Proper systemic anatomy of branchial apparatus in detail. I want to write in a note so give accordingly according to standard ent textbook.
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
I now have comprehensive content from multiple standard ENT and embryology textbooks. Let me compile the detailed note.
BRANCHIAL APPARATUS - SYSTEMATIC ANATOMY
Sources: Scott-Brown's Otorhinolaryngology Head & Neck Surgery (Vol. 1 & 2), Cummings Otolaryngology Head and Neck Surgery, THIEME Atlas of Anatomy (General Anatomy & Musculoskeletal System)
1. INTRODUCTION AND ETYMOLOGY
The term "branchial" is derived from the Greek word "bragchia" meaning gills. The branchial (pharyngeal) apparatus is a series of structures that give the early embryo an appearance resembling the gill apparatus of fish, hence the name. In land-dwelling vertebrates including humans, these are more accurately called pharyngeal arches rather than true branchial arches, but the term "branchial" persists in clinical and surgical use.
2. DEVELOPMENT - TIMELINE
| Week of Gestation | Event |
|---|---|
| Week 4 | Neural crest cells migrate craniocaudally; branchial arches begin to form |
| Week 4-5 | All six arches become apparent; pouches and clefts develop simultaneously |
| Week 5 | Fifth arch obliterates almost immediately after appearing |
| Weeks 3-8 | Entire branchial apparatus development extends across this period |
Development begins during the 4th week of embryonic life, when neural crest cells migrate to the future head and neck region. Within one week, four oblique ridges (first through fourth pharyngeal arches) form at the level of the cranial foregut. Externally, these are separated by four deep grooves called pharyngeal clefts (ectodermal); internally, their counterparts are pharyngeal pouches (endodermal).
3. STRUCTURAL COMPONENTS OF EACH ARCH
Each branchial arch consists of four key components:
- A bar of cartilage (skeletal element) - forms bone, cartilage, or connective tissue
- Musculature (derived from mesoderm of the arch)
- An associated aortic arch artery
- A cranial nerve - the "post-trematic nerve" of that arch; additionally, a "pre-trematic nerve" from the arch below supplies the inner endodermal surface of the arch above
Covering layers:
- External surface covered by ectoderm
- Internal surface lined by endoderm
- Core is mesodermal (pharyngeal arch musculature)
4. SCHEMATIC DIAGRAM OF THE BRANCHIAL APPARATUS
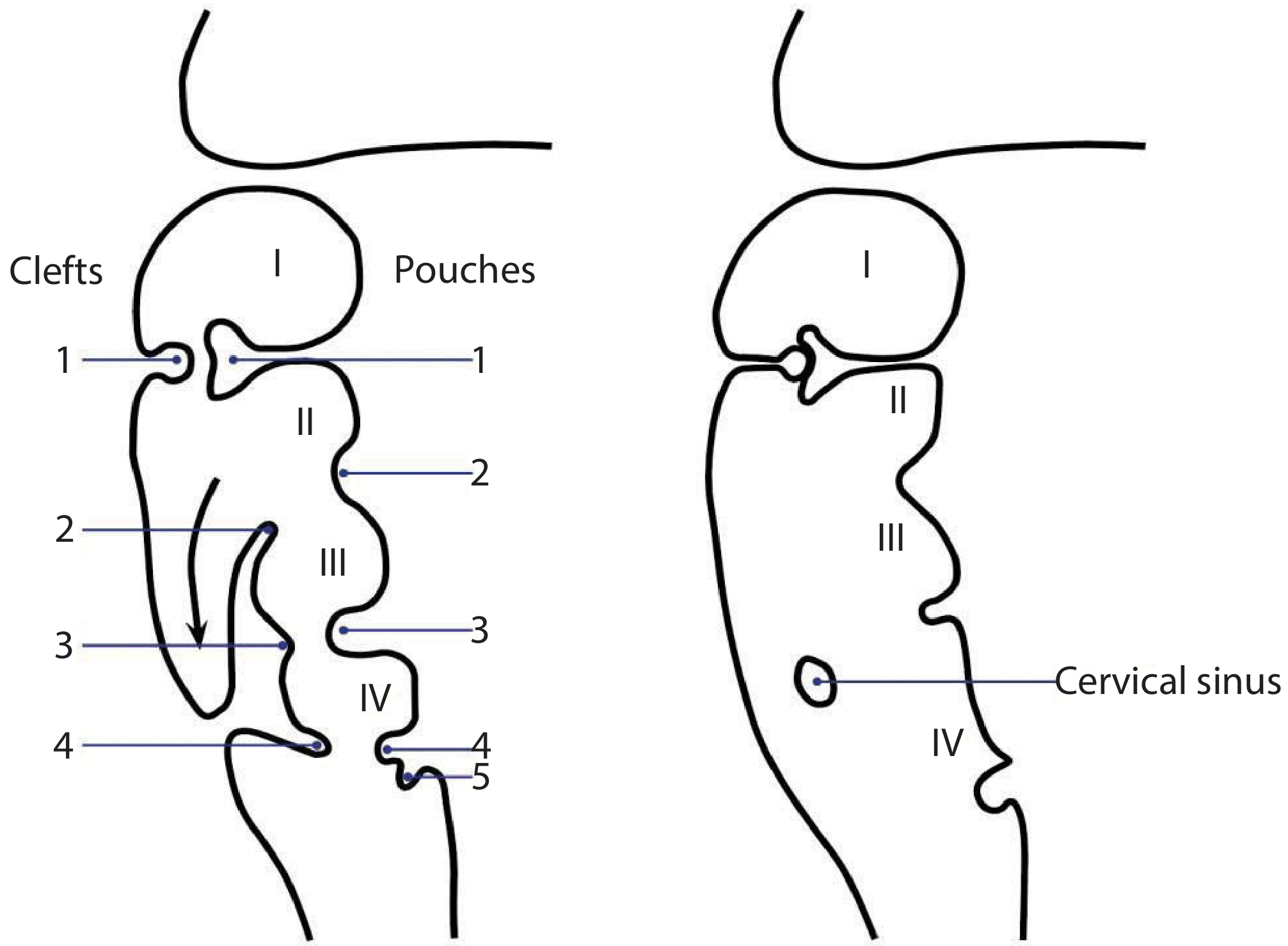
Fig. 1 - Schematic diagram of the branchial apparatus in utero. Left: clefts (ectoderm, external) and pouches (endoderm, internal) numbered 1-4 (with pouch 5). Right: formation of the cervical sinus as arch II overgrows arches III and IV. (Scott-Brown's Otorhinolaryngology)
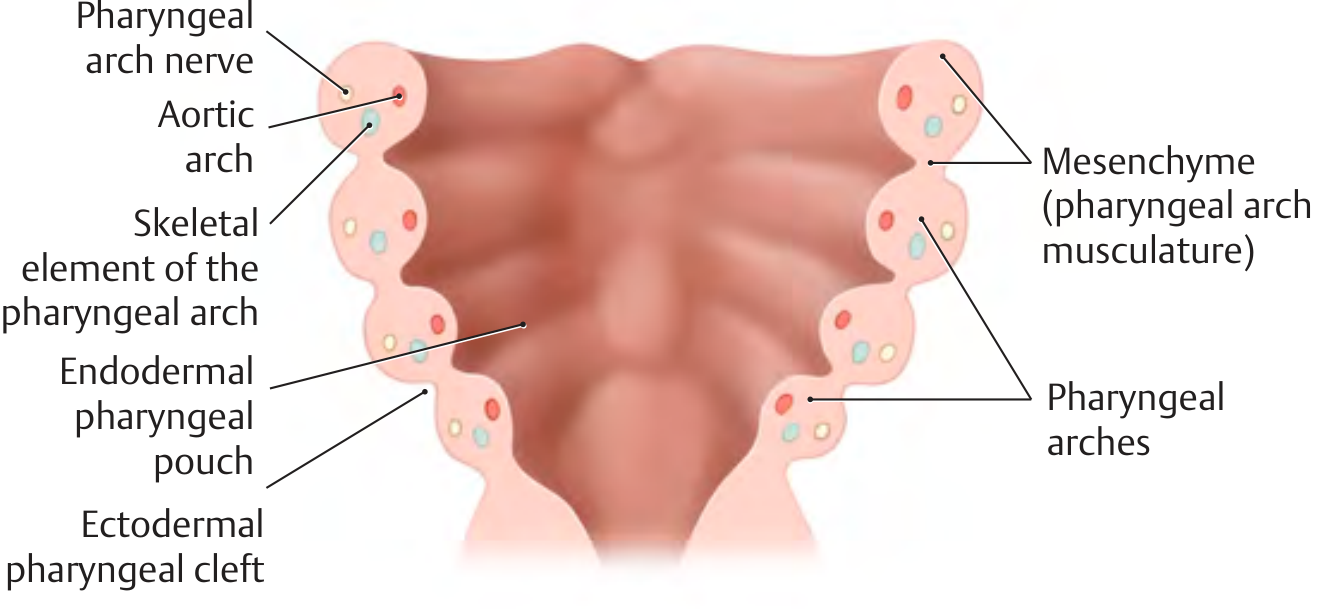
Fig. 2 - Frontal view of the pharyngeal arches showing components of each arch: nerve, aortic arch, skeletal element, and mesenchyme. (THIEME Atlas of Anatomy)
5. THE BRANCHIAL ARCHES - INDIVIDUAL DERIVATIVES
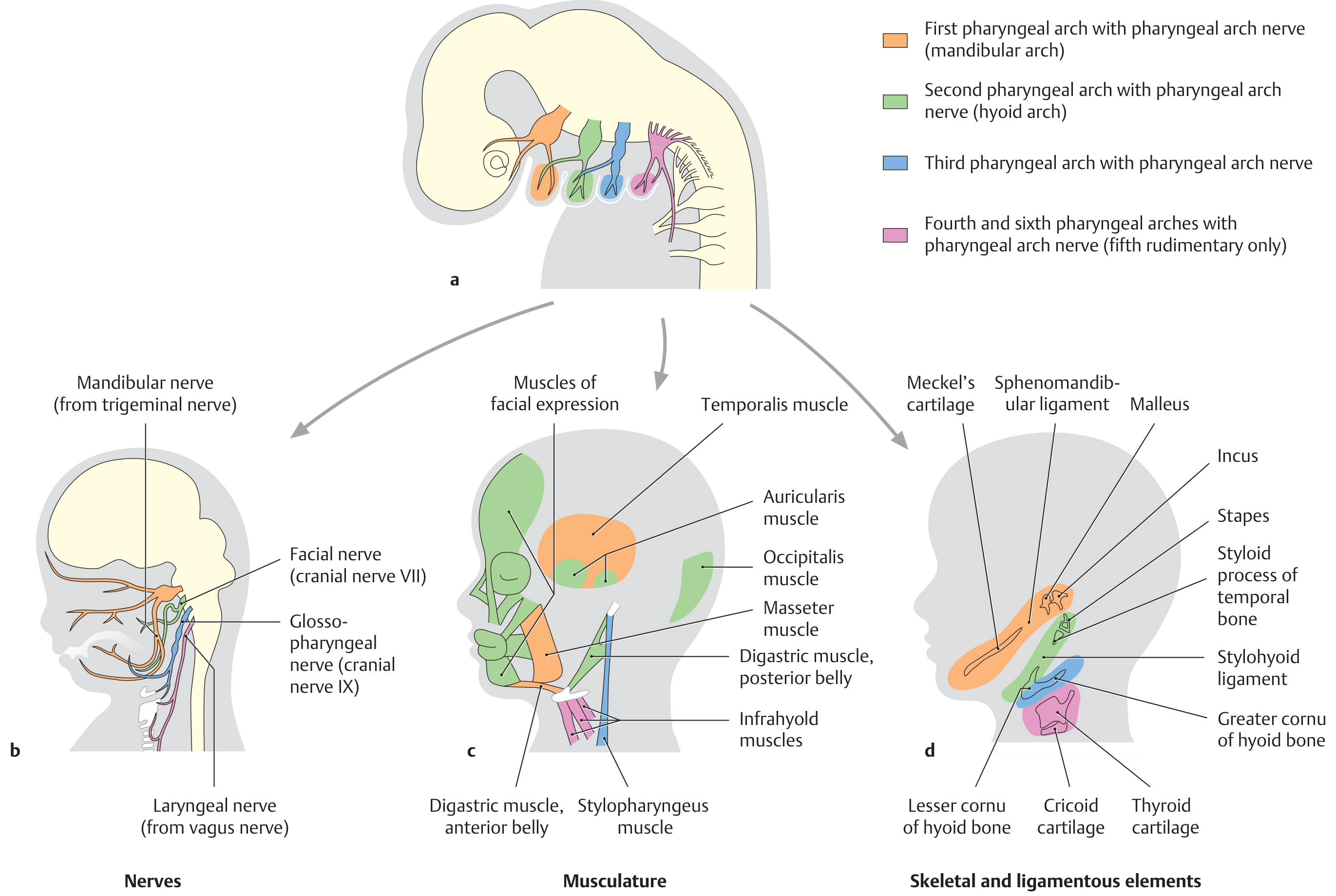
Fig. 3 - Derivatives of pharyngeal arches: (a) embryonic arch arrangement, (b) nerve distribution, (c) muscular derivatives, (d) skeletal and ligamentous derivatives. (THIEME Atlas of Anatomy)
Arch I - Mandibular Arch (First Pharyngeal Arch)
Nerve: CN V - Trigeminal nerve (mandibular division for motor; all three divisions for sensory)
Cartilage: Meckel's cartilage
- Proximal portion - forms the ramus of mandible (via remodelling)
- Distal portion - withers; body of mandible forms by intramembranous ossification
- Also gives: Malleus (except manubrium), Incus (except long process), Sphenomandibular ligament, Anterior malleolar ligament
Maxillary process (dorsal portion of first arch) - forms: premaxilla, maxilla, zygoma, part of temporal bone
Muscles:
- Muscles of mastication: temporalis, masseter, medial pterygoid, lateral pterygoid
- Mylohyoid
- Anterior belly of digastric
- Tensor tympani
- Tensor veli palatini
Artery: First aortic arch artery (contributes to maxillary artery territory)
Arch II - Hyoid Arch (Second Pharyngeal Arch)
Nerve: CN VII - Facial nerve (motor to all muscles of this arch)
- Pre-trematic nerve: Chorda tympani (from CN VII) runs to the first arch territory
Cartilage: Reichert's cartilage
- Proximal portion forms: Stapes suprastructure, Styloid process of temporal bone, Manubrium of malleus, Long process of incus
- Central portion withers leaving: Stylohyoid ligament (fibrous remnant)
- Distal portion forms: Lesser cornu and superior body of hyoid bone
Muscles:
- Muscles of facial expression (all)
- Stylohyoid
- Posterior belly of digastric
- Stapedius
- Auricular muscles, occipitalis
Artery: Stapedial artery (only rarely persists into adult life)
Clinical note: The path of Reichert's cartilage can be traced in the adult from the styloid process through the stylohyoid ligament to the lesser cornu of hyoid - a key surgical landmark.
Arch III (Third Pharyngeal Arch)
Nerve: CN IX - Glossopharyngeal nerve (motor + sensory innervation to parts of pharynx)
- Pre-trematic nerve: Jacobson's nerve (tympanic branch of CN IX) runs to the second arch territory (CN VII)
Cartilage: Forms the greater cornu and inferior body of hyoid bone
Muscles: Stylopharyngeus (the only muscle derived from the third arch)
Artery: Third aortic arch artery - forms common carotid and proximal internal carotid arteries
Arch IV and Arch VI (Fourth, Fifth, and Sixth Arches)
Note: The fifth arch is rudimentary and obliterates almost immediately after forming. Its components are incorporated into the fourth arch in humans.
Nerve: CN X - Vagus nerve
- Fourth arch: superior laryngeal nerve
- Sixth arch: recurrent laryngeal nerve
Cartilage/Skeletal elements (fourth and sixth together): Forms the laryngeal skeleton:
- Thyroid cartilage
- Cricoid cartilage
- Arytenoid cartilage
- Corniculate cartilages
- Cuneiform cartilages
Muscles (fourth arch): Pharyngeal and laryngeal muscles (cricothyroid, constrictors)
Muscles (sixth arch): Intrinsic laryngeal muscles (except cricothyroid)
Artery:
- Fourth arch artery (right) - forms right subclavian artery
- Fourth arch artery (left) - forms the arch of the aorta (between left common carotid and left subclavian)
- Sixth arch artery - forms pulmonary arteries; the left sixth arch persists as the ductus arteriosus until birth
Summary Table: Branchial Arch Derivatives
| Arch | Nerve | Muscles | Cartilage/Skeletal | Artery |
|---|---|---|---|---|
| I (Mandibular) | CN V (trigeminal) | Temporalis, masseter, medial/lateral pterygoid, mylohyoid, ant. belly digastric, tensor tympani, tensor veli palatini | Meckel's cartilage → malleus, incus, mandible, sphenomandibular lig., ant. malleolar lig. | Maxillary artery territory |
| II (Hyoid) | CN VII (facial) | All muscles of facial expression, stylohyoid, post. belly digastric, stapedius | Reichert's cartilage → stapes suprastructure, styloid process, stylohyoid lig., lesser cornu + upper body hyoid | Stapedial artery (transient) |
| III | CN IX (glossopharyngeal) | Stylopharyngeus | Greater cornu + lower body hyoid | Common carotid, proximal internal carotid |
| IV | CN X - superior laryngeal br. | Cricothyroid, pharyngeal constrictors | Thyroid cartilage, part of larynx | Left: aortic arch; Right: right subclavian |
| VI | CN X - recurrent laryngeal br. | Intrinsic laryngeal muscles (except cricothyroid) | Cricoid, arytenoid, corniculate, cuneiform cartilages | Pulmonary arteries; left = ductus arteriosus |
6. BRANCHIAL CLEFTS (ECTODERM - EXTERNAL)
There are four branchial clefts, formed externally between adjacent arches, lined by ectoderm.
Fate of the Clefts
First branchial cleft - the ONLY one that persists in normal development:
- Forms the external auditory canal (EAC)
- Together with the closing plate of the first pouch, forms the outer epithelial layer of the tympanic membrane
- The ectodermal lining of the EAC is derived from this cleft
Second, third, and fourth branchial clefts:
- Normally obliterated as the second arch (hyoid arch) grows caudally to overgrow and submerge the third and fourth arches
- This creates a potential space called the cervical sinus of His, which normally disappears completely
- Failure of obliteration leads to branchial cleft cysts, sinuses, or fistulae
7. BRANCHIAL POUCHES (ENDODERM - INTERNAL)
There are five pharyngeal pouches (though the fifth is rudimentary and often considered part of the fourth).
Pouch I (First Pharyngeal Pouch)
- Elongates laterally to form the tubotympanic recess
- Gives rise to: Eustachian tube (proximal portion) and middle ear cavity (distal/lateral portion)
- The lateral end, together with the closing plate of the first cleft, forms the inner layer of the tympanic membrane
Pouch II (Second Pharyngeal Pouch)
- Endodermal layer forms the epithelial lining of the tonsillar fossa
- Contributes to the palatine tonsil (epithelium; mesenchymal elements incorporate the lymphoid tissue of the tonsil)
- Residual contact between second pouch endoderm and second cleft ectoderm = closing plate that normally disappears
Pouch III (Third Pharyngeal Pouch)
- Divided into superior and inferior portions:
- Superior portion → inferior parathyroid glands (parathyroid III)
- Inferior portion → thymic tissue (migrates caudally and medially into retrosternal mediastinum to form the thymus)
- Because the third pouch derivatives start superiorly and descend, the inferior parathyroid glands end up inferior to the superior parathyroid glands despite their name
Pouch IV (Fourth Pharyngeal Pouch)
- Endoderm forms the superior parathyroid glands (parathyroid IV)
- These descend only slightly, ending up in the superior poles of the thyroid gland
Pouch V (Fifth Pharyngeal Pouch / Ultimobranchial Body)
- Sometimes called the "fifth pouch," "sixth pouch," or ultimobranchial body
- Infiltrated by neural crest cells that migrate to this region
- Incorporated into the thyroid gland as parafollicular C cells (calcitonin-secreting)
Summary Table: Pharyngeal Pouch Derivatives
| Pouch | Derivatives |
|---|---|
| I | Eustachian tube + middle ear cavity (tubotympanic recess); inner layer of tympanic membrane |
| II | Epithelium of tonsillar fossa + palatine tonsil |
| III (superior) | Inferior parathyroid glands (parathyroid III) |
| III (inferior) | Thymus |
| IV | Superior parathyroid glands (parathyroid IV) |
| V (ultimobranchial body) | Parafollicular C cells of thyroid (calcitonin-secreting) |
8. CERVICAL SINUS OF HIS
- Formed when the second arch grows caudally to overgrow the third and fourth arches
- Creates a transient ectodermal-lined space lateral to the neck
- Normally obliterates completely by week 7
- Failure of obliteration results in second branchial cleft cysts (most common branchial anomaly)
- Forms the basis of the cervical sinus theory of branchial cyst formation
9. TONGUE DEVELOPMENT FROM BRANCHIAL ARCHES
- Anterior 2/3 of tongue: lateral lingual swellings + tuberculum impar from arch I
- Sensory: lingual nerve (CN V3)
- Taste: chorda tympani (CN VII branch)
- Posterior 1/3 of tongue: copula/hypobranchial eminence from arches II, III, and IV
- Predominant innervation: CN IX (from arch III)
- Posterior tongue (vallecula) and epiglottis: superior laryngeal nerve (CN X, arch IV)
- Junction: V-shaped terminal sulcus (sulcus terminalis); the foramen caecum marks the apex
- Intrinsic tongue muscles: derived from occipital somite myoblasts that migrate into the tongue, innervated by CN XII (hypoglossal)
10. EAR DEVELOPMENT FROM THE BRANCHIAL APPARATUS
External Ear
- External auditory canal (EAC): from first branchial cleft ectoderm
- Pinna/auricle: from six auricular hillocks (three from arch I, three from arch II) surrounding the first cleft; fully formed by day 60 of gestation
- The first branchial arch artery has a developmental relationship to the pinna (juvenile angiofibroma considerations)
Middle Ear
- Middle ear cavity and Eustachian tube: from first pharyngeal pouch endoderm (tubotympanic recess)
- Tympanic membrane: inner layer from first pouch endoderm, outer layer from first cleft ectoderm, middle fibrous layer from mesoderm
- Ossicular chain:
- Malleus and Incus: first arch (Meckel's cartilage) - except manubrium of malleus and long process of incus which are from second arch
- Stapes suprastructure: second arch (Reichert's cartilage)
- Stapes footplate: largely from the otic capsule (NOT branchial arch)
11. ANOMALIES OF THE BRANCHIAL APPARATUS
Terminology
- Cyst: enclosed epithelial-lined cavity with no opening to skin or pharynx
- Sinus: blind-ended tract opening onto one epithelial surface (external or internal)
- Fistula: tract running from one epithelial surface to another (both external opening on neck skin AND internal opening in pharynx/ear)
First Branchial Cleft Anomalies (rare, ~5% of all branchial anomalies)
- Work Type I: Duplication of the external auditory canal - track in pre/post-auricular region running parallel to EAC, lined by squamous epithelium only; external opening anterior and inferior to tragus
- Work Type II: Duplication of the first arch AND cleft - track runs from skin near angle of mandible to EAC or conchal bowl; lined by squamous epithelium + skin appendages; inconstant relationship to the facial nerve (may run deep or superficial to it)
- Surgery: Complete excision; must identify and preserve facial nerve
Second Branchial Cleft Anomalies (most common, ~95% of all branchial cysts)
- Result from failure of obliteration of the cervical sinus or remnant of second cleft
- External opening: along anterior border of SCM in its lower third
- Internal opening: tonsillar fossa (second pharyngeal pouch territory)
- Track passes between external and internal carotid arteries, lateral to CN IX and XII, medial to CN XI, crossing the hypoglossal nerve
- Lined by stratified squamous epithelium (90%); 10% by respiratory epithelium; 80% have lymphoid tissue in wall with cholesterol crystals in straw-colored fluid
Third Branchial Cleft Anomalies
- External opening: lower anterior border of SCM
- Internal opening: pyriform fossa/posterior larynx (third pouch territory)
- Track passes posterior to internal carotid artery, lateral to CN X, below CN IX
Fourth Branchial Cleft Anomalies
- Extremely rare
- Internal opening: apex of pyriform fossa
- Track descends into the chest (looping around the aortic arch on the left or subclavian artery on the right) then ascends
12. BRANCHIAL CYST - AETIOLOGY THEORIES
Four theories have been proposed (Scott-Brown's):
-
Branchial apparatus theory: Cysts represent remnants of pharyngeal pouches or branchial clefts, or their fusion. Development extends from week 3-8 of gestation. Limitation: if congenital, cysts should be present at birth; peak incidence is 2nd-3rd decade.
-
Cervical sinus (of His) theory: Cysts represent remnants of the cervical sinus, formed as the second arch mesoderm grows down to meet the fifth arch. Second arch mesoderm almost covers the entire neck and forms the platysma muscle.
-
Thymopharyngeal duct theory: Cysts are remnants of the original thymus-third pouch connection. Largely discredited as no persistent thymic duct has been found, and no branchial cyst has been found deep to the thyroid gland.
-
Inclusion theory (currently most favored for classical branchial cysts): Cysts represent epithelial inclusions within cervical lymph nodes. Supported by: (a) presence of lymphoid tissue in 80% of cyst walls; (b) occurrence in the parotid gland and pharynx; (c) absence in neonates; (d) peak onset in second-third decade of life after URTI.
13. CLINICAL RELEVANCE SUMMARY
- Knowledge of branchial anatomy explains the course of fistula tracts (critical for complete surgical excision)
- The facial nerve's relationship to first branchial anomalies requires identification during surgery
- Second branchial cysts can be confused with lymphadenopathy; in adults >40 years, must rule out cystic nodal metastasis (especially from HPV+ oropharyngeal SCC)
- Third and fourth arch anomalies can be managed with endoscopic ablation of the internal opening (pyriform fossa opening) rather than open excision
- Aberrant migration of third pouch derivatives explains ectopic parathyroid and ectopic thymus
- C-cell (parafollicular) tumors (medullary thyroid carcinoma) arise from neural-crest-derived ultimobranchial body remnants incorporated into the thyroid
References: Scott-Brown's Otorhinolaryngology Head & Neck Surgery, 8th Ed. | Cummings Otolaryngology Head and Neck Surgery, 7th Ed. | THIEME Atlas of General Anatomy and Musculoskeletal System
This is a shared conversation. Sign in to Orris to start your own chat.