Ischemic stroke history
Reading File
Finding Sources
Finding Sources
Searching PubMed
"ischemic stroke"[MeSH Terms] AND "history"
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive, well-sourced content from multiple major textbooks. Here is a full, organized account of ischemic stroke.
Ischemic Stroke - A Complete Overview
Definition and Epidemiology
Ischemic stroke accounts for approximately 87% of all strokes. About 600,000 "first-ever" ischemic strokes occur each year in the United States. Strokes of all subtypes are more common in Black and Hispanic populations versus non-Hispanic whites. Although stroke risk increases with age, approximately 3-4% of all strokes occur in patients aged 15-45, and the average age of first stroke has been trending younger. - Rosen's Emergency Medicine, p. 2746
Pathophysiology and Subtypes
1. Large-Vessel Thrombotic (~33% of cases)
Caused by in situ thrombosis at areas of turbulent blood flow - particularly at vessel bifurcations where atherosclerotic plaques form and ulcerate. The internal carotid artery (ICA) distribution is most commonly affected. A stenosis occluding >90% of the vessel diameter causes marked reduction in flow; further ulceration leads to platelet adhesion and clot formation that either embolizes or occludes the artery. - Rosen's, p. 2748
2. Lacunar (Small-Vessel) Strokes (~33%)
Involve small terminal sections of vasculature. Most common in patients with diabetes and hypertension (80-90% of lacunar stroke patients have hypertension). Sites: basal ganglia, thalamus, pons, internal capsule. Size: a few mm to 2 cm. Mechanism: either small emboli or lipohyalinosis (hypertensive cerebral vasculopathy). - Rosen's, p. 2750
3. Cardioembolic (~25%)
Most commonly caused by embolization of mural thrombus in atrial fibrillation - patients with AF have approximately a 5-fold increased risk of stroke. Other sources: aortic atheromas, diseased extracranial arteries (artery-to-artery embolism). A classic example is amaurosis fugax - a carotid plaque embolus to the ophthalmic artery causing transient monocular blindness. - Rosen's, p. 2752
4. Cryptogenic (~33%)
In more than one-third of first-ever strokes, no clear cause is identified. - Rosen's, p. 2746
Causes in Younger Patients (15-45 years)
-
Oral contraceptive use, pregnancy
-
Antiphospholipid antibodies (lupus anticoagulant, anticardiolipin antibodies)
-
Protein S and C deficiencies
-
Sickle cell disease, polycythemia
-
Carotid/vertebral dissection - the leading determined cause in young patients; often follows minor trauma (sneezing, yoga, spinal manipulation, coughing). Associated with fibromuscular dysplasia and connective tissue disorders
-
Fibromuscular dysplasia
-
Migraine with prolonged vasoconstriction (rare)
-
Cocaine and amphetamines (potent vasoconstrictors)
-
Infectious vasculopathies (varicella, fungal meningitis)
-
Rosen's, p. 2754-2758
Clinical Presentation by Territory
Anterior Circulation (ICA, MCA, ACA)
- Contralateral hemiplegia, hemisensory loss
- Aphasia (dominant hemisphere)
- Contralateral gaze deviation
- Contralateral visual field defect
- Deficits limited to one side of the body
Posterior Circulation (Vertebrobasilar)
The most challenging to diagnose - widest variety of symptoms reflecting cranial nerve deficits, cerebellar involvement, and long tract deficits:
-
Loss of consciousness (reticular activating system involvement)
-
Nausea, vomiting (chemoreceptor trigger zone)
-
Vertigo, diplopia, nystagmus, dysarthria, dysphagia
-
Crossed deficits: motor deficit on one side + sensory loss on the other
-
Visual agnosia, alexia, homonymous hemianopsia
-
CN III palsy (tentorial herniation sign)
-
Visual neglect (patient unaware of visual deficit)
-
Ataxia, spasticity
-
Rosen's, p. 2846
Examination
A focused neurological exam should assess:
- Level of consciousness - using GCS (Eye + Verbal + Motor)
- Speech - aphasia vs. dysarthria
- Cranial nerves - pupillary size/reactivity, extraocular movements (CNs III-VI), CN VII (central vs. peripheral: central spares forehead wrinkling), gag reflex
- Motor/sensory - pronator drift (sensitive for motor weakness), double simultaneous extinction (sensory neglect), graphesthesia
- Cerebellar - finger-to-nose, heel-to-shin, gait
- Reflexes - Babinski sign, deep tendon reflexes
Prehospital tools: Cincinnati Prehospital Stroke Scale, Los Angeles Prehospital Stroke Screen. - Rosen's, p. 2848-2856
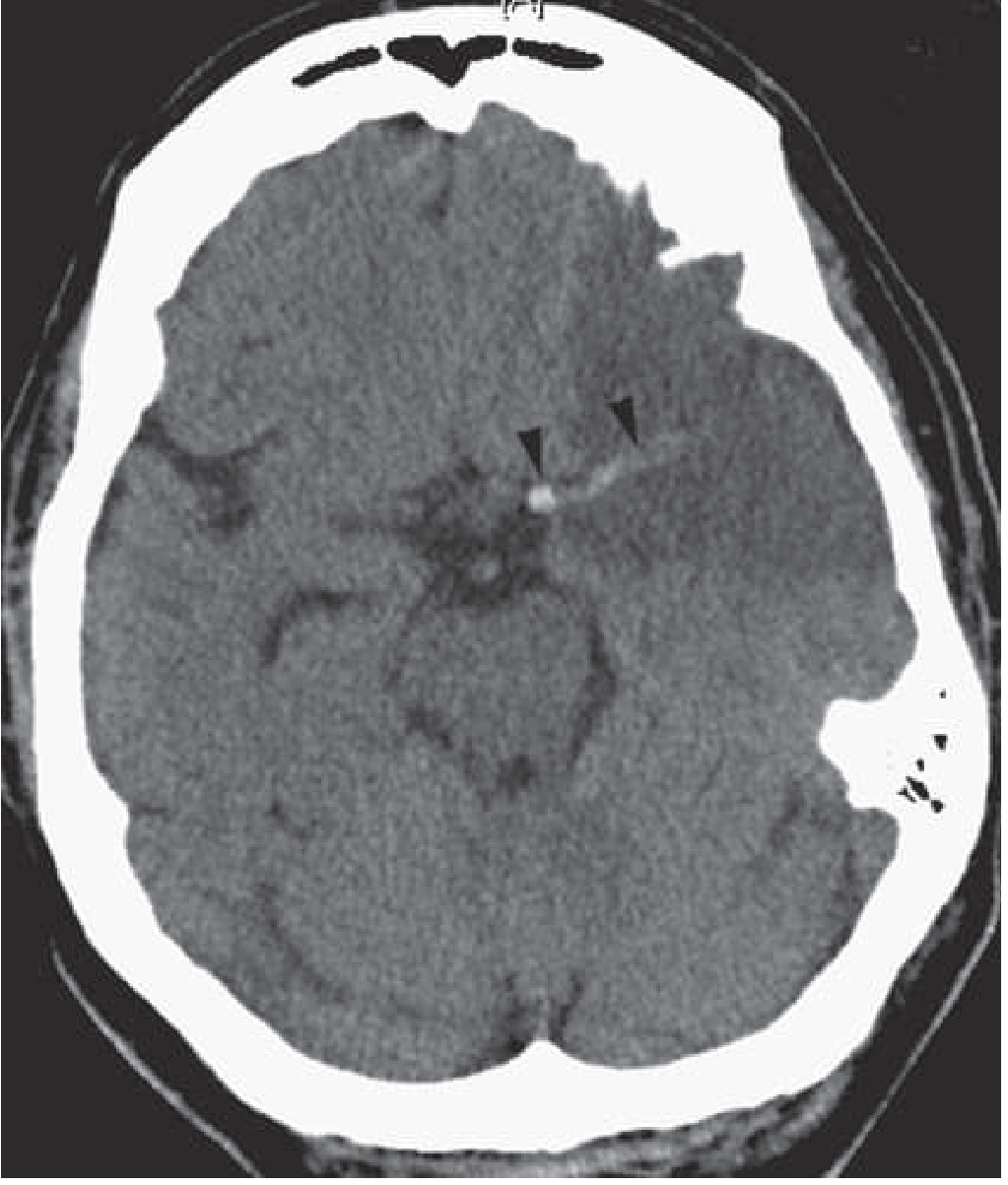
Imaging
CT (Non-contrast)
- First-line: fast, widely available
- Excellent at excluding hemorrhage (hyperdense lesion)
- Early ischemic signs: gray/white junction blurring, sulcal effacement, deep gray matter blurring
- Hyperdense MCA sign (or "hyperdense dot sign"): focal hyperdensity from intraluminal clot
- Limited in posterior fossa (streak artifacts from skull base)
- May be entirely normal in early ischemic stroke
MRI / DWI
-
DWI with ADC mapping is the most sensitive method for acute ischemia - hyperintense signal detectable within minutes of onset
-
Caution: in the first 5-7 days, DWI signal reflects decreased water diffusivity (ischemic cell swelling), then increasingly reflects T2 shine-through from infarcted tissue. Reliable age estimation of a lesion is not possible on DWI alone
-
CT and MR perfusion imaging help identify the ischemic penumbra (at-risk tissue)
-
Bradley & Daroff's, p. 470-474
Differential Diagnosis (Stroke Mimics)
| Mimic | Key Distinguishing Feature |
|---|---|
| Hypoglycemia | Focal deficits that can persist days; check glucose first |
| Wernicke encephalopathy | Ophthalmoplegia + ataxia + confusion; thiamine deficiency |
| Todd's paralysis | Postictal; history of seizure |
| Complex migraine | Focal deficits with/without headache; younger patient |
| Bell's palsy | Peripheral CN VII - forehead wrinkling absent |
| Brain tumor/abscess | Subacute course, fever, systemic signs |
| Ménière disease | Vertigo + tinnitus + hearing loss; no motor/speech deficits |
| Air embolism | History of pressure changes, procedures |
| Giant cell arteritis | Elderly, severe headache, elevated ESR/CRP |
- Rosen's, p. 2920-2939
Acute Management
IV tPA (Alteplase)
- Window: within 4.5 hours of symptom onset (or last known well)
- Also applicable if perfusion-diffusion MRI mismatch is demonstrated
- Prior history of ischemic stroke is a relative contraindication if recent (<3 months)
Mechanical Thrombectomy
- Large vessel occlusion; window extending to 24 hours in selected patients with salvageable penumbra
- Requires CT/MR angiography to confirm occlusion
Blood Pressure
- In fluctuating deficits suggesting large vessel occlusion: avoid aggressive BP lowering, ensure adequate hydration, hold usual antihypertensives to maintain cerebral perfusion
Anticoagulation (when thrombolysis not available)
-
Heparin or LMWH to prevent thrombus propagation, followed by warfarin
-
Adams & Victor's, p. 1166
Secondary Prevention in Patients With Prior Ischemic Stroke / TIA
This is the core clinical challenge when a patient presents with a history of ischemic stroke. - Adams & Victor's, p. 1159-1161
Risk Stratification After TIA
-
~10% stroke risk within 90 days of TIA; nearly half within 2 days
-
Higher risk with: age >60, diabetes, speech/weakness deficits, symptoms >10 min, ischemic MRI lesion
-
After the acute period: ~20% stroke risk over 10 years after a TIA
-
Goldman-Cecil Medicine, p. 2828
Antiplatelets and Anticoagulation
- Atrial fibrillation-related stroke: direct oral anticoagulant (DOAC) or warfarin; recurrence risk 6-10% per year
- Non-cardioembolic stroke: antiplatelet therapy (aspirin, clopidogrel, aspirin/dipyridamole)
- Acute MI-related stroke, valvular disease: warfarin
Statin Therapy
- All patients with prior stroke/TIA + atherosclerotic disease, diabetes, or hyperlipidemia: high-potency statin (atorvastatin 40-80 mg or rosuvastatin 20-40 mg daily) or PCSK9 inhibitor
- Target LDL <70 mg/dL reduces recurrent major cardiovascular events and all-cause recurrent strokes by ~20%
- Stopping a statin acutely in ischemic stroke increases morbidity and mortality
Carotid Revascularization
| Stenosis | Recommendation |
|---|---|
| 70-99% symptomatic extracranial carotid stenosis (within 6 months) | Carotid endarterectomy (CEA) or stenting; reduces recurrence by ~50% |
| 50-69% symptomatic stenosis | Benefit present but smaller (~16% relative reduction) |
| <50% stenosis | No benefit from revascularization |
- Carotid stenting = similar efficacy to CEA overall, but higher stroke risk; patients >70 years do better with CEA, younger patients better with stenting
- Extracranial-intracranial bypass: no benefit, possibly harmful
- Intracranial artery stenting: no benefit vs. medical therapy
Blood Pressure and Metabolic Control
-
Control of hypertension
-
High LDL treatment (above)
-
Pioglitazone (45 mg/day) showed reduced subsequent stroke/MI in patients with prior ischemic stroke/TIA + insulin resistance without overt diabetes in one RCT - awaits wider guideline adoption
-
Goldman-Cecil Medicine, p. 2814-2824
Workup After Established Prior Stroke
Key investigations to identify the etiology and guide prevention:
- Carotid duplex ultrasonography or MRA - to assess ICA patency; if >70% stenosis or severely ulcerated plaque, revascularization indicated
- ECG - detect atrial fibrillation
- Transesophageal echocardiogram - source of embolism
- Cardiac monitoring - prolonged monitoring for paroxysmal AF
- CT/MRI brain - characterize lesion
- Fasting lipids, HbA1c, glucose
The critical mistake is to ignore the potential significance of a prior small stroke or TIA. - Adams & Victor's Principles of Neurology, p. 1161
Sources
- Rosen's Emergency Medicine: Concepts and Clinical Practice, Chapter 87 (Ischemic Stroke), pp. 2746-3053
- Bradley and Daroff's Neurology in Clinical Practice, Chapter 40 & 65 (Ischemic Stroke, Imaging)
- Adams and Victor's Principles of Neurology, 12th Edition, p. 1159-1166
- Goldman-Cecil Medicine, Chapter 376 (Secondary Prevention after Stroke/TIA), pp. 2813-2829
This is a shared conversation. Sign in to Orris to start your own chat.