55 year old male has BP 160/90 with no other co morbs what should be given treatment
Reading File
Finding Sources
Searching PubMed
"hypertension" AND "antihypertensive" AND "treatment"
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Reading File
I now have comprehensive information to provide a thorough answer. Here's the management for this patient:
Hypertension Management: 55-Year-Old Male, BP 160/90, No Comorbidities
Classification
BP 160/90 mmHg = Stage 2 Hypertension (SBP ≥140 or DBP ≥90 by most guidelines; ≥130/80 by ACC/AHA 2017).
Step 1 — Lifestyle Modifications (Start Immediately)
These are mandatory regardless of drug therapy and can meaningfully reduce BP:
| Modification | Recommendation | Expected SBP Reduction |
|---|---|---|
| Weight reduction | Maintain BMI 18.5–24.9 | 5–20 mmHg per 10 kg lost |
| DASH diet | Rich in fruits, vegetables, low-fat dairy; low saturated fat | 8–14 mmHg |
| Sodium restriction | ≤2.3 g/day (6 g NaCl/day) | 2–8 mmHg |
| Aerobic exercise | ≥30 min/day, most days of the week | 5–8 mmHg |
| Limit alcohol | ≤2 drinks/day for men | 2–4 mmHg |
| Stop smoking | — | Reduces overall CV risk |
Step 2 — Pharmacotherapy
Should drug therapy be started now?
Yes, immediately. With BP 160/90, this patient is >20 mmHg above the systolic goal of <130 mmHg (ACC/AHA) or >20 mmHg above 140 (ESH/NICE). Guidelines recommend starting two antihypertensives simultaneously when SBP is >20 mmHg or DBP >10 mmHg above goal.
First-Line Drug Options (Uncomplicated Hypertension)
For a non-Black patient with no comorbidities, all four classes are appropriate:
| Drug Class | Example Agent | Key Notes |
|---|---|---|
| Thiazide/Thiazide-like diuretic | Chlorthalidone 12.5–25 mg/day, HCTZ 25 mg/day | Preferred in many guidelines; monitor K⁺, uric acid, glucose |
| ACE Inhibitor | Enalapril 5–20 mg/day, Ramipril 2.5–10 mg/day | Avoid in bilateral RAS, angioedema history; monitor K⁺/creatinine |
| ARB | Losartan 50–100 mg/day, Telmisartan 40–80 mg/day | Alternative to ACE-I; avoid dual RAAS blockade |
| Calcium Channel Blocker (CCB) | Amlodipine 5–10 mg/day | Preferred if Black race or age ≥55 (NICE); well tolerated |
Note on race/age (NICE 2019): For patients ≥55 years, CCB is preferred as first-line before ACE-I/ARB, as renin levels tend to be lower. This patient at 55 years is right at this threshold — CCB (amlodipine) is a strong first choice.
Preferred Combination (Since BP is 160/90)
Since this patient is significantly above goal, start combination therapy:
ACE-I (or ARB) + CCB is the most evidence-based combination
- e.g., Ramipril 5 mg + Amlodipine 5 mg once daily
- Alternatively: ACE-I + Thiazide-like diuretic (e.g., Ramipril + Chlorthalidone)
Avoid combining two RAAS agents (e.g., ACE-I + ARB) — increased risk of renal impairment and hyperkalemia without additive BP benefit.
β-Blockers are not recommended as first-line for uncomplicated hypertension — they are less effective at stroke prevention compared to the above classes.
BP Target
<130/80 mmHg (ACC/AHA 2017, ESC 2024)
Step 3 — Follow-Up
- Reassess in 4 weeks after initiating therapy
- If BP still uncontrolled on dual therapy, add a third agent from a different class (thiazide diuretic if not already included, or spironolactone for resistant hypertension)
- Monitor serum electrolytes, creatinine, eGFR after starting ACE-I/ARB
- Check for end-organ damage: fundoscopy, ECG (LVH), urine microalbumin, renal function
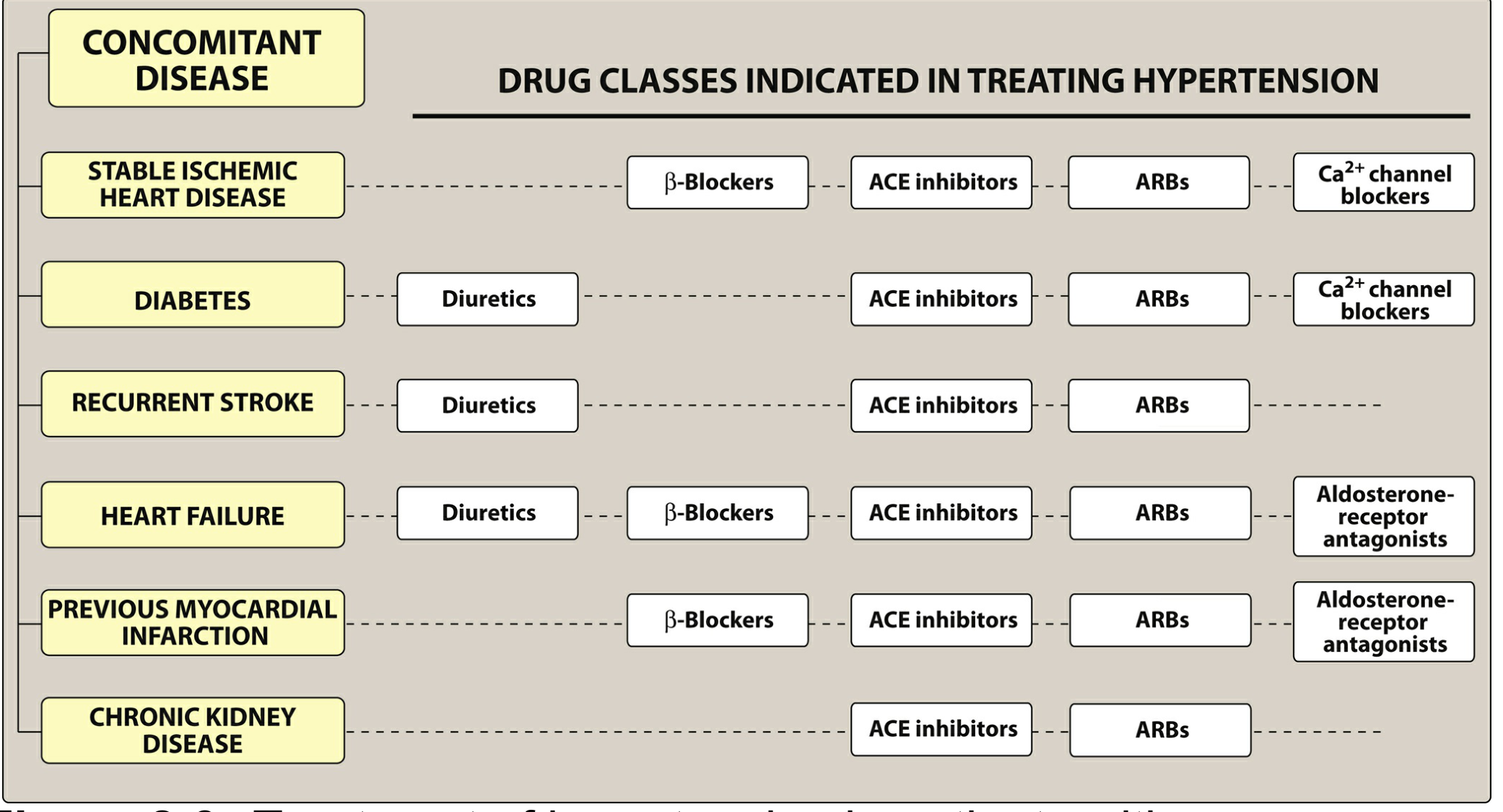
Figure: Drug class selection based on concomitant disease (applicable if comorbidities develop in future)
Sources: Lippincott Illustrated Reviews: Pharmacology, p. 294–295 | Goldman-Cecil Medicine, p. 755 | National Kidney Foundation Primer on Kidney Diseases, p. 690 | 2024 ESC Guidelines for Hypertension [PMID: 39210715]
This is a shared conversation. Sign in to Orris to start your own chat.