Please make notes on subcutaneous icd
Reading File
Finding Sources
Finding Sources
Searching PubMed
"subcutaneous ICD" AND implantable cardioverter defibrillator
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Loading Image
Reading File
I now have comprehensive information to compile detailed notes. Let me put these together:
Subcutaneous ICD (S-ICD) - Clinical Notes
Sources: Braunwald's Heart Disease 12e, Miller's Anesthesia 10e
What is an S-ICD?
The subcutaneous ICD is a fully extrathoracic defibrillation system - neither the pulse generator nor the lead enters the vasculature or heart. It was initially approved in 2012 for defibrillation therapy in patients at risk for malignant ventricular arrhythmias. The current commercially available device is manufactured by Boston Scientific Inc.
Device Anatomy
The system consists of two components:
- Pulse generator - implanted between the anterior and midaxillary lines at the level of the 6th intercostal space on the left chest
- Single subcutaneous lead - tunneled medially from the pulse generator pocket to the xiphoid process, then superiorly along the left parasternal border
The lead carries:
- A distal sensing electrode
- A shock coil
- A proximal sensing electrode
Chest X-ray appearance of an implanted S-ICD (PA and lateral views):
What the S-ICD CAN and CANNOT Do
| Feature | S-ICD |
|---|---|
| Detect and shock VF/VT | YES |
| Post-shock backup pacing (50 ppm x 30 sec) | YES |
| Long-term bradycardia pacing | NO |
| Antitachycardia pacing (ATP) | NO |
| Cardiac resynchronization therapy (CRT) | NO |
Future models are expected to communicate wirelessly with leadless capsule pacemakers (Boston Scientific's Empower LP is in trials). This "modular cardiac rhythm management" would allow the S-ICD to trigger ATP through the leadless pacemaker.
Pre-implant ECG Screening
All candidates undergo pre-implant screening using surface ECG electrodes to assess risk of:
- T-wave oversensing
- R-wave double-counting
About 7-10% of candidates fail screening and are not suitable for S-ICD.
Advantages over Transvenous ICD
- Eliminates vascular access complications (pneumothorax, cardiac perforation, hemothorax)
- No intravascular/lead infection risk; no risk of lead-associated endocarditis
- Implantation is possible without fluoroscopy
- Lead extraction is simpler and safer (entirely subcutaneous)
- Lead failure may be less common
- Well-suited for MRI: no transvenous lead complications during scanning
Disadvantages vs Transvenous ICD
- Higher rate of inappropriate shocks (5-10% vs <2% in first year for transvenous ICDs), though newer sensing algorithms have reduced this
- Cannot deliver ATP, bradycardia pacing, or CRT
- Requires pre-implant ECG screening (7-10% fail)
- Higher defibrillation thresholds (DFTs) - defibrillation testing at implant is recommended (unlike transvenous, where testing can often be omitted)
- Larger pulse generator
- Shorter battery longevity (relative)
- Slower charge time vs modern transvenous devices
Patient Selection
Preferred Candidates for S-ICD
- Limited vascular access (e.g., dialysis patients)
- History or high risk of intravascular infection (e.g., prosthetic heart valves, prior CIED infection)
- Intracardiac shunt (where transvenous leads carry risk of paradoxical embolism)
- Young patients - easier lead extraction long-term, potentially greater lead longevity
- Brugada syndrome - lead-related complications are a real concern in this group
NOT candidates for S-ICD (need transvenous instead)
- Need for bradycardia pacing
- Need for ATP to manage VT
- Need for CRT (resynchronization)
- Fail pre-implant ECG screening
Complications
| Complication | Notes |
|---|---|
| Vascular access complications (pneumothorax, cardiac perforation) | NOT applicable - extrathoracic |
| Pocket infection | ~1.1% in large series; trend toward lower total infections than transvenous (Praetorian trial) |
| Systemic/intravascular infection | Not reported in S-ICD |
| Inappropriate shocks | Reduced with new sensing algorithms but still higher than transvenous |
Sensing and EGMs
The S-ICD records subcutaneous EGMs from one of three sensing vectors:
- Primary vector
- Secondary vector (prone to myopotential artifact - overlies pectoralis muscles)
- Alternate vector (smallest amplitude - often overlies atrial tissue and sternum)
Perioperative / Magnet Behavior
The S-ICD responds to a magnet similarly to a standard Boston Scientific ICD:
- Magnet application over the pulse generator suspends arrhythmia detection and shock therapy
- A beeping sound confirms correct magnet positioning (stops after 60 seconds, but therapy remains suspended while magnet is in place)
- Removing the magnet reverts the device to its prior programmed state
- In the perioperative setting, preferred approach is to reprogram the device (turn off antitachycardic function) and place defibrillator pads
Defibrillation Testing at Implant
- Recommended for all S-ICD implants because DFTs are higher with subcutaneous shock vectors
- This differs from transvenous ICDs (left pectoral), where DFT testing can reasonably be omitted when lead position, sensing, and impedance are confirmed by fluoroscopy
Key Clinical Trials
- Praetorian trial - compared S-ICD vs transvenous ICD; showed a trend toward lower total infections with S-ICD
- A 2026 systematic review (PMID: 42171458 - Zweibel et al., J Med Econ) reviewed acute and long-term outcomes in patients with non-transvenous ICDs
Braunwald's Heart Disease 12e, Chapter 69 | Miller's Anesthesia 10e, Chapter on Emerging Technologies
Please provide images on subcutaneous icd and convert above into notes
Reading File
Finding Sources
Finding Sources
Searching the Web
subcutaneous ICD S-ICD images diagram anatomy lead placement screening
Loading Image
Loading Image
Loading Image
Loading Image
Running Command
mkdir -p /home/daytona/workspace/sicd-notes && cd /home/daytona/workspace/sicd-n…
Writing File
~/sicd-notes/build.js
const {
Document, Packer, Paragraph, TextRun, Table, TableRow, TableCell,
ImageRun, HeadingLevel, AlignmentType, BorderStyle, WidthType,
ShadingType, VerticalAlign, PageNumber, Header, Footer,
UnderlineType, TableOfContents
} = require('docx');
const fs = require('fs');
const path = require('path');
const DIR = '/home/daytona/workspace/sicd-notes/';
// Load images
const imgComparison = fs.readFileSync(path.join(DIR, 'img_braunwald_comparison.png'));
const imgCXR = fs.readFileSync(path.join(DIR, 'img_cxr.png'));
const imgAnatomy = fs.readFileSync(path.join(DIR, 'img_anatomy_comparison.jpg'));
const imgVectors = fs.readFileSync(path.join(DIR, 'img_screening_vectors.png'));
// ─── Helpers ──────────────────────────────────────────────────────────────────
function h1(text) {
return new Paragraph({
text,
heading: HeadingLevel.HEADING_1,
spacing: { before: 320, after: 120 },
border: { bottom: { style: BorderStyle.SINGLE, size: 6, color: '2E4057', space: 4 } },
});
}
function h2(text) {
return new Paragraph({
text,
heading: HeadingLevel.HEADING_2,
spacing: { before: 240, after: 80 },
});
}
function h3(text) {
return new Paragraph({
text,
heading: HeadingLevel.HEADING_3,
spacing: { before: 160, after: 60 },
});
}
function para(runs) {
if (typeof runs === 'string') runs = [new TextRun({ text: runs, size: 22 })];
return new Paragraph({ children: runs, spacing: { after: 100 } });
}
function bullet(text, bold_prefix) {
const children = [];
if (bold_prefix) {
children.push(new TextRun({ text: bold_prefix, bold: true, size: 22 }));
children.push(new TextRun({ text: ' ' + text, size: 22 }));
} else {
children.push(new TextRun({ text, size: 22 }));
}
return new Paragraph({
children,
bullet: { level: 0 },
spacing: { after: 60 },
});
}
function subbullet(text) {
return new Paragraph({
children: [new TextRun({ text, size: 22 })],
bullet: { level: 1 },
spacing: { after: 50 },
});
}
function boldText(t) { return new TextRun({ text: t, bold: true, size: 22 }); }
function normalText(t) { return new TextRun({ text: t, size: 22 }); }
function redText(t) { return new TextRun({ text: t, bold: true, color: 'C0392B', size: 22 }); }
function greenText(t) { return new TextRun({ text: t, bold: true, color: '27AE60', size: 22 }); }
function imageBlock(data, ext, w, h, caption) {
const type = ext === 'jpg' ? 'jpg' : 'png';
const items = [
new Paragraph({
children: [new ImageRun({ data, transformation: { width: w, height: h }, type })],
alignment: AlignmentType.CENTER,
spacing: { before: 120, after: 60 },
}),
];
if (caption) {
items.push(new Paragraph({
children: [new TextRun({ text: caption, italics: true, size: 18, color: '555555' })],
alignment: AlignmentType.CENTER,
spacing: { after: 160 },
}));
}
return items;
}
function spacer() {
return new Paragraph({ text: '', spacing: { after: 80 } });
}
// ─── Table helpers ────────────────────────────────────────────────────────────
function makeTable(headers, rows, colWidths) {
const headerRow = new TableRow({
children: headers.map((h, i) => new TableCell({
children: [new Paragraph({
children: [new TextRun({ text: h, bold: true, size: 20, color: 'FFFFFF' })],
alignment: AlignmentType.CENTER,
})],
shading: { type: ShadingType.SOLID, fill: '2E4057' },
width: { size: colWidths[i], type: WidthType.DXA },
verticalAlign: VerticalAlign.CENTER,
})),
tableHeader: true,
});
const dataRows = rows.map((row, ri) => new TableRow({
children: row.map((cell, ci) => new TableCell({
children: [new Paragraph({
children: [new TextRun({ text: cell, size: 20 })],
alignment: AlignmentType.LEFT,
})],
shading: { type: ShadingType.SOLID, fill: ri % 2 === 0 ? 'EBF5FB' : 'FFFFFF' },
width: { size: colWidths[ci], type: WidthType.DXA },
})),
}));
return new Table({
rows: [headerRow, ...dataRows],
width: { size: 100, type: WidthType.PERCENTAGE },
margins: { top: 80, bottom: 80, left: 80, right: 80 },
});
}
function twoColumnCompareTable(headers, leftRows, rightRows) {
const hRow = new TableRow({
children: headers.map((h, i) => new TableCell({
children: [new Paragraph({
children: [new TextRun({ text: h, bold: true, size: 20, color: 'FFFFFF' })],
alignment: AlignmentType.CENTER,
})],
shading: { type: ShadingType.SOLID, fill: i === 0 ? '2E4057' : '1A5276' },
width: { size: 4500, type: WidthType.DXA },
})),
tableHeader: true,
});
const maxLen = Math.max(leftRows.length, rightRows.length);
const dataRows = [];
for (let i = 0; i < maxLen; i++) {
dataRows.push(new TableRow({
children: [
new TableCell({
children: [new Paragraph({ children: [new TextRun({ text: leftRows[i] || '', size: 20 })], })],
shading: { type: ShadingType.SOLID, fill: i % 2 === 0 ? 'D6EAF8' : 'EBF5FB' },
width: { size: 4500, type: WidthType.DXA },
}),
new TableCell({
children: [new Paragraph({ children: [new TextRun({ text: rightRows[i] || '', size: 20 })], })],
shading: { type: ShadingType.SOLID, fill: i % 2 === 0 ? 'FDFEFE' : 'F8F9F9' },
width: { size: 4500, type: WidthType.DXA },
}),
],
}));
}
return new Table({
rows: [hRow, ...dataRows],
width: { size: 100, type: WidthType.PERCENTAGE },
margins: { top: 80, bottom: 80, left: 80, right: 80 },
});
}
// ─── Banner / Title ────────────────────────────────────────────────────────────
const titleBlock = [
new Paragraph({
children: [new TextRun({ text: 'SUBCUTANEOUS ICD (S-ICD)', bold: true, size: 52, color: 'FFFFFF' })],
alignment: AlignmentType.CENTER,
spacing: { before: 200, after: 80 },
shading: { type: ShadingType.SOLID, fill: '2E4057' },
}),
new Paragraph({
children: [new TextRun({ text: 'Clinical Notes | Cardiology', size: 26, color: 'FFFFFF', italics: true })],
alignment: AlignmentType.CENTER,
spacing: { before: 0, after: 200 },
shading: { type: ShadingType.SOLID, fill: '2E4057' },
}),
new Paragraph({
children: [new TextRun({ text: 'Sources: Braunwald\'s Heart Disease 12e | Miller\'s Anesthesia 10e | Fuster & Hurst\'s The Heart 15e', size: 18, italics: true, color: '666666' })],
alignment: AlignmentType.CENTER,
spacing: { after: 300 },
}),
];
// ─── Section 1: Overview ──────────────────────────────────────────────────────
const sec1 = [
h1('1. OVERVIEW'),
para([
normalText('The '),
boldText('subcutaneous ICD (S-ICD)'),
normalText(' is a fully extrathoracic defibrillation system in which '),
boldText('neither the pulse generator nor the lead enters the vasculature or heart.'),
normalText(' FDA-approved in '),
boldText('2012'),
normalText(', it is used for termination of malignant ventricular arrhythmias (VF/VT) in patients who do not require pacing or resynchronization therapy. Currently manufactured by '),
boldText('Boston Scientific Inc.'),
normalText(' (EMBLEM S-ICD).'),
]),
];
// ─── Section 2: Device Anatomy ────────────────────────────────────────────────
const sec2 = [
h1('2. DEVICE ANATOMY & IMPLANTATION'),
h2('2.1 Components'),
bullet('Pulse generator - implanted between the anterior and midaxillary lines at the level of the 6th intercostal space (left lateral chest wall)'),
bullet('Single subcutaneous lead - tunneled medially from the pulse generator to the xiphoid process, then superiorly along the left parasternal border'),
spacer(),
h2('2.2 Lead Electrodes'),
bullet('Distal sensing electrode (superior end of lead near manubrium)'),
bullet('Shock coil (main defibrillation element)'),
bullet('Proximal sensing electrode (near xiphoid)'),
spacer(),
h2('2.3 Sensing Vectors (3 available)'),
bullet('Primary vector - distal electrode to pulse generator can'),
bullet('Secondary vector - prone to myopotential artifact (overlies pectoralis muscles)'),
bullet('Alternate vector - smallest amplitude; often overlies atrial tissue and sternum'),
spacer(),
...imageBlock(imgAnatomy, 'jpg', 480, 220, 'Figure 1: S-ICD vs Transvenous ICD - anatomy and position (Nature Reviews Cardiology)'),
...imageBlock(imgVectors, 'png', 400, 200, 'Figure 2: S-ICD ECG screening vectors - electrode positions and vector directions'),
h2('2.4 Implantation Notes'),
bullet('Can be implanted WITHOUT fluoroscopy (advantage over transvenous systems)'),
bullet('Only implantable in the left chest (current generation)'),
bullet('Defibrillation testing at implant is RECOMMENDED (DFTs higher than transvenous)'),
spacer(),
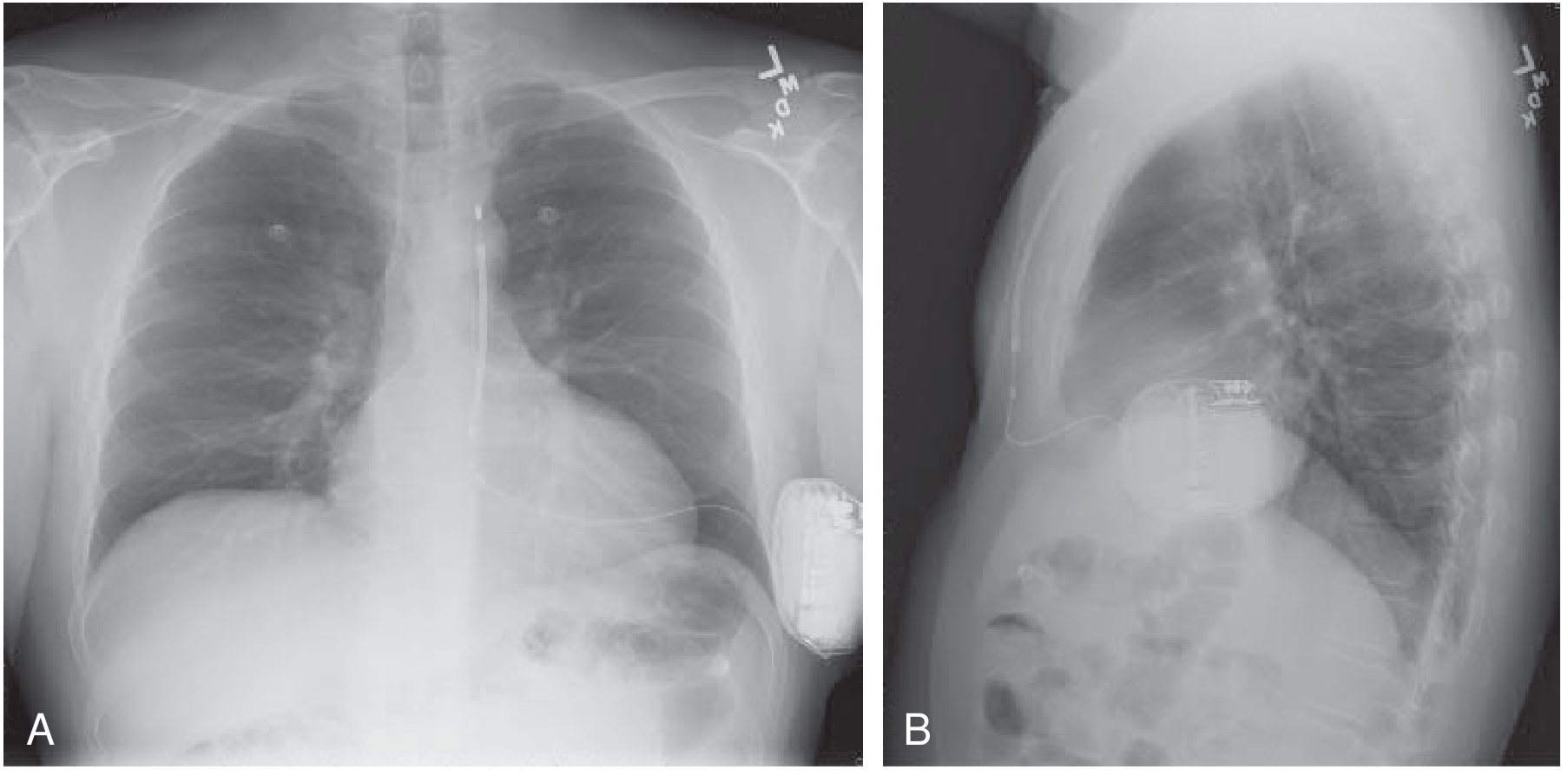
...imageBlock(imgCXR, 'png', 500, 220, 'Figure 3: Chest X-ray (PA and lateral) of implanted S-ICD system (Braunwald\'s Heart Disease 12e, Fig 69.5)'),
];
// ─── Section 3: Capabilities ─────────────────────────────────────────────────
const sec3 = [
h1('3. WHAT THE S-ICD CAN AND CANNOT DO'),
makeTable(
['Feature', 'S-ICD', 'Transvenous ICD'],
[
['Detect & shock VF/VT', '✔ YES', '✔ YES'],
['Post-shock backup pacing (50 ppm × 30 sec)', '✔ YES (temporary only)', '✔ YES'],
['Long-term bradycardia pacing', '✘ NO', '✔ YES'],
['Antitachycardia pacing (ATP)', '✘ NO', '✔ YES'],
['Cardiac resynchronization therapy (CRT)', '✘ NO', '✔ YES'],
['MRI compatibility', '✔ Easier (no intracardiac lead)', 'Conditional'],
['Fluoroscopy at implant required', '✘ Not required', '✔ Usually required'],
['Defibrillation testing at implant', '✔ Recommended (higher DFTs)', 'Can often be omitted'],
],
[3200, 2200, 2200]
),
spacer(),
para([
boldText('Future:'),
normalText(' Boston Scientific\'s '),
boldText('Empower LP leadless pacemaker'),
normalText(' (in trials) will communicate wirelessly with the S-ICD - enabling ATP delivery through the leadless device ("modular cardiac rhythm management").'),
]),
];
// ─── Section 4: Pre-implant ECG Screening ────────────────────────────────────
const sec4 = [
h1('4. PRE-IMPLANT ECG SCREENING'),
para([
normalText('All candidates undergo surface ECG screening before implantation to assess risk of:'),
]),
bullet('T-wave oversensing'),
bullet('R-wave double-counting'),
spacer(),
para([
boldText('~7-10% of candidates fail screening'),
normalText(' and are NOT suitable for S-ICD - they must receive a transvenous ICD instead.'),
]),
para([
normalText('Screening uses electrodes placed at standardized positions to simulate the 3 sensing vectors. A minimum R-wave amplitude and acceptable T:R ratio must be met in at least one vector.'),
]),
];
// ─── Section 5: Patient Selection ────────────────────────────────────────────
const sec5 = [
h1('5. PATIENT SELECTION'),
h2('5.1 Preferred Candidates for S-ICD'),
bullet('Limited vascular access', ''),
subbullet('e.g., dialysis patients with exhausted venous access'),
bullet('History or high risk of intravascular infection', ''),
subbullet('e.g., prosthetic heart valves, prior CIED infection, IV drug users'),
bullet('Intracardiac shunt (reduces paradoxical embolism risk from transvenous leads)'),
bullet('Young patients', ''),
subbullet('Easier future lead extraction; potentially greater lead longevity'),
bullet('Brugada syndrome - lead-related complications are a concern; S-ICD preferred'),
spacer(),
h2('5.2 NOT Suitable - Use Transvenous ICD Instead'),
bullet('Need for long-term bradycardia pacing'),
bullet('Need for ATP (frequent VT amenable to antitachycardia pacing)'),
bullet('Need for cardiac resynchronization therapy (CRT)'),
bullet('Fail pre-implant ECG screening (~7-10% of candidates)'),
spacer(),
twoColumnCompareTable(
['S-ICD ADVANTAGES', 'TRANSVENOUS ICD ADVANTAGES'],
[
'No vascular/intravascular lead complications',
'No pneumothorax, cardiac perforation risk',
'No intravascular system infection',
'Implant possible without fluoroscopy',
'Lead failure may be less likely',
'Simpler and safer lead extraction',
],
[
'Bradycardia, ATP, CRT pacing',
'No pre-implant ECG screening needed',
'Fewer inappropriate shocks (<2%/yr)',
'Greater battery longevity',
'Shorter charge time; faster shock delivery',
'Smaller pulse generator; long-term data',
]
),
spacer(),
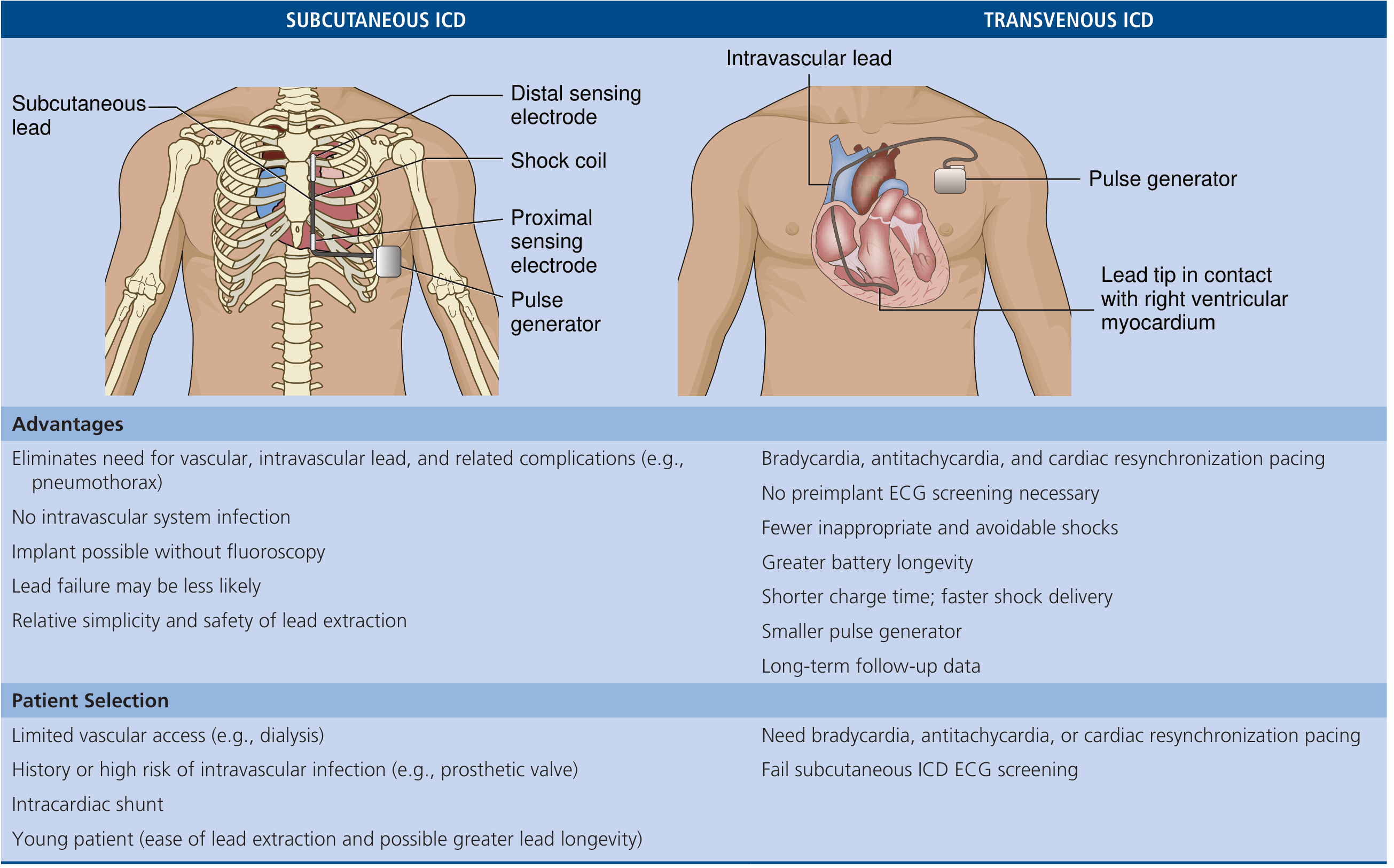
...imageBlock(imgComparison, 'png', 560, 380, 'Figure 4: S-ICD vs Transvenous ICD - full comparison table with anatomy (Braunwald\'s Heart Disease 12e, eTable 69.4)'),
];
// ─── Section 6: Sensing & Detection ──────────────────────────────────────────
const sec6 = [
h1('6. SENSING, DETECTION & INAPPROPRIATE SHOCKS'),
para([
normalText('The S-ICD senses subcutaneous EGMs. Because it lacks intracardiac electrograms, it is '),
boldText('more susceptible to oversensing'),
normalText(' than transvenous ICDs.'),
]),
h2('6.1 Inappropriate Shock Rates'),
bullet('S-ICD: 5-10% in the first year'),
bullet('Modern transvenous ICD: <2% in the first year'),
bullet('New SMART Pass sensing algorithm (BeatSense) has significantly reduced inappropriate shocks'),
spacer(),
h2('6.2 Causes of Inappropriate Shocks'),
bullet('T-wave oversensing (most common) - identified on pre-implant screening'),
bullet('Myopotential oversensing (especially secondary vector overlying pectoralis)'),
bullet('Double-counting of R or T waves'),
bullet('External electromagnetic interference'),
spacer(),
h2('6.3 Sensing Vectors'),
para([normalText('Three bipolar sensing vectors available (device auto-selects optimal or manually programmed):')]),
bullet('Primary - distal electrode to can'),
bullet('Secondary - prone to myopotential artefact'),
bullet('Alternate - smallest amplitude; overlies atrial tissue and sternum'),
];
// ─── Section 7: Defibrillation ────────────────────────────────────────────────
const sec7 = [
h1('7. DEFIBRILLATION & SHOCK THERAPY'),
bullet('Shock energy: up to 80 J (higher than most transvenous devices ~40 J)'),
bullet('DFTs are higher for S-ICD than transvenous ICDs due to extrathoracic vector'),
bullet('Defibrillation testing at implant is RECOMMENDED for all S-ICD patients'),
bullet('Post-shock backup pacing: 50 ppm for up to 30 seconds if patient becomes bradycardic after shock'),
bullet('Device delivers up to 5 shocks per detected episode'),
para([
boldText('Note:'),
normalText(' Using maximum energy for the first shock is reasonable - minimizes episode duration and need for multiple shocks.'),
]),
];
// ─── Section 8: Complications ────────────────────────────────────────────────
const sec8 = [
h1('8. COMPLICATIONS'),
makeTable(
['Complication', 'S-ICD', 'Notes'],
[
['Pneumothorax / cardiac perforation', 'NOT applicable', 'Fully extrathoracic - no vascular access'],
['Pocket infection', '~1.1% of implants', 'Praetorian trial: trend toward fewer than transvenous'],
['Systemic / intravascular infection', 'Not reported', 'Major advantage - no intravascular lead'],
['Inappropriate shocks', '5-10%/yr (reduced with new algorithms)', 'Still higher than transvenous ICDs'],
['Lead-related failure', 'Potentially less likely', 'Subcutaneous environment is less hostile'],
['Lead extraction complications', 'Simpler and safer', 'Entirely subcutaneous - no laser extraction'],
],
[2400, 2000, 2800]
),
spacer(),
h2('Key Trial - Praetorian (2020)'),
para([
normalText('Randomized trial of S-ICD vs transvenous ICD. S-ICD showed '),
boldText('non-inferiority'),
normalText(' for complications + inappropriate shocks composite endpoint. Trend toward lower total infections with S-ICD.'),
]),
];
// ─── Section 9: Perioperative / Magnet ───────────────────────────────────────
const sec9 = [
h1('9. PERIOPERATIVE MANAGEMENT & MAGNET BEHAVIOR'),
h2('9.1 Magnet Response (Boston Scientific behavior)'),
bullet('Magnet applied over pulse generator: SUSPENDS arrhythmia detection and shock therapy'),
bullet('A beeping tone confirms correct magnet positioning'),
subbullet('Beeping stops after 60 seconds - but therapy REMAINS suspended as long as magnet stays in place'),
subbullet('If no beep heard - reposition magnet until beep is elicited'),
bullet('Removing the magnet: device REVERTS to prior programmed state automatically'),
spacer(),
h2('9.2 Perioperative Strategy'),
bullet('Preferred: REPROGRAM device (turn off antitachycardic function) before surgery - do not rely on magnet alone'),
bullet('Place external defibrillator pads when device reprogrammed'),
bullet('Located at midaxillary line (6th ICS) - can interfere with surgical positioning; note location'),
bullet('Does NOT provide pacing - if pacing is needed intraoperatively, external pacing must be arranged'),
spacer(),
h2('9.3 EMI Considerations'),
bullet('Electrocautery / monopolar diathermy: risk of inappropriate sensing/shock - device should be reprogrammed'),
bullet('S-ICD is more susceptible to electromagnetic interference than transvenous ICDs'),
];
// ─── Section 10: Key Numbers ─────────────────────────────────────────────────
const sec10 = [
h1('10. KEY NUMBERS TO REMEMBER'),
makeTable(
['Parameter', 'Value'],
[
['FDA approval year', '2012'],
['Pre-implant screening failure rate', '7-10% of candidates'],
['Inappropriate shock rate (Year 1)', '5-10% (S-ICD) vs <2% (transvenous)'],
['Pocket infection rate', '~1.1%'],
['Post-shock backup pacing', '50 ppm × 30 seconds'],
['Pulse generator position', 'Left lateral chest, anterior-midaxillary line, 6th ICS'],
['Lead trajectory', 'Xiphoid → left parasternal border (subcutaneous)'],
['Maximum shock energy', 'Up to 80 J'],
],
[4000, 4000]
),
];
// ─── Section 11: Recent Evidence ─────────────────────────────────────────────
const sec11 = [
h1('11. RECENT EVIDENCE'),
bullet('Praetorian Trial (NEJM 2020): S-ICD non-inferior to transvenous ICD for combined endpoint of device-related complications + inappropriate shocks'),
bullet('Zweibel et al., J Med Econ (2026): Systematic review of acute and long-term outcomes in non-transvenous ICD patients (PMID: 42171458)'),
bullet('New sensing algorithms (SMART Pass / BeatSense) have substantially reduced inappropriate shocks from T-wave oversensing'),
bullet('Modular cardiac rhythm management (S-ICD + Empower LP leadless pacemaker) in clinical trials - will provide fully leadless ICD + ATP capability'),
];
// ─── Assemble document ────────────────────────────────────────────────────────
const doc = new Document({
styles: {
paragraphStyles: [
{
id: 'Heading1',
name: 'Heading 1',
basedOn: 'Normal',
next: 'Normal',
run: { size: 28, bold: true, color: '2E4057', font: 'Calibri' },
paragraph: { spacing: { before: 320, after: 120 } },
},
{
id: 'Heading2',
name: 'Heading 2',
basedOn: 'Normal',
next: 'Normal',
run: { size: 24, bold: true, color: '1A5276', font: 'Calibri' },
paragraph: { spacing: { before: 200, after: 80 } },
},
{
id: 'Heading3',
name: 'Heading 3',
basedOn: 'Normal',
next: 'Normal',
run: { size: 22, bold: true, color: '117A65', font: 'Calibri' },
paragraph: { spacing: { before: 160, after: 60 } },
},
],
default: {
document: {
run: { font: 'Calibri', size: 22 },
},
},
},
sections: [
{
properties: {
page: {
margin: { top: 720, bottom: 720, left: 900, right: 900 },
},
},
children: [
...titleBlock,
...sec1,
...sec2,
...sec3,
...sec4,
...sec5,
...sec6,
...sec7,
...sec8,
...sec9,
...sec10,
...sec11,
],
},
],
});
Packer.toBuffer(doc).then(buffer => {
fs.writeFileSync(path.join(DIR, 'Subcutaneous_ICD_Notes.docx'), buffer);
console.log('SUCCESS: Subcutaneous_ICD_Notes.docx created');
}).catch(err => {
console.error('ERROR:', err);
process.exit(1);
});
Running Command
cd /home/daytona/workspace/sicd-notes && node build.js 2>&1
Running Command
python3 /home/daytona/skills/docx/scripts/office/validate.py /home/daytona/works…
Running Command
cd /home/daytona/workspace/sicd-notes && python3 -c " import zipfile, os with zi…
Your Word document is ready:
Subcutaneous ICD Notes
Word Document · DOCX
Here is a preview of all the images included in the notes:
Figure 1 - S-ICD vs Transvenous ICD anatomy (Nature Reviews Cardiology):
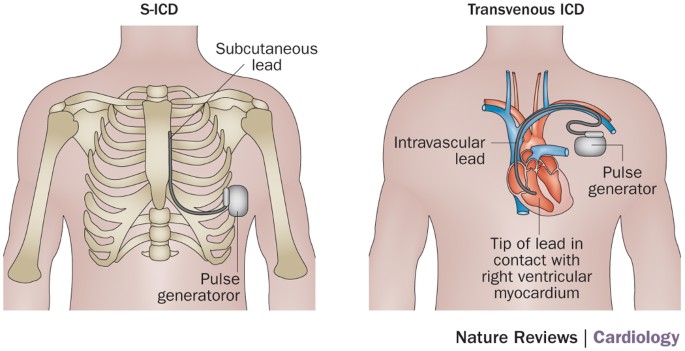
Figure 2 - ECG Screening Vectors (electrode positions):
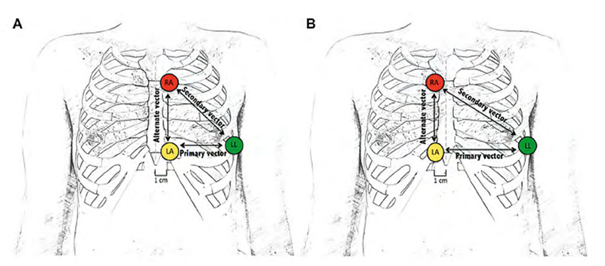
Figure 3 - S-ICD full comparison table with anatomy (Braunwald's 12e, eTable 69.4):
Figure 4 - Chest X-ray of implanted S-ICD (Braunwald's 12e, Fig 69.5):
The document contains 11 sections with color-coded headings, formatted tables, and all 4 images embedded:
| Section | Content |
|---|---|
| 1 | Overview & approval history |
| 2 | Device anatomy, components, implant technique |
| 3 | Capabilities table (S-ICD vs transvenous) |
| 4 | Pre-implant ECG screening |
| 5 | Patient selection (indications & contraindications) |
| 6 | Sensing vectors, inappropriate shocks |
| 7 | Defibrillation & shock therapy |
| 8 | Complications (with Praetorian trial) |
| 9 | Perioperative management & magnet behavior |
| 10 | Key numbers quick reference table |
| 11 | Recent evidence & trials |
This is a shared conversation. Sign in to Orris to start your own chat.