Bppv
Reading File
Finding Sources
Searching PubMed
"benign paroxysmal positional vertigo" AND treatment
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Here is a thorough clinical overview of Benign Paroxysmal Positional Vertigo (BPPV):
Benign Paroxysmal Positional Vertigo (BPPV)
Definition & Overview
BPPV is the most common cause of vertigo in patients presenting to otolaryngologists and neurologists. It is characterized by brief, recurrent episodes of vertigo and nystagmus triggered by specific changes in head position - classically rolling over in bed, looking up (top-shelf vertigo), bending forward and straightening up, or tilting the head back.
- Episodes typically last less than 1 minute (usually 15-40 seconds)
- No hearing loss or other neurological deficits
- More frequent than Meniere's disease
Pathophysiology
Two main theories explain BPPV:
-
Canalolithiasis (most common, accepted mechanism): Free-floating otolithic debris (otoconia/calcium carbonate crystals) detaches from the utricle and enters the endolymph of a semicircular canal. With head movement, this debris gravitates to the dependent part of the canal and induces abnormal fluid currents that deflect the cupula, triggering vertigo.
-
Cupulolithiasis: Otolithic crystals adhere directly to the cupula of the posterior semicircular canal, making it abnormally sensitive to gravity.
Canal involvement:
- Posterior semicircular canal: ~90% of cases
- Horizontal (lateral) canal: ~10% of cases
- Superior canal: rare
Clinical Features
| Feature | Details |
|---|---|
| Trigger | Rapid head position changes (rolling in bed, looking up) |
| Duration | Usually < 1 minute per episode |
| Latency | 2-10 second delay before onset after position change |
| Associated symptoms | Oscillopsia, nausea, fear during attacks |
| Hearing | Normal (no hearing loss) |
| Course | Episodic for days to months; may remit spontaneously |
Known precipitants (Baloh et al study of 240 cases):
- 17% onset after head trauma
- 15% after presumed viral neurolabyrinthitis
- Association with osteoporosis (Jeong et al)
Diagnosis: Dix-Hallpike Maneuver
The bedside Dix-Hallpike test is the gold standard for diagnosing posterior canal BPPV.
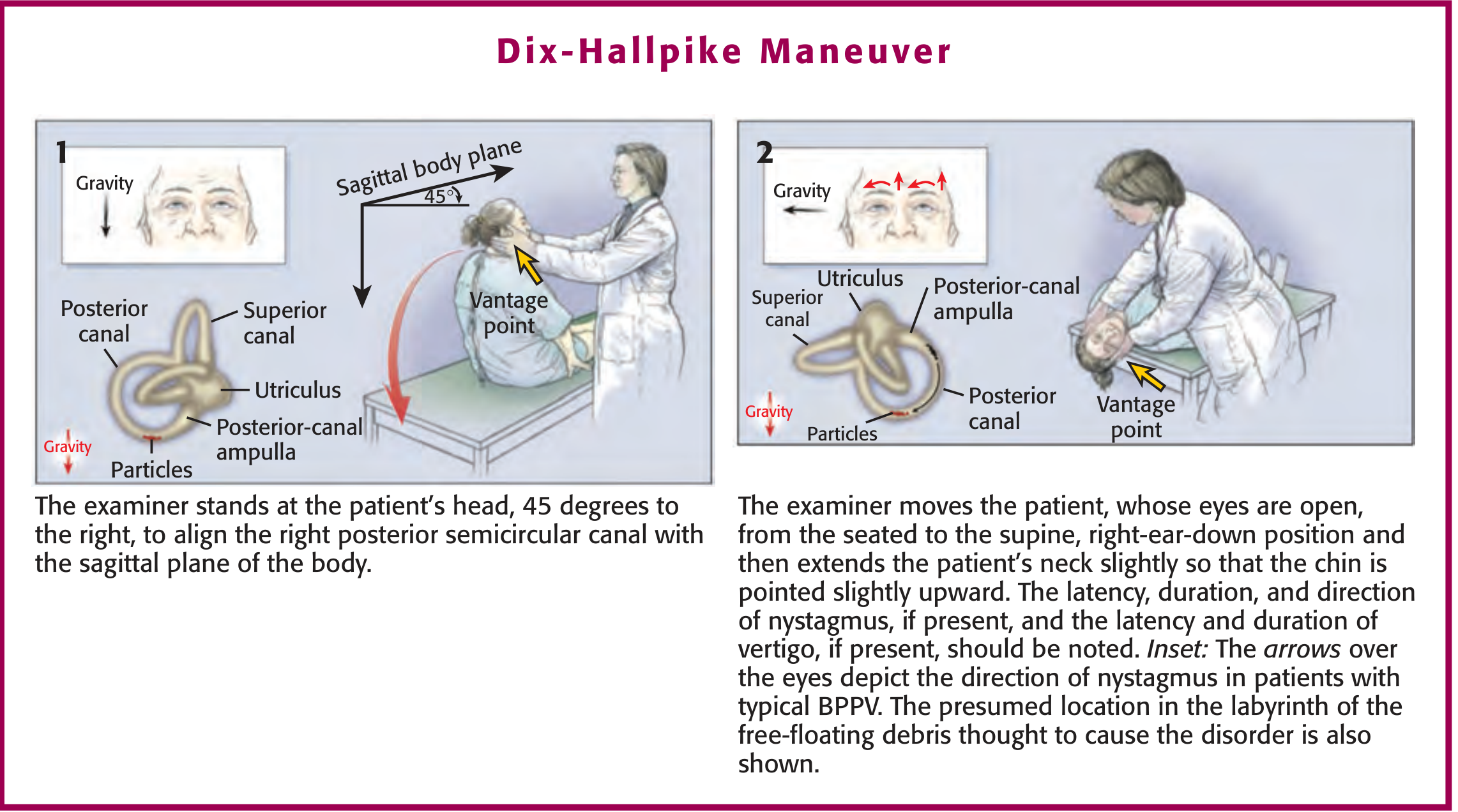
Technique:
- Patient sits upright; head turned 45 degrees to the side being tested
- Patient is rapidly laid back so the head hangs below the table (neck slightly extended)
- Hold the position for at least 30 seconds while observing for nystagmus
A positive response (posterior canal BPPV):
- Latency: 2-10 seconds before onset
- Mixed vertical-torsional nystagmus: fast-phase vertical toward forehead, torsional fast-phase toward the dependent (affected) ear
- Duration: < 30 seconds (usually < 15 s)
- Fatigues with repeated testing
- Nystagmus direction reverses when patient returns to sitting
Affected ear = the ear that is downward when vertigo is elicited (the dysfunctional ear).
Sensitivity: 75%; Specificity: 94%
Red Flags - Suspect Central Cause If:
- Nystagmus begins without latency (immediately on positioning)
- Nystagmus lasts > 1 minute
- Nystagmus does not fatigue
- Nystagmus is not suppressed by visual fixation
- Nystagmus is purely vertical or purely horizontal without rotatory component
- Associated neurological signs (dysarthria, diplopia, ataxia, headache)
CNS imaging is required when any of these alarm features are present.
Horizontal Canal BPPV
- Less common (~10%)
- Standard Dix-Hallpike may be negative
- Diagnosed by: laying patient supine then turning head side to side (supine roll test)
- Nystagmus: purely horizontal, may beat geotropically (toward ground - suggests canalolithiasis) or ageotropically (away from ground - suggests cupulolithiasis)
- Nystagmus tends to last longer than posterior canal BPPV
Treatment
1. Epley Canalith Repositioning Maneuver (first-line)
The Epley maneuver moves the free-floating debris out of the posterior semicircular canal and back into the vestibule, where it no longer causes symptoms.
Steps (for right ear):
- A. Start with Dix-Hallpike position (head 45° right, hanging back) - wait for vertigo to subside
- B. Rotate head 45-60° toward the opposite (left) ear
- C. Roll the entire body onto the left side, rotating head another 45° until face is nearly down
- D. Return to seated position with head turned left
Each step is held for ~20 seconds. A single treatment session is effective in approximately 80% of patients. A second sequence immediately after the first captures additional responders.
- Post-maneuver activity restrictions (avoiding head-down position for 24h) are no longer considered necessary based on recent studies
- Temporal bone vibration can be added in refractory cases to mobilize adherent crystals
Caution: An incompletely performed Epley maneuver risks converting posterior canal BPPV into the harder-to-treat lateral canal variant.
2. Semont Maneuver
For patients who fail or cannot tolerate the Epley maneuver:
- Patient sits with head turned 45° to one side
- Drops laterally to the side-lying position on the opposite ear
- Then swings briskly to the opposite side-lying position
3. Brandt-Daroff Exercises
A series of side-lying exercises performed repeatedly (sitting → side-lying → sitting). Used for home self-treatment and vestibular habituation.
4. Vestibular Rehabilitation
Exercises that trigger central adaptation; another viable option.
5. Vestibular Suppressants (use sparingly)
- Meclizine, benzodiazepines: May relieve acute symptoms but cause drowsiness, worsen imbalance, and delay CNS adaptation
- Use only for patients with frequent intolerable spells; avoid long-term use
6. Surgery
Reserved for refractory cases that fail all repositioning maneuvers. Rarely necessary.
Natural Course
Most patients recover regardless of therapy within 2-6 weeks, though it can take months. Episodes may come and go for years, particularly in the elderly.
Differential Diagnosis of Vertigo
| Condition | Key distinguishing features |
|---|---|
| BPPV | Brief episodes (<1 min), positional trigger, Dix-Hallpike positive |
| Vestibular neuritis | Sustained vertigo (days), no hearing loss, no positional trigger |
| Meniere disease | Episodic vertigo + sensorineural hearing loss + tinnitus + aural fullness |
| Central (brainstem/cerebellar) | No latency/fatigue of nystagmus, neurological signs |
Recent Evidence (2024-2026)
A 2024 systematic review (Valsted et al, Am J Audiol, PMID 38900988) compared four repositioning maneuvers for posterior BPPV, and a 2026 meta-analysis (Fu & Zhao, Front Neurol, PMID 42344001) examined differences in therapeutic outcomes between traumatic and idiopathic BPPV - these broadly support current management approaches with canalith repositioning as first-line therapy.
A video demonstrating the Dix-Hallpike and Epley maneuvers:
Sources: Adams and Victor's Principles of Neurology 12th Ed; Shambaugh Surgery of the Ear; Roberts and Hedges' Clinical Procedures in Emergency Medicine; Symptom to Diagnosis: An Evidence-Based Guide, 4th Ed
This is a shared conversation. Sign in to Orris to start your own chat.