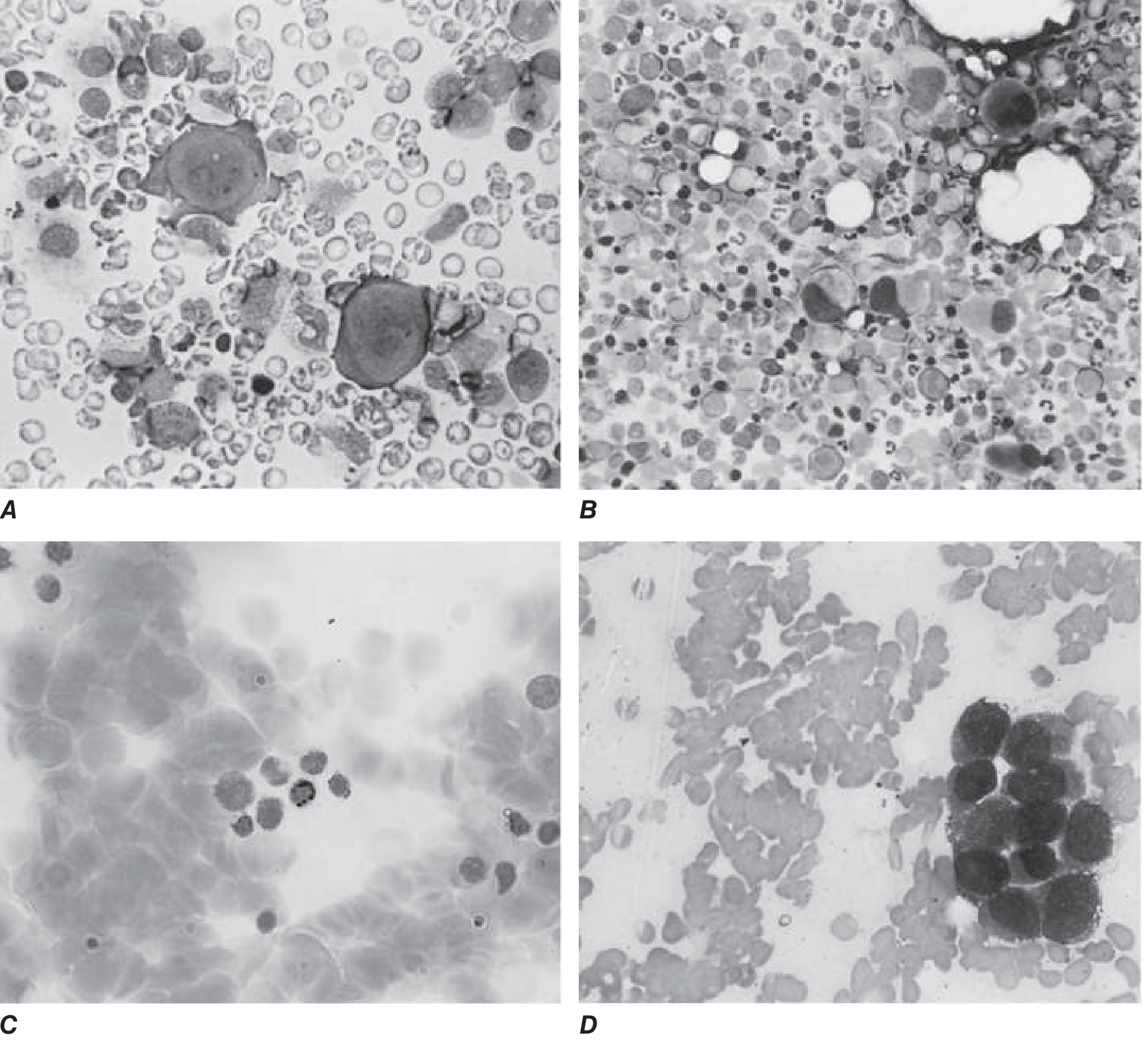
A 45-year-old patient presents to the haematologist with complaints of weakness and fatigue. Lab investigations reveal a decrease in the haemoglobin and reticulocyte count while WBC and platelet counts are normal. Bone marrow shows a selective decrease in the erythroid precursors. What is the likely diagnosis?
"pure red cell aplasia" diagnosis treatment
Diagnosis: Pure Red Cell Aplasia (PRCA)
Why This Diagnosis Fits
| Feature | This Patient | PRCA Hallmark |
|---|---|---|
| Hemoglobin | Low | Yes - normocytic anemia |
| Reticulocyte count | Low | Yes - reticulocytopenia (aregenerative) |
| WBC | Normal | Yes - myeloid line unaffected |
| Platelets | Normal | Yes - megakaryocytes unaffected |
| Bone marrow | Absent/reduced erythroid precursors | Defining feature |
- Harrison's Principles of Internal Medicine 22E, p. 857
- Robbins, Cotran & Kumar Pathologic Basis of Disease
Classification of PRCA
- Transient erythroblastopenia of childhood
- Transient aplastic crisis in hemolytic anemias (acute B19 parvovirus infection)
- Fetal red cell aplasia / nonimmune hydrops fetalis
- Diamond-Blackfan anemia - diagnosed at birth or in early childhood; due to mutations in ribosomal protein genes; often responds to glucocorticoids
- Primary immune-mediated (most common in adults)
- Associated with thymoma (classic association - resection leads to improvement in ~50% of cases)
- Large granular lymphocytic (LGL) leukemia or chronic lymphocytic leukemia (CLL)
- MDS with 5q- syndrome
- Connective tissue diseases (SLE, RA)
- Persistent parvovirus B19 infection (especially in immunosuppressed patients)
- Drug exposures
- Recombinant erythropoietin-induced (neutralizing antibodies to EPO)
Pathophysiology
Key Differentials to Rule Out
- Aplastic anemia - pancytopenia with a hypocellular marrow (all three lineages affected)
- Myelodysplastic syndrome (MDS) - dysplastic changes across lineages; may include cytopenias
- Iron deficiency anemia - microcytic, low reticulocytes, but no selective erythroid progenitor loss on marrow biopsy
- Hemolytic anemia - reticulocyte count would be HIGH, not low
Treatment Approach (Acquired PRCA)
- Treat/remove the underlying cause: thymectomy if thymoma is present, stop offending drugs
- Immunosuppression: corticosteroids first-line; cyclosporine, cyclophosphamide, or azathioprine for refractory cases
- IVIG: for parvovirus B19-associated PRCA in immunocompromised patients
- Plasmapheresis: for cases with anti-erythropoietin antibodies
- Rituximab or alemtuzumab: for LGL leukemia-associated PRCA
What investigations would help identify the underlying cause?
Investigations to Identify the Underlying Cause of PRCA
1. Bone Marrow Biopsy (Confirmatory - Already Done)
- Normal to hypocellular marrow
- Absent or nearly absent erythroid precursors (erythroblasts)
- Normal myeloid and megakaryocytic series
2. Imaging - To Detect Thymoma
| Investigation | Rationale |
|---|---|
| CT chest (investigation of choice) | Thymoma is the single most important association in adults; anterior mediastinal mass on CT |
| Chest X-ray | May show anterior mediastinal widening but CT is superior |
Thymoma is present in a minority of PRCA cases, but resection leads to hematological improvement in ~25-30% of thymoma-associated cases.
3. Peripheral Blood - For LGL Leukemia
| Investigation | Rationale |
|---|---|
| Peripheral blood film | Large granular lymphocytes (LGL) may be increased; LGL leukemia is a common cause of PRCA in adults |
| Flow cytometry (peripheral blood) | Quantify LGL concentration; characterize T-cell or NK-cell clones (CD3+CD8+CD57+ profile is typical of T-LGL leukemia) |
| T-cell receptor (TCR) gene rearrangement | Confirms clonality of LGL population |
4. Virology - To Detect Parvovirus B19
| Investigation | Rationale |
|---|---|
| Parvovirus B19 PCR (DNA detection in blood) | Gold standard; antibody tests (IgG/IgM) are unreliable in immunosuppressed patients as they may be absent |
| Parvovirus IgG/IgM serology | Useful only in immunocompetent patients; IgM indicates acute infection |
5. Immunological Studies - Autoimmune Causes
| Investigation | Rationale |
|---|---|
| ANA (Antinuclear antibodies) | Screen for SLE |
| Anti-dsDNA, complement (C3/C4) | Confirm SLE if ANA positive |
| Rheumatoid factor (RF) + Anti-CCP | Screen for rheumatoid arthritis |
| Serum immunoglobulins (IgG, IgA, IgM) | Hypogammaglobulinaemia is associated with PRCA; thymoma can cause Good syndrome (thymoma + hypogammaglobulinaemia) |
| Anti-erythropoietin antibodies | If patient has received recombinant EPO therapy - EPO-induced PRCA via neutralising antibodies; plasmapheresis is the treatment |
6. Biochemistry - Organ Function & Secondary Causes
| Investigation | Rationale |
|---|---|
| Liver function tests (LFTs) | Hepatitis-associated aplasia; liver disease affects erythropoiesis |
| Renal function tests (urea, creatinine) | Renal failure reduces EPO production (though usually pan-lineage effect) |
| Thyroid function tests (TFTs) | Hypothyroidism can impair red cell production |
| HIV serology | HIV-associated PRCA, especially when chronic parvovirus co-infection |
7. Haematological Studies - Rule Out Malignancy
| Investigation | Rationale |
|---|---|
| Lymph node biopsy / CT abdomen-pelvis | If lymphoma is suspected based on clinical or flow cytometry findings |
| STAT3 / STAT5b mutation analysis | Common mutations in T-LGL leukemia |
| Cytogenetics / FISH on bone marrow | Detect 5q deletion (5q- syndrome - MDS presenting as red cell aplasia); other MDS-associated abnormalities |
8. Drug and Toxin History
- Recombinant human erythropoietin (rHuEPO) - via anti-EPO antibodies
- Mycophenolate mofetil
- Isoniazid
- Azathioprine
- Phenytoin
- Chloramphenicol
- AZT (zidovudine)
Summary Algorithm
PRCA Confirmed on Bone Marrow
|
├── CT Chest → Thymoma?
├── Peripheral blood film + Flow cytometry → LGL Leukemia?
├── Parvovirus B19 PCR → Viral cause?
├── ANA/Anti-dsDNA/RF → Autoimmune disease?
├── Serum Ig levels → Hypogammaglobulinaemia / Good syndrome?
├── Anti-EPO antibodies → Drug-induced (rHuEPO)?
├── Medication review → Drug-induced?
├── HIV serology → HIV-related?
└── BFU-E colony assay → Predicts response to immunosuppression
- Goldman-Cecil Medicine, p. 1744 - Diagnosis section
- Harrison's Principles of Internal Medicine 22E, p. 857-858
Best books for pharmacology
best pharmacology textbooks medical school MBBS 2024 2025
Best Pharmacology Books for Medical School (MBBS/MD)
Tier 1 - Core Textbooks (Pick One as Your Main Book)
- Best for: MBBS exams, USMLE Step 1 foundation, NEET PG prep
- Verdict: Start here if you can only pick one book
- Best for: Students who want deeper conceptual understanding and a strong international standard text
- Verdict: Best Western medical school standard text; pairs well with clinical years
- Best for: Advanced study, clinical pharmacology, postgraduate reference
- Verdict: Too detailed for early MBBS years; excellent in later years and beyond
Tier 2 - Concise / Revision Books
- Best for: Visual learners, quick concept grasp, parallel reading alongside a main text
- Verdict: Excellent supplementary or even standalone book for many students
- Best for: Board exam revision, self-testing
- Verdict: Best review/Q-bank style book for exams
- Best for: Last-minute exam prep, NEET PG, USMLE Step 1 rapid review
- Verdict: Excellent revision companion, not a primary learning resource
Tier 3 - Specialized / Visual References
| Book | Best For |
|---|---|
| BRS Pharmacology (Board Review Series) | Concise USMLE-focused review |
| First Aid for USMLE Step 1 (pharmacology sections) | Integrating pharm into a broader Step 1 prep strategy |
| Clinical Pharmacology by Laurence & Bennett | Clinical application, final year and beyond |
| Basic & Clinical Pharmacology - Katzung (16th Ed.) | International standard; comprehensive but approachable |
Recommended Reading Strategy by Year
| Year | Recommended Approach |
|---|---|
| Pre-clinical / 2nd year MBBS | KD Tripathi (primary) + Lippincott (visual aid) |
| Clinical years (3rd-5th) | Rang & Dale or Katzung for depth; clinical pharmacology focus |
| Exam prep / finals | Sparsh Gupta or BRS for high-yield revision |
| Postgraduate / residency | Goodman & Gilman as reference |
Quick Verdict
- Single best book for MBBS: KD Tripathi
- Best for conceptual depth: Rang & Dale
- Best visual/diagram book: Lippincott Illustrated Reviews
- Best for board exams: Katzung & Trevor's or BRS Pharmacology
- Best comprehensive reference: Goodman & Gilman
FMGE orentiated
best pharmacology books FMGE screening test 2024 2025 preparation
best pharmacology books FMGE
Best Pharmacology Books for FMGE Preparation
Understanding What FMGE Demands in Pharmacology
- Mechanism-of-action based
- Drug of choice (DOC) for specific conditions
- Side effect profiles and contraindications
- High-yield drug interactions
- Recent drug additions to NEET PG / NBE pattern
Tier 1 - Primary FMGE Pharmacology Book (Pick One)
- Best for: Main revision, NBE-pattern MCQ prep
- Verdict: Top pick for FMGE pharmacology
- Best for: Conceptual clarity on mechanisms, building your pharmacology base
- Verdict: Essential reference; read during MBBS, revise key chapters for FMGE
- Best for: Final 4-6 weeks of FMGE prep, rapid revision
- Verdict: Best revision companion alongside Ranjan Patel or KD Tripathi
Tier 2 - Supplementary / Question Practice
| Book | Use |
|---|---|
| FMGE Solutions by Dr. Deepak Marwah | Subject-wise previous FMGE questions with explanations; excellent for pattern recognition |
| Across by Arvind Arora | Popular MCQ bank for FMGE/PGMEE across all subjects including pharmacology |
| Previous Year FMGE Question Papers (NBE) | Non-negotiable - practice at least 5-7 years of papers |
High-Yield Pharmacology Topics for FMGE
| Topic | Why It's High-Yield |
|---|---|
| Autonomic pharmacology (adrenergic/cholinergic) | Mechanism MCQs appear every exam |
| Antihypertensives | DOC questions in various clinical scenarios |
| Antibiotics (mechanism + resistance) | Very frequent, especially beta-lactams, fluoroquinolones |
| Antiepileptics | Drug of choice in pregnancy, neonates, status epilepticus |
| Antidepressants / antipsychotics | Side effect profiles heavily tested |
| Anticoagulants (heparin, warfarin, NOACs) | Reversal agents, monitoring tests |
| Cancer chemotherapy | Classification, cell-cycle specificity, side effects |
| Corticosteroids | Mechanism, uses, complications |
| NSAIDs / analgesics | COX selectivity, renal effects, drug interactions |
| ORS / IV fluids / electrolytes | Clinically applied pharmacology |
Recommended FMGE Pharmacology Strategy
- Foundation (if time allows): Read KD Tripathi for major drug classes during your MBBS years abroad
- FMGE Prep - Main revision: Ranjan Kumar Patel cover-to-cover (2-3 passes)
- Rapid revision (last 4-6 weeks): Sparsh Gupta for mnemonics + tables
- Practice: Deepak Marwah FMGE Solutions + previous year papers
- Mock tests: Simulate exam conditions - aim for speed and accuracy since there's no negative marking (attempt all 300 questions)
Quick Summary
| Priority | Book |
|---|---|
| Must-have #1 | Conceptual Review of Pharmacology - Ranjan Kumar Patel |
| Must-have #2 | Sparsh Gupta - Review of Pharmacology |
| Reference (if needed) | KD Tripathi - Essentials of Medical Pharmacology |
| MCQ practice | FMGE Solutions - Deepak Marwah + Previous year papers |
Pro tip: Since FMGE has no negative marking, completing all pharmacology topics even at a surface level and then doing question-based revision from previous papers is a more efficient strategy than deep-reading a single heavy textbook.
Q5. A 24-year-old trekker develops headache, nausea, dizziness, confusion and insomnia 12 hours after reaching an altitude of 3,800 m. What is the most probable cause for this condition-
Diagnosis: Acute Mountain Sickness (AMS)
Why This Is AMS - Matching the Case
| Patient Feature | AMS Criterion |
|---|---|
| Altitude of 3,800 m (~12,500 ft) | AMS occurs above 2,400-2,500 m (8,000 ft) |
| Symptoms onset at 12 hours | Classic: develops 6-10 hours after arrival, peaks at 24-48 hours |
| Headache | Cardinal/required symptom (Lake Louise Criteria) |
| Nausea | Gastrointestinal symptom - part of diagnostic criteria |
| Dizziness | Part of diagnostic criteria |
| Confusion | Suggests moderate-severe AMS (approaching HACE territory - watch closely) |
| Insomnia | Common at altitude due to periodic breathing |
Pathophysiology - Why Does AMS Occur?
Rapid ascent → ↓ PO₂ (hypobaric hypoxia)
↓
Hypoxic ventilatory response → Hyperventilation → Respiratory alkalosis
↓
Cerebral vasodilation (hypoxia-mediated)
↓
↑ Cerebral blood flow → ↑ Intracranial pressure
↓
Trigeminovascular activation → HEADACHE (cardinal symptom)
↓
CNS: nausea, dizziness, confusion, insomnia
Lake Louise Scoring Criteria for AMS (Diagnostic Standard)
- Gastrointestinal symptoms (anorexia, nausea, vomiting)
- Fatigue or weakness
- Dizziness / lightheadedness
AMS incidence: 22-67% of travelers to altitudes between 1,850-4,240 m. Rates up to 70% with rapid ascent (e.g., Mt. Kilimanjaro). - Murray & Nadel's Textbook of Respiratory Medicine
Spectrum of Altitude Illness (Important to Know)
| Condition | Key Features | This Patient? |
|---|---|---|
| AMS (Acute Mountain Sickness) | Headache + GI/dizziness/fatigue; normal neuro exam | YES - most likely |
| HACE (High Altitude Cerebral Edema) | AMS + ataxia + altered consciousness/coma | Confusion here is a WARNING sign - monitor closely |
| HAPE (High Altitude Pulmonary Edema) | Dyspnea at rest, cough, crackles, pink frothy sputum | Most lethal altitude illness; absent here |
The confusion in this patient is a red flag. Per Rosen's Emergency Medicine: "Any evidence of ataxia or altered mentation suggests HACE or other malignant etiology and mandates immediate descent." This patient should be monitored for progression to HACE.
Differential Diagnoses to Rule Out
- Dehydration (very common at altitude)
- Hypothermia
- Hyponatremia (from excessive water intake)
- Exhaustion / fatigue
- Carbon monoxide poisoning (if using gas stoves in poorly ventilated shelters - altitude makes CO poisoning worse)
- CNS infection (meningitis, encephalitis)
- Alcohol hangover
Management
- Rest at the same altitude
- Acetazolamide (Diamox) 250 mg BD - carbonic anhydrase inhibitor; stimulates ventilation, speeds acclimatization, reduces symptoms
- Ibuprofen / paracetamol for headache
- Ondansetron / prochlorperazine for nausea
- Supplemental oxygen if available
- Immediate descent (500-1,000 m is often enough)
- Dexamethasone 8 mg loading, then 4 mg every 6 hours - reduces cerebral edema
- Portable hyperbaric chamber (Gamow bag) if available - simulates descent
- Supplemental oxygen
- Gradual ascent - "climb high, sleep low"
- Above 3,000 m: limit ascent to 300-500 m/day
- Acetazolamide 125-250 mg BD starting 24 hours before ascent (prophylaxis)
- Avoid alcohol and sedatives (suppress ventilatory response)
- High-carbohydrate diet
Summary for FMGE/Exam
-
Diagnosis: Acute Mountain Sickness (AMS)
-
Cause: Hypobaric hypoxia from rapid ascent above 2,500 m
-
Cardinal symptom: Headache (mandatory for diagnosis)
-
Drug of choice - treatment: Acetazolamide ± Dexamethasone (severe)
-
Drug of choice - prophylaxis: Acetazolamide
-
Immediate severe action: Descent + Dexamethasone
-
Confusion at altitude = HACE until proven otherwise
-
Murray & Nadel's Textbook of Respiratory Medicine, p. 2431
-
Rosen's Emergency Medicine, Box 132.2