Explain hypertension
Reading File
Finding Sources
Searching PubMed
"hypertension"[MeSH Terms] AND "management"[MeSH Terms]
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have everything needed for a comprehensive answer. Let me compile the full explanation.
Hypertension
Hypertension (high blood pressure) is one of the most common and clinically significant chronic conditions worldwide. It is a sustained elevation of arterial blood pressure above normal thresholds that, over time, damages blood vessels and target organs.
1. Definition and Classification
The American College of Cardiology/American Heart Association (ACC/AHA) 2017 classification for adults is the current standard:
| Category | Systolic (mmHg) | Diastolic (mmHg) | |
|---|---|---|---|
| Normal BP | < 120 | and | < 80 |
| Elevated BP | 120–129 | and | < 80 |
| Stage 1 Hypertension | 130–139 | or | 80–89 |
| Stage 2 Hypertension | ≥ 140 | or | ≥ 90 |
When SBP and DBP fall in different categories, the higher classification applies. Diagnosis requires averaging two or more readings at two or more separate visits. In children under 13, hypertension is defined as BP at or above the 95th percentile for age, sex, and height. - Harrison's Principles of Internal Medicine 22E, p. 288
2. Epidemiology
By the criteria above, over 40% of adults in the United States are hypertensive. Prevalence rises with age and is highest in African Americans compared to European Americans, Asian Americans, and Latin Americans. Without treatment, approximately half of hypertensive patients die of ischemic heart disease or heart failure, and about one-third succumb to stroke. - Robbins & Kumar Basic Pathology, p. 311
3. Types of Hypertension
Primary (Essential) Hypertension
- Accounts for 90–95% of all cases
- No single identifiable cause; results from interplay of genetic and environmental factors
- Compatible with long life unless a complication supervenes
Secondary Hypertension
Accounts for the remaining 5–10%. Known causes include:
-
Renal: Acute/chronic glomerulonephritis, polycystic kidney disease, renal artery stenosis, renin-producing tumors
-
Endocrine: Primary aldosteronism (Conn's syndrome), Cushing syndrome, pheochromocytoma, acromegaly, hypo/hyperthyroidism
-
Cardiovascular: Coarctation of the aorta, increased intravascular volume
-
Neurologic / Other: Obstructive sleep apnea, increased intracranial pressure, oral contraceptives/exogenous estrogen, sympathomimetics
-
Robbins & Kumar Basic Pathology, Table 8.1
4. Pathophysiology
Arterial blood pressure = Cardiac Output × Peripheral Vascular Resistance
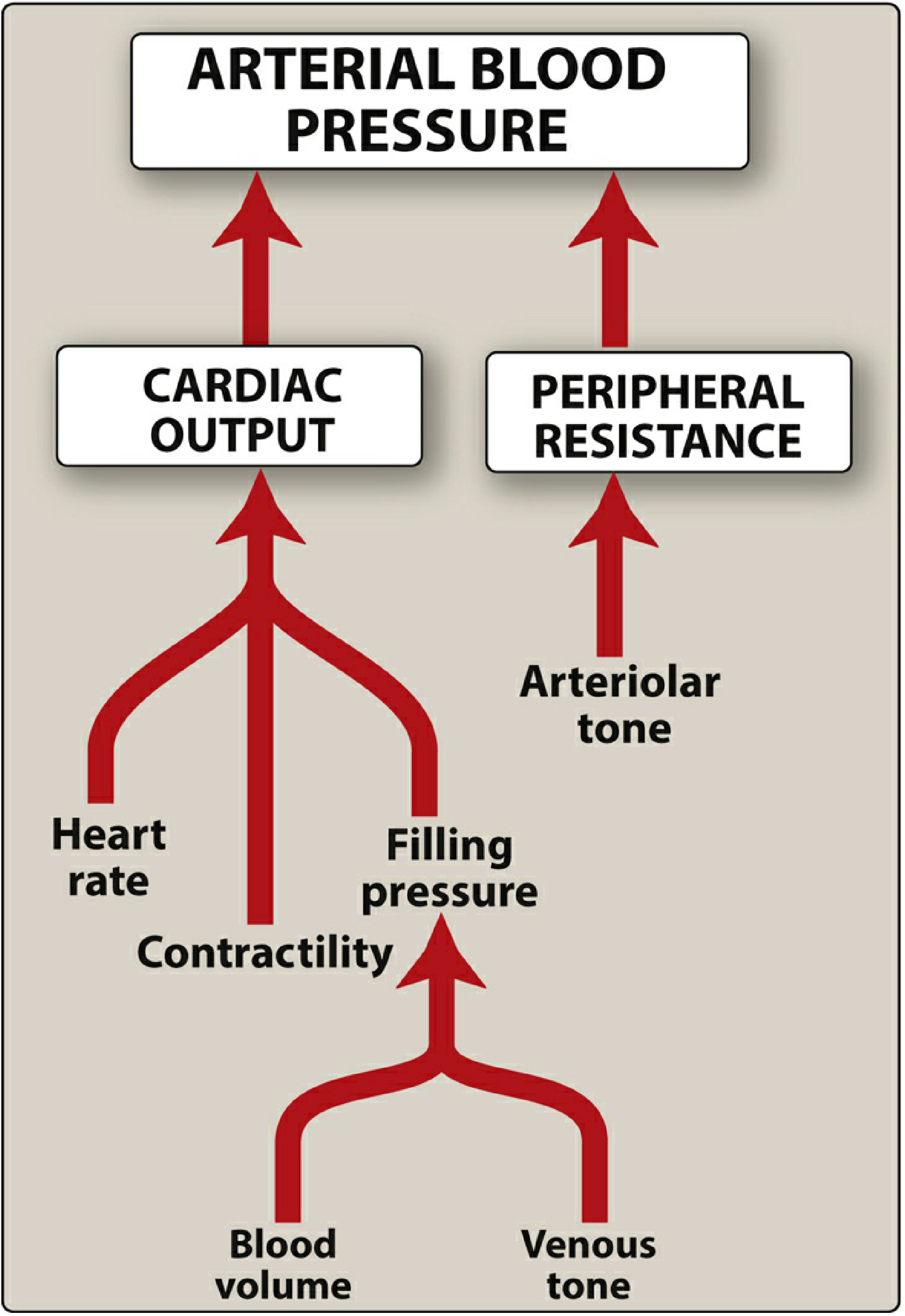
Two major regulatory systems keep BP in balance:
A. Autonomic Nervous System
Baroreceptors in the aortic arch and carotid sinuses detect pressure changes. A fall in BP triggers increased sympathetic and decreased parasympathetic output, causing vasoconstriction and raised cardiac output. Moment-to-moment regulation works through this reflex arc. - Lippincott Pharmacology, p. 292
B. Renin-Angiotensin-Aldosterone System (RAAS)
When renal baroreceptors detect reduced arterial pressure, the kidney releases renin, which converts angiotensinogen → Angiotensin I → Angiotensin II (via ACE). Angiotensin II:
- Causes potent vasoconstriction (arterioles and veins)
- Stimulates aldosterone secretion → increased renal Na⁺ reabsorption → increased blood volume
- Preferentially constricts efferent renal arterioles, raising glomerular filtration pressure
C. Pathogenesis of Primary Hypertension
The exact trigger remains unknown, but the key mechanisms are:
- Impaired renal sodium excretion - reduced Na⁺ excretion at normal pressure forces volume expansion and raises cardiac output; at the new elevated pressure, Na⁺ balance is restored but at the cost of chronically high BP
- Increased vascular resistance - from vasoconstriction and structural thickening of vessel walls
- Obesity and excess adiposity - may account for 65–75% of risk; mechanisms include increased sympathetic activity (partly via leptin signaling), elevated Angiotensin II and aldosterone, and physical renal compression
- Genetic factors - familial clustering and twin studies confirm heritability; polymorphisms in the renin-angiotensin system, renal sodium transport genes, and endogenous pressor genes contribute
- Environmental factors - high dietary sodium, stress, physical inactivity, smoking all amplify genetic predisposition
- Guyton & Hall Textbook of Medical Physiology, p. 246–247; Robbins & Kumar Basic Pathology, p. 311
5. Vascular Pathology (Morphology)
Hypertension drives characteristic vascular injury:
-
Hyaline arteriolosclerosis - thickening of arteriolar walls with deposition of homogeneous pink hyaline material, luminal narrowing; caused by plasma protein leakage and increased ECM production in response to hemodynamic stress. In the kidney, this causes nephrosclerosis (glomerular scarring)
-
Hyperplastic arteriolosclerosis - seen in severe/malignant hypertension; "onion-skin" concentric laminated thickening of arteriolar walls with SMC layers and reduplicated basement membrane; may be accompanied by fibrinoid necrosis
-
Large vessel disease - accelerates atherogenesis; degenerative changes in large/medium arteries can cause aortic dissection and cerebrovascular hemorrhage
-
Robbins & Kumar Basic Pathology, p. 311
6. Clinical Presentation and Complications
Hypertension is called the "silent killer" because it is usually asymptomatic until target-organ damage occurs. End-organ damage affects:
| Organ | Complication |
|---|---|
| Heart | Left ventricular hypertrophy, heart failure, coronary artery disease, MI |
| Brain | Stroke (hemorrhagic and ischemic), hypertensive encephalopathy |
| Kidneys | Nephrosclerosis, chronic kidney disease |
| Eyes | Hypertensive retinopathy |
| Peripheral vasculature | Peripheral artery disease (2.5× risk in men, 3.9× in women) |
A small subset (~5%) present with hypertensive crisis (BP > 180/120 mmHg), which may be:
- Urgency: Severely elevated BP without acute target-organ damage
- Emergency: Severely elevated BP with acute damage (aortic dissection, hypertensive encephalopathy, acute pulmonary edema, MI)
7. Diagnosis
- Confirm with average of ≥2 readings at ≥2 separate visits
- White coat hypertension (elevated only in office) can be identified with ambulatory blood pressure monitoring (ABPM) or home monitoring
- Assess for secondary causes: renal function, urinalysis, electrolytes, lipid panel, thyroid function, aldosterone-to-renin ratio if primary aldosteronism suspected
- Screen for end-organ damage: ECG/echo for LVH, fundoscopy, urinary albumin
8. Treatment
Lifestyle Modifications (First-line for all stages)
- Weight loss (obesity accounts for a large portion of risk)
- Regular aerobic exercise
- DASH diet (high in fruits, vegetables, low-fat dairy; low in sodium)
- Sodium restriction (< 2.3 g/day)
- Alcohol moderation
- Smoking cessation
Pharmacologic Treatment
First-line drug classes (per ACC/AHA and Brenner & Rector's The Kidney):
| Drug Class | Examples | Key Use |
|---|---|---|
| Thiazide/thiazide-like diuretics | Chlorthalidone (preferred), HCTZ | First-line monotherapy; chlorthalidone is more potent than HCTZ |
| ACE inhibitors | Lisinopril, enalapril | First-line; preferred in CKD, diabetes, heart failure |
| Angiotensin Receptor Blockers (ARBs) | Losartan, valsartan | Alternative to ACE inhibitors (avoid ACE inhibitor cough) |
| Calcium channel blockers (CCBs) | Amlodipine, diltiazem | First-line; useful in elderly, isolated systolic hypertension |
Combination strategies:
- ACE inhibitor/ARB + CCB or thiazide are highly effective combinations
- ACE inhibitor/ARB + CCB reduces pedal edema (a common CCB side effect)
- Triple-pill combinations (ARB + CCB + HCTZ) are FDA-approved for moderate-to-severe hypertension
- Do NOT combine ACE inhibitor + ARB (dual RAAS blockade increases adverse effects)
Special populations:
- CKD or proteinuria: ACE inhibitor or ARB preferred (renoprotective)
- Diabetes: ACE inhibitor or ARB; BP target generally < 130/80 mmHg
- Heart failure with reduced EF: ACE inhibitor/ARB, beta-blocker, aldosterone antagonist
- Pregnancy: Labetalol, nifedipine, methyldopa are safe; ACE inhibitors and ARBs are contraindicated
BP targets:
-
General: < 130/80 mmHg (ACC/AHA 2017)
-
If existing CV disease or 10-year CVD risk > 10%: < 130/80 mmHg
-
Elderly (cautious approach): may target < 150/90 mmHg depending on frailty
-
Brenner and Rector's The Kidney; Lippincott Illustrated Reviews Pharmacology; Comprehensive Clinical Nephrology 7e
9. Hypertension in Special Contexts
Hypertension in Pregnancy
Preeclampsia is defined as BP ≥ 140/90 mmHg after 20 weeks' gestation (confirmed on two readings ≥ 4 hours apart) plus proteinuria ≥ 300 mg/24h, or, in the absence of proteinuria, thrombocytopenia, renal insufficiency, impaired liver function, pulmonary edema, or cerebral/visual symptoms. Severe hypertension (≥ 160/105) can herald eclampsia (seizures) and must be treated urgently. - Brenner and Rector's The Kidney, Table 48.3
Resistant Hypertension
BP that remains above goal despite three optimally dosed drugs from different classes (including a diuretic). Obstructive sleep apnea is a common reversible cause; CPAP has been shown to reduce BP in resistant hypertension. - Textbook of Family Medicine 9e
Summary
Hypertension is a sustained elevation in blood pressure (≥ 130/80 mmHg by ACC/AHA criteria) affecting >40% of U.S. adults. The vast majority (~90–95%) is primary/essential, with no single cause but driven by RAAS activation, sympathetic overactivity, impaired renal sodium handling, obesity, and genetic factors. It silently damages the heart, brain, kidneys, and blood vessels. Treatment begins with lifestyle modification and, when indicated, pharmacotherapy with thiazide diuretics, ACE inhibitors/ARBs, or CCBs - chosen based on comorbidities and patient profile. With proper management, hypertension-related morbidity and mortality are substantially reduced.
This is a shared conversation. Sign in to Orris to start your own chat.