I now have all the information needed for a thorough viva answer. Let me compose the full response.
Viva Questions & Answers: 12-Year-Old Female with Right Breast Lump (Fibroadenoma)
Sources: Schwartz's Principles of Surgery 11e; Berek & Novak's Gynecology; Mulholland & Greenfield's Surgery 7e
SECTION 1: INTRODUCTION AND DIAGNOSIS
Q1. What is your diagnosis and why?
Most likely diagnosis: Juvenile (Giant) Fibroadenoma of the right breast.
Reasoning:
- Age 12, early reproductive years (peak age 10-25)
- Lump is firm, smooth, freely mobile (no fixation, no skin tethering, no nipple retraction)
- No pain (fibroadenomas classically non-tender)
- No inflammatory signs
- Rapidly enlarging to 7x6x3 cm - this qualifies as a giant fibroadenoma (>5 cm by most definitions, some use >3 cm)
- No family history of breast malignancy
- Regular menstrual cycle
The diagnosis falls within the ANDI (Aberrations of Normal Development and Involution) classification - a fibroadenoma in the early reproductive years is an aberration of normal lobular development, not a malignancy. - Schwartz's Principles of Surgery, p. 578
Q2. What is the ANDI classification? Where does this case fit?
ANDI places benign breast conditions along a spectrum from Normal → Disorder → Disease, across three reproductive phases:
| Period | Normal | Disorder | Disease |
|---|
| Early reproductive (15-25 y) | Lobular/stromal development | Fibroadenoma | Giant fibroadenoma, multiple fibroadenomas |
| Mature reproductive (25-40 y) | Cyclic hormonal changes | Cyclic mastalgia, nodularity | - |
| Involution (35-55 y) | Lobular/ductal involution | Macrocysts, sclerosing lesions | Epithelial hyperplasia with atypia |
This 12-year-old patient falls at the disease end of the early reproductive period because the size (7 cm) constitutes a giant fibroadenoma. - Berek & Novak's Gynecology, p. 979-980
Q3. Define fibroadenoma. What type is this?
A fibroadenoma is a benign fibroepithelial tumor composed of both epithelial (glandular) and stromal (fibrous) elements. It is the most common benign tumor of the breast.
Classification relevant to this case:
- Simple fibroadenoma: ≤3 cm, in women 15-35 years
- Giant fibroadenoma: >5 cm (some define >3 cm); uncommon
- Juvenile fibroadenoma: occurs in girls aged 10-18 years, can range 5-20 cm, rapid growth pattern
- Complex fibroadenoma: fibroadenoma associated with sclerosing adenosis, papillary apocrine changes, ductal epithelial hyperplasia - slightly higher cancer risk
This case is a juvenile giant fibroadenoma given the patient's age (12) and size (7x6x3 cm). - Mulholland & Greenfield's Surgery 7e, p. 3904
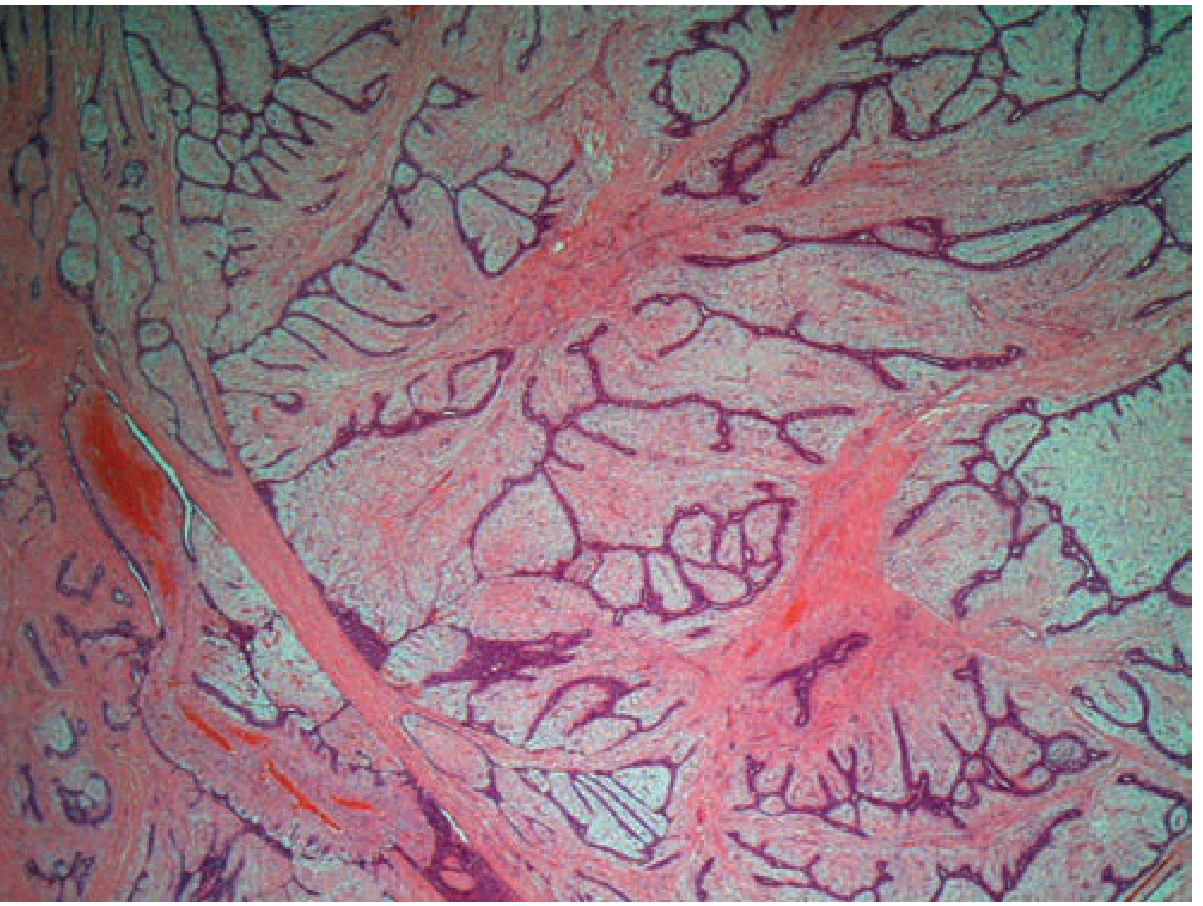
Q4. What is the histopathology of fibroadenoma?
Microscopically:
- Proliferation of both stromal and epithelial (glandular) components
- Well-circumscribed with a pseudocapsule
- Two architectural patterns:
- Intracanalicular: stromal proliferation compresses glands into slit-like spaces
- Pericanalicular: gland lumina remain open and round, surrounded by stroma
- In older/postmenopausal lesions: calcifications may be present in stroma
Fibroadenoma histology (40x) - Schwartz's Principles of Surgery
Q5. What are the clinical features of fibroadenoma? Do they match this case?
Classic features (all present in this case):
| Feature | Expected | This Case |
|---|
| Age | 15-25 y (juvenile: 10-18 y) | 12 y ✓ |
| Consistency | Firm, rubbery, smooth | Present ✓ |
| Mobility | Freely mobile ("breast mouse") | Freely mobile ✓ |
| Pain | Non-tender | No pain ✓ |
| Skin changes | Absent | Absent ✓ |
| Nipple retraction | Absent | Absent ✓ |
| Family history | Not causally linked | Negative ✓ |
The term "breast mouse" is used because the tumor slips away under the examining fingers due to its free mobility. - Berek & Novak's Gynecology, p. 980
Q6. What is the quadrant classification of the breast?
The breast is divided into 4 quadrants by lines passing through the nipple:
- Upper Outer Quadrant (UOQ) - most common site of breast pathology (~50% of cancers)
- Upper Inner Quadrant (UIQ) - this patient's lump is here
- Lower Outer Quadrant (LOQ)
- Lower Inner Quadrant (LIQ)
- Central/Subareolar area
The axillary tail of Spence extends from the upper outer quadrant toward the axilla. Fibroadenomas can occur in any quadrant.
SECTION 2: INVESTIGATIONS
Q7. How would you investigate this patient?
Triple Assessment is the gold standard for any breast lump:
- Clinical examination (already done - freely mobile, non-tender, well-defined)
- Imaging
- Ultrasound (preferred in young patients <30 y) - expect a well-defined, smooth, oblong, solid hypoechoic mass with clearly defined margins
- Mammography has limited utility in dense adolescent breast tissue; not routinely used in this age group
- Tissue sampling (biopsy)
- Core needle biopsy (CNB) or FNAC (fine needle aspiration cytology)
- If imaging is classic for fibroadenoma in a young patient, biopsy may be deferred, but given the size (7 cm) and need to exclude phyllodes tumor, core biopsy is strongly recommended
Q8. What is the imaging finding of fibroadenoma on ultrasound?
- Well-defined, smooth borders
- Oblong/ovoid shape
- Solid, homogeneous internal echotexture
- Hypoechoic compared to surrounding breast tissue
- May show posterior acoustic enhancement
- No irregular margins, no microcalcifications (which would suggest malignancy)
Q9. What is the differential diagnosis?
| Diagnosis | Features that differentiate |
|---|
| Juvenile fibroadenoma (most likely) | Age 10-18, rapid growth, freely mobile, non-tender |
| Phyllodes tumor | Often history of stable lump that suddenly enlarges; leaf-like architecture histologically; must always be excluded in large/growing lumps |
| Breast abscess | Tender, erythematous, fluctuant, fever |
| Lipoma | Soft, lobulated, non-glandular origin |
| Breast cyst | Fluctuant, often tender pre-menstrually; common >25 y |
| Carcinoma | Fixed, hard, irregular, skin changes, lymphadenopathy - very rare at age 12 |
Key exam point: The most important differential to exclude in this case is Phyllodes tumor, which may be clinically indistinguishable from a giant fibroadenoma and shares similar histological features. Histology is required to differentiate.
SECTION 3: MANAGEMENT
Q10. What is the management of this patient?
Given this is a 7 cm juvenile fibroadenoma (giant fibroadenoma) in a 12-year-old:
Surgical excision is indicated for the following reasons:
- Size >3-5 cm (giant)
- Rapid enlargement
- Cosmetic distress (at this age, a 7 cm lump is cosmetically and psychologically significant)
- Need to exclude phyllodes tumor
Surgical considerations:
- Conservative excision preserving breast parenchyma - this is critical in a prepubertal/pubertal girl to avoid damaging the breast bud and future breast development
- Incision choice: periareolar or along skin lines to minimize scarring
- Send specimen for histopathology
If it were small (<3 cm) and classic: Conservative management with watchful waiting (serial ultrasound) is acceptable because:
- 15% regress spontaneously
- 75-85% remain stable
- 5-10% progress - Berek & Novak's Gynecology, p. 981
Q11. What are the risks of surgical excision in a 12-year-old?
- Damage to the breast bud: surgery on a developing breast can impair normal breast development and cause asymmetry/deformity
- Recurrence: fibroadenomas may recur, especially if incompletely excised
- Scarring
- The operating surgeon must be careful to excise the mass while preserving surrounding normal breast tissue, especially the retroareolar tissue - Mulholland & Greenfield's Surgery 7e
Q12. What is the natural history of fibroadenoma?
- ~15% regress spontaneously (involution)
- ~75-80% remain stable in size
- Only 5-10% grow progressively
- Fibroadenomas do not transform into malignancy (standard simple fibroadenomas carry no increased breast cancer risk)
- In complex fibroadenomas, there is a marginally increased risk
- In pregnancy/lactation, may enlarge due to hormonal influence and then regress postpartum - Berek & Novak's Gynecology, p. 981
SECTION 4: PROGESTERONE PILLS AND FIBROADENOMA
Q13. Is there a relationship between progesterone pills (taken for short menstrual cycle) and fibroadenoma?
This is an important and nuanced question. The relationship is complex and the evidence cuts both ways:
Fibroadenomas are estrogen-sensitive tumors:
- It is well established that fibroadenomas are responsive to estrogen stimulation - they occur in premenopausal women, enlarge in pregnancy (high estrogen state), and regress after menopause (low estrogen state) - Berek & Novak's Gynecology, p. 980
Role of progesterone:
- Fibroadenoma cells express both estrogen receptors (ER) and progesterone receptors (PR)
- In recent (cellular, low-fibrosis) fibroadenomas, progesterone receptors are present and high. Progestogen therapy in these cases has actually been associated with regression of fibroadenomas in some older studies (Kuttenn et al., 1983)
- A French cohort study found a positive association between progestin use and the evolution (growth/multiplication) of multiple fibroadenomas - progestins and multiple fibroadenomas study
- Combined oral contraceptives (containing both estrogen and progestogen), however, have been shown in epidemiological studies to reduce the incidence of fibroadenoma by 30-50%, possibly by suppressing ovulation and stabilizing hormonal cycling
Verdict for this case:
- The patient took progesterone alone (not combined OCP) for short menstrual cycle
- Exogenous progestogens can influence fibroadenoma behavior via PR receptor stimulation
- Whether this caused or accelerated her fibroadenoma cannot be stated definitively - the fibroadenoma may have developed independently in the background of her pubertal hormonal environment
- However, progestin exposure is biologically plausible as a contributing factor to growth of an existing fibroadenoma given its receptor sensitivity
- This is an area of ongoing research and the relationship is not definitively causal
SECTION 5: SHORT MENSTRUAL CYCLE AND FIBROADENOMA
Q14. Is there a relationship between a 15-day (short) menstrual cycle and fibroadenoma?
Normal menstrual cycle: 21-35 days. A cycle of 15 days is called polymenorrhea (abnormally frequent menstruation).
Physiological basis:
- A short cycle means more frequent follicular phases - each follicular phase produces a surge of estrogen (estradiol)
- Greater cumulative estrogen exposure over time = more frequent and prolonged estrogen stimulation of breast tissue
- Fibroadenomas are estrogen-responsive - increased estrogen exposure promotes lobular proliferation, which underpins fibroadenoma formation
- The peri-ovulatory estrogen surge also triggers progesterone from the corpus luteum - so short cycles = more frequent hormonal fluctuations
Implications for this patient:
- 15-day cycles mean approximately double the monthly estrogen surges compared to a normal 30-day cycle
- This chronic, frequent hormonal stimulation of estrogen-sensitive breast stroma could plausibly drive or accelerate fibroadenoma growth
- Short cycles are also often associated with a shortened or inadequate luteal phase, which means relative progesterone deficiency with relative estrogen excess - this state of estrogen dominance is linked to benign breast disease (fibrocystic disease, fibroadenomas)
Important note: This is a pathophysiological association, not a proven direct causation. No high-quality randomized data establishes that polymenorrhea directly causes fibroadenoma. However, the hormonal basis (estrogen-sensitivity of fibroadenoma + high estrogen burden from short cycles) is mechanistically sound.
Q15. Why did the treating doctor prescribe progesterone pills for the short cycle?
- Short cycles (polymenorrhea) often reflect shortened follicular phase or anovulation with inadequate progesterone production
- Progesterone supplementation helps lengthen the luteal phase and regularize the cycle
- In gynecological practice, micronized progesterone or synthetic progestins are prescribed in the second half of the cycle to support cycle regulation
- This is a common clinical approach for dysfunctional uterine bleeding and polymenorrhea in adolescents
SECTION 6: PHYLLODES TUMOR - MUST KNOW DISTINCTION
Q16. How do you differentiate fibroadenoma from phyllodes tumor clinically and histologically?
| Feature | Fibroadenoma | Phyllodes Tumor |
|---|
| Age | 15-35 y (juvenile: 10-18 y) | Late 30s-50s (but can be any age) |
| Growth | Slow, stable after 2-3 cm | Often stable then sudden rapid enlargement |
| Size | Usually 1-3 cm (giant if >3-5 cm) | Often large at presentation (can be >10 cm) |
| Consistency | Firm, rubbery | May be lobulated, cystic areas |
| Bilaterality | Rare | Rarely bilateral |
| Histology | Benign epithelium + stroma in balance | Leaf-like (phyllodes) stromal fronds, stromal overgrowth, mitoses in stromal cells |
| Malignant potential | None (simple) | Benign (60%), Borderline (20%), Malignant (20%) |
| Recurrence | Low | High if incompletely excised |
| Management | Excision or watchful waiting | Wide local excision with clear margins (even for benign) |
This case is suspicious for phyllodes because of the large size (7 cm) and rapid enlargement in a 12-year-old - histopathology after excision is mandatory. - Berek & Novak's Gynecology, p. 981-982
SECTION 7: ADDITIONAL VIVA POINTS
Q17. What is the blood supply of the breast?
- Medial: Internal thoracic (internal mammary) artery perforators
- Lateral: Lateral thoracic artery (branch of axillary artery)
- Superior: Thoracoacromial artery
- Venous drainage parallels arterial supply; deep veins drain to axillary and internal mammary veins
The upper inner quadrant (as in this patient) is supplied primarily by the internal thoracic artery perforators.
Q18. What is the lymphatic drainage of the breast relevant to this case?
- 75% of lymph drains to axillary lymph nodes
- Medial breast (including UIQ where this tumor is) drains to internal mammary nodes
- Supraclavicular and infraclavicular nodes
- Rotter's nodes (interpectoral)
For this patient (UIQ lump), the relevant nodal groups are the axillary AND internal mammary nodes.
Q19. Does fibroadenoma increase risk of breast cancer?
- Simple fibroadenoma: No increased risk
- Complex fibroadenoma (with sclerosing adenosis, apocrine changes, epithelial hyperplasia): ~1.5-2x increased risk compared to general population
- Fibroadenoma occurring in a patient with a first-degree relative with breast cancer: risk is higher but still modest
- Standard fibroadenoma does not undergo malignant transformation - Berek & Novak's Gynecology, p. 981
Q20. What would you counsel this patient and her parents?
- Reassure - this is a benign condition, not cancer
- Explain the diagnosis - a benign tumor of breast tissue, common in young girls
- Surgery is recommended given the large size (7 cm) and need to exclude phyllodes tumor
- Risk of breast bud damage will be minimized by careful surgery
- Recurrence is possible and follow-up will be needed
- Address the progesterone treatment - discuss with their gynecologist regarding continued need
- Menstrual health: investigate further why cycles are only 15 days
Summary Table for Revision
| Feature | Detail |
|---|
| Diagnosis | Juvenile giant fibroadenoma, right UIQ |
| Size | 7x6x3 cm (giant = disease in ANDI) |
| Key clinical sign | Freely mobile, non-tender, no skin/nipple changes |
| Investigations | Triple assessment: clinical + ultrasound + core biopsy |
| Must exclude | Phyllodes tumor |
| Management | Surgical excision (conservative, breast-bud sparing) |
| Progesterone link | Biologically plausible (PR receptor expression); progestins may influence growth but evidence not definitively causal |
| Short cycle link | Polymenorrhea → increased estrogen exposure → promotes estrogen-sensitive tumor growth (mechanistically sound, not proven causal) |
| Cancer risk | Not increased for simple fibroadenoma |
| ANDI classification | Early reproductive years, disorder → disease (giant fibroadenoma) |
Key References:
- Schwartz's Principles of Surgery 11e, Chapter 17 (Benign Breast Disorders), pp. 578-582
- Berek & Novak's Gynecology, Chapter 19 (Benign Breast Conditions), pp. 978-985
- Mulholland & Greenfield's Surgery 7e, Chapter on Proliferative Breast Lesions, p. 3904
- Progestins and multiple fibroadenoma evolution (PMC7354733)