ECG
Asking for Preferences
Reading File
Finding Sources
Searching Images
ECG electrocardiogram normal waves intervals
Finding Sources
Searching Images
ECG PQRST waves intervals segments diagram labeled
Reading File
Loading Image
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
I now have comprehensive material. Let me compose the full ECG overview.
ECG — Comprehensive Overview
What Is an ECG?
The electrocardiogram (ECG/EKG) records tiny potential differences on the body surface that reflect the sequence of depolarization and repolarization of the myocardium. Because different regions of the heart activate at different times (atria before ventricles, specific ventricular sequences), measurable voltage gradients arise between body-surface electrodes. — Costanzo Physiology, 7th Ed.
The Standard 12-Lead ECG
A standard recording runs for 10 seconds at 25 mm/s and 10 mm/mV. Each small box = 0.04 sec (40 ms); each large box = 0.2 sec (200 ms).
Lead groups:
| Group | Leads | Territory viewed |
|---|---|---|
| Limb leads | I, II, III | Frontal plane |
| Augmented limb | aVR, aVL, aVF | Frontal plane (augmented) |
| Precordial | V1–V6 | Horizontal plane |
Under normal sinus rhythm, P waves and QRS complexes are upright in I, II, III, aVF and inverted in aVR. — Goldman-Cecil Medicine
ECG Waveforms — What Each Represents

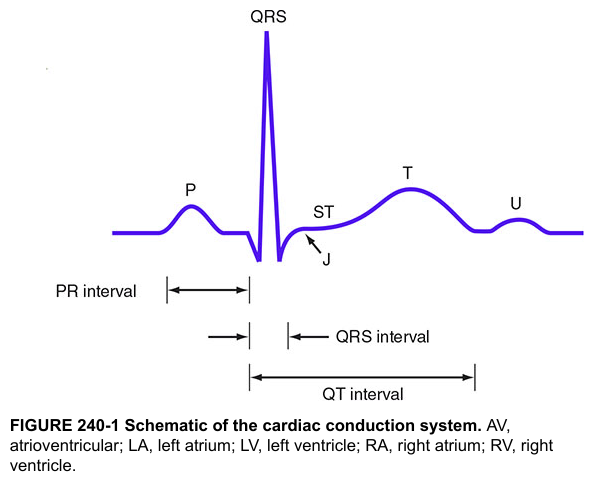
| Wave / Segment | Electrical Event |
|---|---|
| P wave | Atrial depolarization; duration reflects atrial conduction time |
| PR interval | Onset of atrial depolarization → onset of ventricular depolarization (includes AV node conduction) |
| PR segment | Isoelectric; represents AV nodal conduction delay only |
| QRS complex | Ventricular depolarization (Q = initial septal; R = main ventricular; S = terminal basal/posterior) |
| ST segment | Between end of QRS (J point) and start of T wave; normally isoelectric; represents early ventricular repolarization |
| T wave | Ventricular repolarization |
| QT interval | QRS onset → T wave end; total ventricular depolarization + repolarization time |
| U wave | Small deflection after T; thought to represent repolarization of Purkinje fibers or papillary muscles; prominent in hypokalemia |
Atrial repolarization is not visible on a normal ECG — it is buried within the QRS complex. — Costanzo Physiology
Normal Intervals
(From Goldman-Cecil Medicine, Table 42-1)
| Parameter | Normal Range |
|---|---|
| Heart rate | 50–100 bpm |
| P wave duration | < 120 ms |
| PR interval | 90–200 ms |
| QRS duration | 75–110 ms |
| QTc (males) | 390–450 ms |
| QTc (females) | 390–460 ms |
| QRS axis | −30° to +90° |
Heart rate calculation: HR (bpm) = 60,000 ÷ RR interval (ms)
Systematic Approach to ECG Interpretation
(Goldman-Cecil Medicine, Table 42-2)
- Rate — estimate heart rate
- Rhythm — regular vs. irregular
- P waves — present? morphology? 1:1 relationship with QRS?
- Pauses / premature beats — any?
- Intervals — measure PR, QRS duration, QT; calculate QTc
- Axis — estimate QRS axis in frontal plane
- P wave morphology — duration, axis
- QRS progression — R-wave progression V1→V6; transition zone (normally V3–V4)
- ST segments — elevation or depression in regional groupings (inferior: II, III, aVF; anterior: V2–V4; lateral: I, aVL, V5–V6)
- T waves — inversion, hyperacuity
Key Abnormalities at a Glance
Rhythm Disturbances
| Finding | Interpretation |
|---|---|
| No P waves, irregularly irregular RR | Atrial fibrillation |
| Sawtooth baseline ~300/min, regular RR | Atrial flutter |
| Wide QRS, no preceding P waves | Ventricular tachycardia |
| Short PR + delta wave + wide QRS | Wolff-Parkinson-White |
Conduction Blocks
| Finding | Interpretation |
|---|---|
| PR > 200 ms | 1st-degree AV block |
| Progressively lengthening PR → dropped QRS | 2nd-degree AV block, Mobitz I (Wenckebach) |
| Constant PR, intermittent dropped QRS | 2nd-degree AV block, Mobitz II |
| Complete AV dissociation | 3rd-degree (complete) AV block |
| QRS ≥ 120 ms, RsR' in V1, slurred S in I/V6 | Right bundle branch block (RBBB) |
| QRS ≥ 120 ms, broad notched R in I/V6, no septal q | Left bundle branch block (LBBB) |
Ischemia / Infarction
| Pattern | Territory |
|---|---|
| ST elevation + Q waves in II, III, aVF | Inferior MI (RCA) |
| ST elevation in V1–V4 | Anterior MI (LAD) |
| ST elevation in I, aVL, V5–V6 | Lateral MI (LCx) |
| ST elevation in aVR + diffuse depression | Left main / proximal LAD occlusion |
| Reciprocal ST depression in V1–V3 + tall R | Posterior MI |
AMI is classified by ECG into STEMI (ST-segment elevation MI) or NSTEMI (no ST elevation). Right-sided ECG leads should be obtained to detect RV infarction when inferior ST elevation is present. — Tintinalli's Emergency Medicine
QTc Prolongation
Caused by electrolyte abnormalities (hypokalemia, hypomagnesemia), drugs (antiarrhythmics, antipsychotics, antibiotics), or congenital long QT syndrome. Predisposes to torsades de pointes.
Axis Deviation
| Axis | Degrees | Causes |
|---|---|---|
| Normal | −30° to +90° | — |
| Left axis deviation (LAD) | −30° to −90° | Left anterior fascicular block, inferior MI, LVH |
| Right axis deviation (RAD) | +90° to +180° | RVH, lateral MI, left posterior fascicular block, normal in children |
To estimate axis quickly: find the lead in which QRS is most isoelectric — the axis is perpendicular to that lead.
Precordial Lead Progression
Normal R-wave progression: small r in V1 → progressively taller R waves → transition (R = S) at V3–V4 → large R in V6. Poor R-wave progression (R stays small through V4–V5) suggests anterior infarction or LVH.
This overview covers the essentials. If you need deeper coverage of any specific area — a particular arrhythmia, a specific conduction block, ischemia patterns, pediatric ECG, or drug-induced changes — just ask.
This is a shared conversation. Sign in to Orris to start your own chat.