Explain about the cholelithesis
"cholelithiasis"[MeSH Terms] AND "pathogenesis"
Cholelithiasis (Gallstones)
Epidemiology
- Affects 10-20% of adults in high-resource countries (western Europe, North America).
- Over 20 million persons in the United States have gallstones, with more than 700,000 cholecystectomies performed annually at a cost of ~$6 billion.
- In the UK, the prevalence at the time of death is estimated at 17%.
- Prevalence among Native Americans (Pima, Hopi, Navajo) approaches 75%.
- Cholesterol stones predominate in the West (90%); pigment stones predominate in parts of Asia (80%).
- 70-80% of patients remain asymptomatic throughout their lives; symptomatic conversion occurs at ~4% per year.
Classification and Types
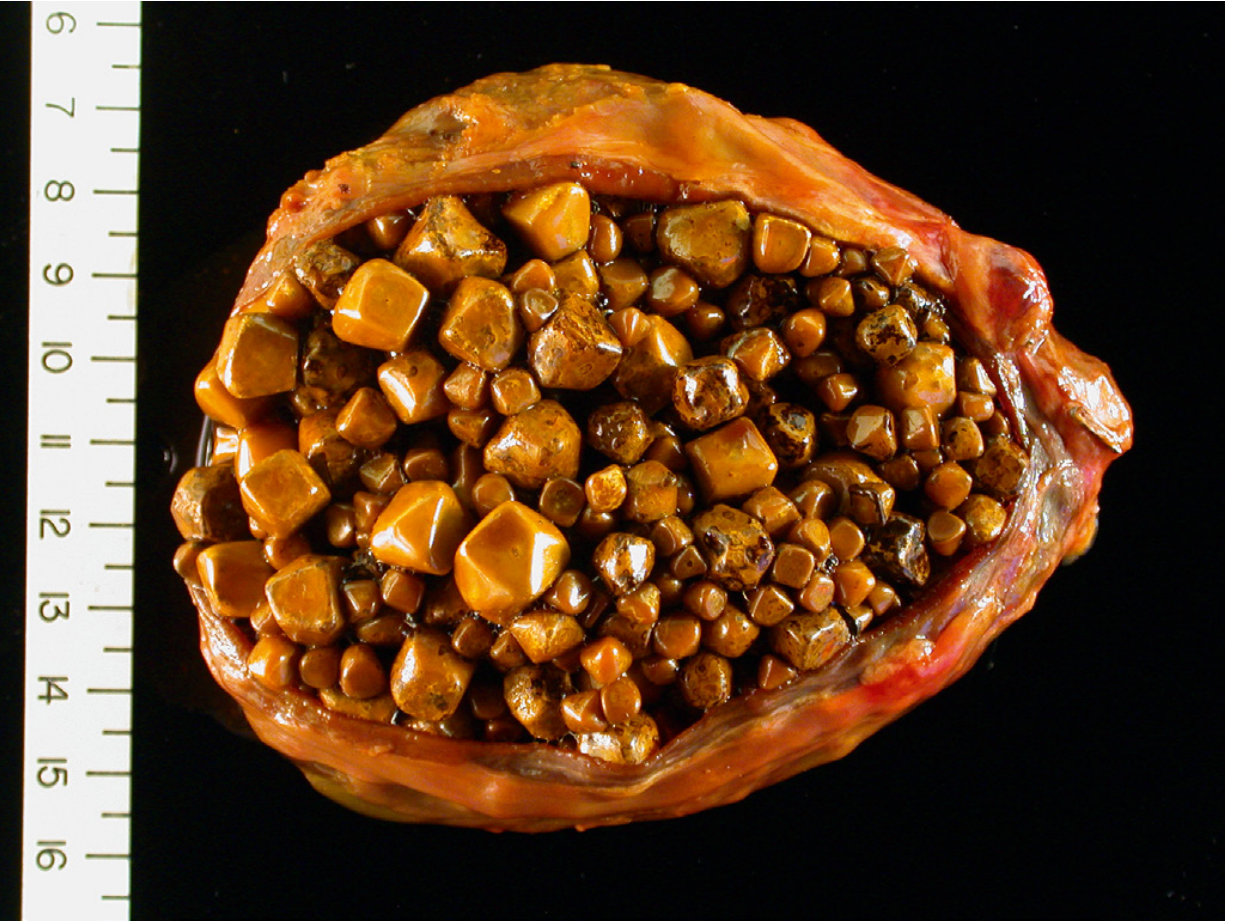
1. Cholesterol Stones (>50% crystalline cholesterol monohydrate)
- Composition: 50-99% cholesterol, plus calcium salts, bile acids, bile pigments, and phospholipids.
- Appearance: Pale yellow, round to ovoid, hard external surface with a radiating crystalline palisade on cross-section. Multiple stones are typical and may be faceted.
- Radiology: Mostly radiolucent (10-20% have enough calcium carbonate to be radiopaque).
- Form exclusively in the gallbladder.
2. Pigment Stones (<30% cholesterol)
- Composed of oxidized polymers of calcium salts of unconjugated bilirubin, calcium carbonate, calcium phosphate, and mucin glycoprotein.
- Found in sterile gallbladder bile.
- Associated with chronic hemolytic anemia (sickle cell disease, hereditary spherocytosis), cirrhosis, and mechanical heart valves.
- Contain calcium bilirubinate, calcium palmitate, calcium stearate, and cholesterol.
- Found in infected bile ducts.
- Related to bile stasis, infection, and deconjugation of bilirubin by bacterial beta-glucuronidase.
- Associated with biliary parasites (Clonorchis sinensis, Ascaris lumbricoides) and bile duct stents.

Risk Factors
Cholesterol Stones
| Category | Risk Factors |
|---|---|
| Demographics | Northern Europeans, North/South Americans, Native Americans |
| Age/Sex | Middle to older age; female sex (hypersecretion of biliary cholesterol) |
| Hormonal | Oral contraceptives, pregnancy, estrogen therapy |
| Metabolic | Obesity, metabolic syndrome, hyperlipidemia, rapid weight loss |
| Acquired | Gallbladder stasis (neurogenic or hormonal), total parenteral nutrition |
| Genetic | ABCG8 gene variant (sterol transporter); inborn bile acid metabolism disorders |
Pigment Stones
| Category | Risk Factors |
|---|---|
| Demographics | Rural > urban; Asia |
| Hemolytic | Sickle cell disease, hereditary spherocytosis, thalassemia, mechanical heart valves |
| Infection | Biliary bacteria (E. coli), parasites (Ascaris, Clonorchis) |
| GI disorders | Ileal disease (Crohn's), ileal resection or bypass, cystic fibrosis with pancreatic insufficiency |
| Cirrhosis | Increased incidence for unclear reasons |
Pathogenesis
Cholesterol Stone Formation
- Supersaturation of bile with cholesterol - when cholesterol concentrations exceed the solubilizing capacity of bile, nucleation into solid cholesterol monohydrate crystals occurs.
- Gallbladder hypomotility - stasis allows crystal aggregation; removing stones without removing the gallbladder invariably leads to recurrence.
- Accelerated cholesterol crystal nucleation - from unstable unilamellar phospholipid vesicles.
- Hypersecretion of gallbladder mucus - traps nucleated crystals, leading to progressive accretion into macroscopic stones.
Pigment Stone Formation
- Bacterial infection of the biliary tree releases microbial beta-glucuronidases, which hydrolyze bilirubin glucuronides (from E. coli, Ascaris, liver flukes).
- Chronic hemolytic anemia increases secretion of conjugated bilirubin; ~1% undergoes spontaneous deconjugation in the biliary tree - enough to precipitate pigment stones over time.
Clinical Features
- Episodic, severe, constant (not truly "colicky") pain in the right upper quadrant or epigastrium.
- Radiates to the right shoulder or back.
- Typically follows a fatty meal that triggers gallbladder contraction against an obstructing stone.
- Episodes last 30 minutes to several hours.
| Complication | Description |
|---|---|
| Acute cholecystitis | Inflammation from stone obstructing the cystic duct; RUQ pain, fever, Murphy's sign |
| Choledocholithiasis | Stone migration into common bile duct; obstructive jaundice |
| Cholangitis | Infection of the biliary tree (Charcot's triad: fever, jaundice, RUQ pain) |
| Acute pancreatitis | Small stones ("travel") are most dangerous; they obstruct the ampulla of Vater |
| Empyema | Pus-filled gallbladder |
| Perforation | May lead to peritonitis or pericholecystic abscess |
| Gallstone ileus | Large stone erodes through gallbladder into small bowel; impaction ~60 cm proximal to the ileocecal valve. Rigler's triad: small bowel obstruction + pneumobilia + ectopic calcification |
| Bouveret syndrome | Stone erosion directly into the duodenum causing gastric outlet obstruction |
| Gallbladder carcinoma | Increased risk with chronic cholelithiasis |
Note: Small stones are more dangerous than large ones because they can migrate into the cystic and common bile ducts. Large stones are more likely to remain in the gallbladder but can erode into adjacent bowel.
Diagnosis
- Ultrasound (first-line): Highly sensitive and specific for gallstones; shows acoustic shadowing. Also detects wall thickening, pericholecystic fluid, and dilated ducts. It is the investigation of choice in pregnancy.
- Plain X-ray: Only 10-20% of cholesterol stones are radiopaque; 50% of pigment stones are radiopaque.
- CT scan: Detects complications (perforation, abscess, pancreatitis) but less sensitive than US for gallstones themselves.
- MRCP (MR cholangiopancreatography): Best non-invasive modality for bile duct stones (choledocholithiasis).
- ERCP: Both diagnostic and therapeutic for common bile duct stones.
- Labs: In uncomplicated cholelithiasis, labs are normal. Elevated bilirubin, ALP, and GGT suggest ductal obstruction; elevated amylase/lipase suggest pancreatitis.
Management
Asymptomatic Cholelithiasis
- Generally watchful waiting is appropriate; prophylactic cholecystectomy is not routinely indicated.
- Exceptions: patients undergoing bariatric surgery, immunocompromised patients, or those with porcelain gallbladder.
Symptomatic Cholelithiasis
- Laparoscopic cholecystectomy is the gold standard - it definitively treats the disease and prevents recurrence.
- Removing stones alone (without the gallbladder) leads to inevitable recurrence because the underlying defect in bile composition and gallbladder motility persists.
Special Considerations
- Pregnancy: Laparoscopic cholecystectomy is preferred in the first or second trimester for symptomatic disease; associated with lower fetal and maternal complications than the open approach. Gallstone pancreatitis in pregnancy carries a maternal mortality of 15% and fetal mortality of 60%, strongly supporting surgical intervention.
- Bariatric surgery: Rapid weight loss after RYGB carries a ~30% risk of new gallstone formation. Prophylactic ursodiol 300-400 mg twice daily for 6 months reduces this to ~4%. Synchronous cholecystectomy is recommended for those with existing biliary pathology.
- Non-surgical options: Ursodeoxycholic acid (UDCA) can dissolve small cholesterol stones in selected patients but requires months of therapy and stones recur when stopped. Rarely used today given the safety of laparoscopic surgery.
Summary Table
| Feature | Cholesterol Stones | Black Pigment Stones | Brown Pigment Stones |
|---|---|---|---|
| Composition | >50% cholesterol | Calcium bilirubinate polymer | Calcium bilirubinate + fatty acids |
| Location | Gallbladder | Gallbladder | Bile ducts |
| Bile | Sterile | Sterile | Infected |
| Radiopacity | Mostly radiolucent | Radiopaque | Radiolucent |
| Key associations | Obesity, OCP, pregnancy | Hemolysis, cirrhosis | Biliary infection, parasites |
| Prevalence (West) | ~80% | ~20% | Uncommon |
Create a comparison poster: Cholesterol vs. Pigment stones
A clean, professional medical comparison poster titled "Cholesterol vs. Pigment Gallstones" with two clearly divided columns side by side. Left column header: "CHOLESTEROL STONES" with a yellow/golden color theme. Contains sections with icons: - Composition: >50% crystalline cholesterol monohydrate + calcium salts, bile acids, phospholipids - Appearance: Pale yellow, round to ovoid, faceted, glistening radiating crystalline surface on cut section - Location: Gallbladder only - Radiology: Mostly RADIOLUCENT (10-20% radiopaque) - Prevalence: 80% in Western countries - Pathogenesis: Bile supersaturation with cholesterol → crystal nucleation → stone accretion; gallbladder hypomotility; mucus hypersecretion - Risk Factors: Female sex, obesity, OCP/pregnancy, rapid weight loss, advancing age, North/South Americans, Native Americans, metabolic syndrome, ABCG8 gene variant Right column split into two sub-columns: Sub-column: "BLACK PIGMENT STONES" with dark/black color theme: - Composition: Calcium bilirubinate polymer + calcium carbonate & phosphate - Appearance: Black, small, multiple, hard, irregular - Location: Gallbladder (sterile bile) - Radiology: RADIOPAQUE - Prevalence: Common in hemolytic disease - Pathogenesis: Elevated unconjugated bilirubin → precipitation of calcium bilirubinate - Risk Factors: Chronic hemolytic anemia (sickle cell, spherocytosis), cirrhosis, mechanical heart valves, Gilbert syndrome Sub-column: "BROWN PIGMENT STONES" with brown/tan color theme: - Composition: Calcium bilirubinate + calcium palmitate/stearate + cholesterol - Appearance: Brown, soft, earthy, laminated - Location: Bile ducts (infected bile) - Radiology: Radiolucent - Prevalence: Common in Asia - Pathogenesis: Bacterial β-glucuronidase hydrolyzes bilirubin glucuronides → unconjugated bilirubin precipitates - Risk Factors: Biliary infection (E. coli), parasites (Ascaris, Clonorchis sinensis), biliary stents, bile stasis Bottom section: A comparison row highlighting key differences: "Small stones most dangerous - can migrate to CBD & cause pancreatitis or cholangitis" Footer: "Treatment: Laparoscopic Cholecystectomy (gold standard)" Clean white background, color-coded sections, medical icons for each category, bold headers, professional typography, well-organized layout with clear visual hierarchy.
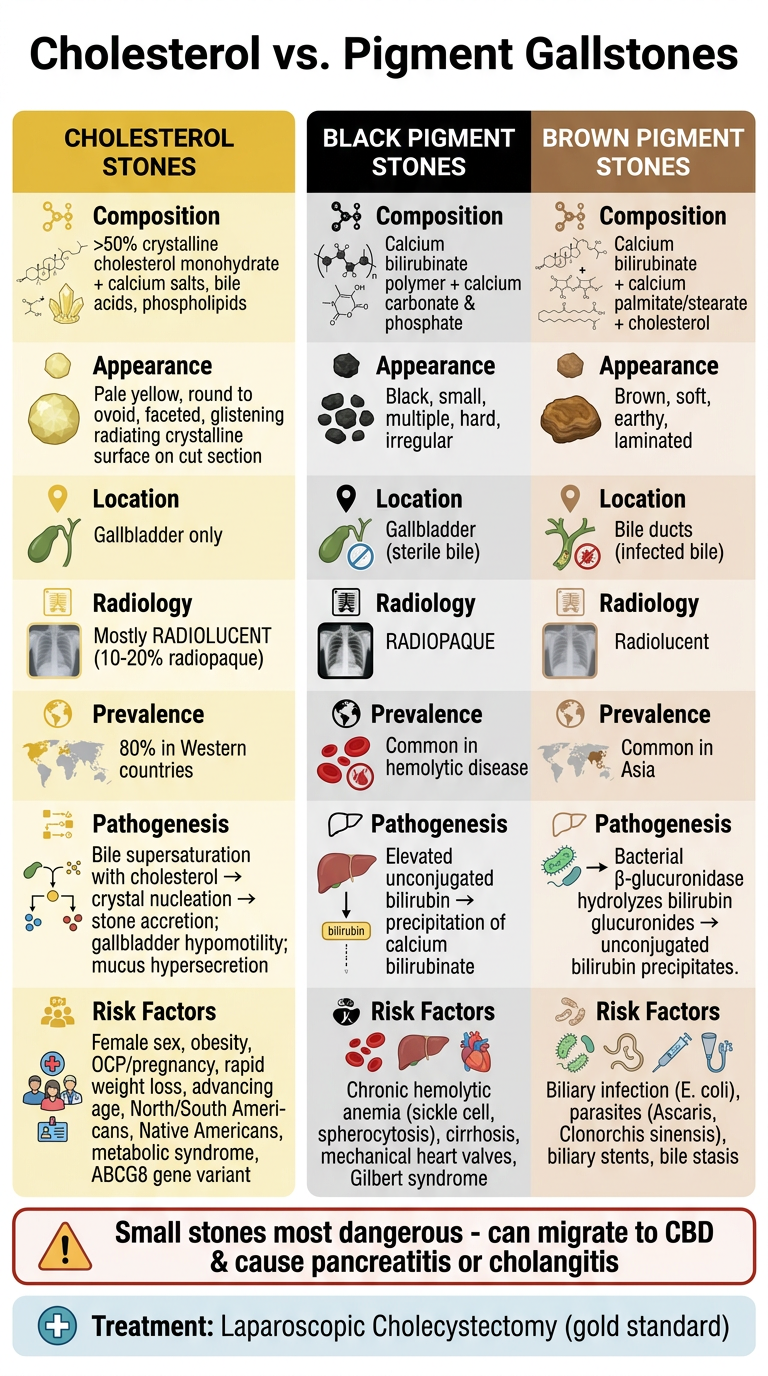
- Cholesterol stones (left, yellow) - the dominant type in Western countries, driven by bile supersaturation, obesity, hormonal factors, and gallbladder stasis.
- Black pigment stones (center, dark) - sterile gallbladder bile, linked to hemolytic conditions and cirrhosis.
- Brown pigment stones (right, brown) - infected bile ducts, associated with bacterial beta-glucuronidase activity and biliary parasites.