| DOI <2 mm, carcinoma in situ | Observation may be considered |
| T1/T2, N0 (any DOI) | Sentinel lymph node biopsy — feasible and accurate |
| Selective neck dissection | At least levels I–III (supraomohyoid neck dissection) |
| Midline/ventral tongue | Bilateral neck dissections |
| N+ neck | Selective/modified radical neck dissection + adjuvant RT |
Base of Tongue Treatment
| Stage | Treatment |
|---|---|
| T1/T2 | Transoral robotic surgery (TORS) or laser ± adjuvant; or (chemo)radiation |
| T3/T4 (resectable) | Mandibular swing, composite resection, or median mandibuloglossotomy |
| Smaller lesions at base | Suprahyoid pharyngotomy |
| Advanced | Total glossectomy ± laryngectomy + free flap reconstruction |
| HPV+ | Generally favorable response to chemoradiation |
Outcomes / Prognosis
Oral Tongue (5-year survival)
| Stage | Survival |
|---|---|
| Stage I–II | 60–75% |
| Stage III–IV | 25–40% |
| After salvage for regional recurrence | 35–40% |
Locoregional control at 5 years: 91% (early-stage surgical series)
Base of Tongue (5-year survival)
| Stage | Locoregional control | Overall survival |
|---|---|---|
| Stage I–II | 75–90% | Higher |
| Stage III | 50% | Moderate |
| Stage IV | 20% | Poor |
Key Surgical Margins
- Margin of ≥2.2 mm is the threshold below which local recurrence risk substantially increases (Zanoni et al., 381 patients — adjusted HR 2.25 for margin 0.01–2.2 mm vs. HR 1.17 for 2.3–5.0 mm)
- Tumor bed sampling for frozen section has sensitivity of only 24% for detecting positive margins in early-stage tongue SCC
Complications of Treatment
| Complication | Context |
|---|---|
| Aspiration / airway compromise | Post-glossectomy; may require laryngectomy |
| Dysphagia / altered swallowing | Post-partial or total glossectomy |
| Speech impairment | Loss of tongue bulk/mobility |
| Osteoradionecrosis | Post-radiation, especially after mandibulectomy |
| Xerostomia | Post-radiation |
| Fistula | Post-surgical reconstruction |
| Hypothyroidism | Post-neck dissection + radiation |
Summary of Key Points
- Most common histology: SCC; most frequent subsite = posterolateral oral tongue
- Risk factors: tobacco + alcohol (synergistic); HPV-16 for base of tongue
- Early sign: erythroplakia; late signs: fixation, otalgia, dysphagia, lymphadenopathy
- AJCC 8th ed. incorporates DOI into T-staging — critical prognostic variable
- Primary treatment: surgery (partial glossectomy) for oral tongue; (chemo)radiation or TORS for base of tongue
- Elective neck dissection: recommended for DOI ≥4 mm even if clinically N0
- ECS dramatically worsens prognosis; drives adjuvant chemoradiation decision
- Free flap reconstruction is the standard for defects involving >1/2 tongue or floor of mouth
Sources:
- Cummings Otolaryngology Head and Neck Surgery, Chapter 91
- KJ Lee's Essential Otolaryngology, Chapter 45
- Mulholland & Greenfield's Surgery, Chapter 41
- Harrison's Principles of Internal Medicine, 22nd ed.
This is a shared conversation. Sign in to Orris to start your own chat.