If I give you the link of a yt vedio can you give me the entire notes of the thing thought in it with images as it is .
- Extract the transcript from the video
- Organize it into structured notes with headings, bullet points, and key concepts
- Include relevant images/diagrams where applicable to match the visual content
https://youtu.be/F_pMLuneImw?si=EXlrpZUTRx0DGc02
youtube video F_pMLuneImw transcript title
video title topic content
transcript content
scapula anatomy labeled diagram glenoid cavity spine process coracoid acromion
🦴 Scapula - Complete Anatomy Notes
Lecture Context: This is the 1st of 3 videos on the Scapula & Humerus series.
- Video 1 (this): Scapula - all features EXCEPT muscle attachments
- Video 2: Humerus - all features EXCEPT muscle attachments
- Video 3: Scapula + Humerus - muscle attachments together (better for visualization & memory)
1. Introduction to Scapula
| Feature | Detail |
|---|---|
| Other name | Shoulder Blade |
| Type of bone | Flat bone |
| Shape | Triangular |
| Location | Posterior thoracic wall |
- Skull protects the brain
- Ribs protect the lungs
- Scapula protects the muscles beneath it
2. Surfaces (2 total)
| Surface | Direction | Faces |
|---|---|---|
| Costal Surface | Anterior (front) | Faces the ribs |
| Dorsal Surface | Posterior (back) | Has the spine process |
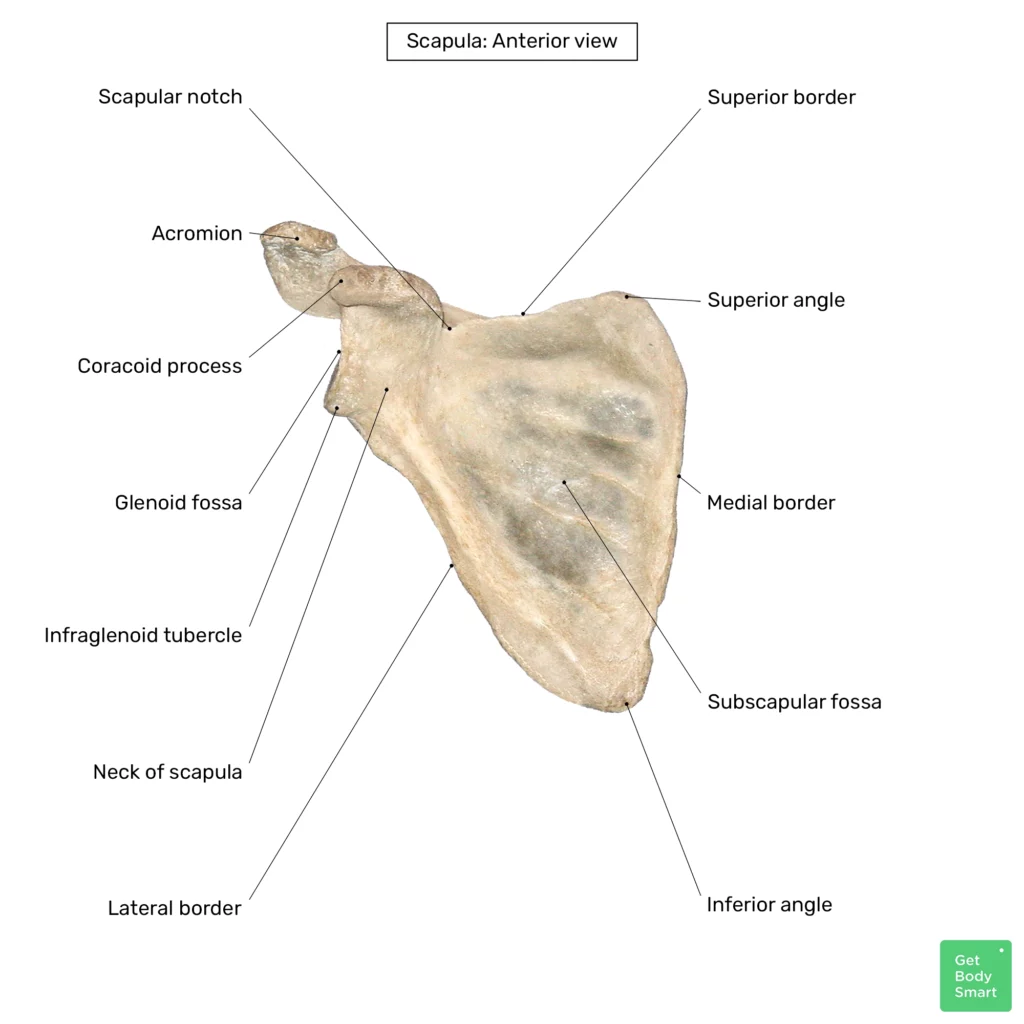

3. Borders (3 total)
| Border | Location |
|---|---|
| Superior Border | Upper edge |
| Medial Border (Vertebral border) | Middle/medial side (towards spine) |
| Lateral Border (Axillary border) | Lateral side (towards humerus) - thicker |
Note: The lateral border is thicker compared to the medial border (which is thin like a blade edge).
4. Angles (3 total)
| Angle | Location |
|---|---|
| Superior Angle | Top of the triangle |
| Inferior Angle | Bottom of the triangle |
| Lateral Angle | Side - where the Glenoid Cavity is located |
5. Processes (3 total)
| Process | Location/Details |
|---|---|
| Acromion Process | Projects superiorly/laterally; overhangs glenoid cavity |
| Coracoid Process | Projects anteriorly |
| Spine (Spinous Process) | On the posterior (dorsal) surface |
All 3 processes project outward (away from the body).
6. Side Determination (Right vs Left Scapula)
Step 1 - Orient Superior/Inferior:
- The glenoid cavity, acromion process, and coracoid process are all on the upper/superior side.
- Place them upward.
Step 2 - Orient Lateral/Medial:
- Glenoid cavity is always on the lateral side.
- Lateral border is thicker than medial border.
- Once glenoid cavity is lateral, the medial border (thinner, blade-like) will be on the other side.
Step 3 - Orient Anterior/Posterior:
- Spine process is on the posterior (dorsal) surface.
- So if you see the spine, you're looking at the back.
| Feature | Position |
|---|---|
| Glenoid Cavity | Lateral side |
| Lateral Border | Thicker |
| Spine Process | Posterior surface |
| Acromion + Coracoid | Superior end |
7. Suprascapular Notch
- Located on the superior border of the scapula
- Covered superiorly by the Suprascapular Ligament
Important Viva Question:
"What passes above and below the suprascapular ligament?"
| Structure | Position |
|---|---|
| Suprascapular Artery | Passes ABOVE the ligament |
| Suprascapular Nerve | Passes BELOW the ligament |
- "Air"force - artery flies above (in the air)
- "Navy" - nerve goes below (under the sea)
8. Glenoid Cavity
- Located at the lateral angle of the scapula
- Articulates with the head of the humerus (forms the shoulder joint)
- It is very shallow - so the humeral head could easily slip out
Glenoid Labrum
- To deepen the glenoid cavity, a fibrocartilage ring called the Glenoid Labrum is attached around its margins
- This makes the cavity deeper and prevents easy dislocation of the humeral head
- Structure: fibrocartilage, attached to the margin, forms a deeper cup shape
Without the labrum, moving your arm even slightly would cause the joint to dislocate.
Tubercles around the Glenoid Cavity:
| Tubercle | Location |
|---|---|
| Supraglenoid Tubercle | Above the glenoid cavity |
| Infraglenoid Tubercle | Below the glenoid cavity |
9. Costal (Anterior) Surface Features
| Feature | Details |
|---|---|
| Subscapular Fossa | A depression (hollow) on the anterior (costal) surface |
| Muscle origin | Subscapularis muscle originates from this fossa |
10. Dorsal (Posterior) Surface Features
| Fossa | Location | Muscle |
|---|---|---|
| Supraspinous Fossa | Above the spine | Supraspinatus muscle (to be covered in Video 3) |
| Infraspinous Fossa | Below the spine | Infraspinatus muscle (to be covered in Video 3) |
11. Quick Summary Table
| Feature | Count | Names |
|---|---|---|
| Surfaces | 2 | Costal (anterior), Dorsal (posterior) |
| Borders | 3 | Superior, Medial, Lateral |
| Angles | 3 | Superior, Inferior, Lateral |
| Processes | 3 | Acromion, Coracoid, Spine |
| Fossae | 3 | Subscapular, Supraspinous, Infraspinous |
| Notch | 1 | Suprascapular notch |
| Tubercles | 2 | Supra- and Infraglenoid tubercles |
12. What's NOT in This Video (Coming Next)
- Muscle attachments of the scapula - will be covered in Video 3 along with humerus attachments together, because most scapular muscles attach onto the humerus - learning them together helps you:
- Visualize better
- Remember more easily
- Understand shoulder joint movements when you get there
Next Video: Humerus anatomy (all features except muscle attachments) Video After: Scapula + Humerus muscle attachments combined
https://youtu.be/cnl_WOHB9Ow?si=zc78eLDdXMKofzX5
youtube cnl_WOHB9Ow title anatomy lecture
anterior abdominal wall layers diagram camper scarpa fascia labeled
anterior abdominal wall blood supply arterial epigastric arteries diagram labeled
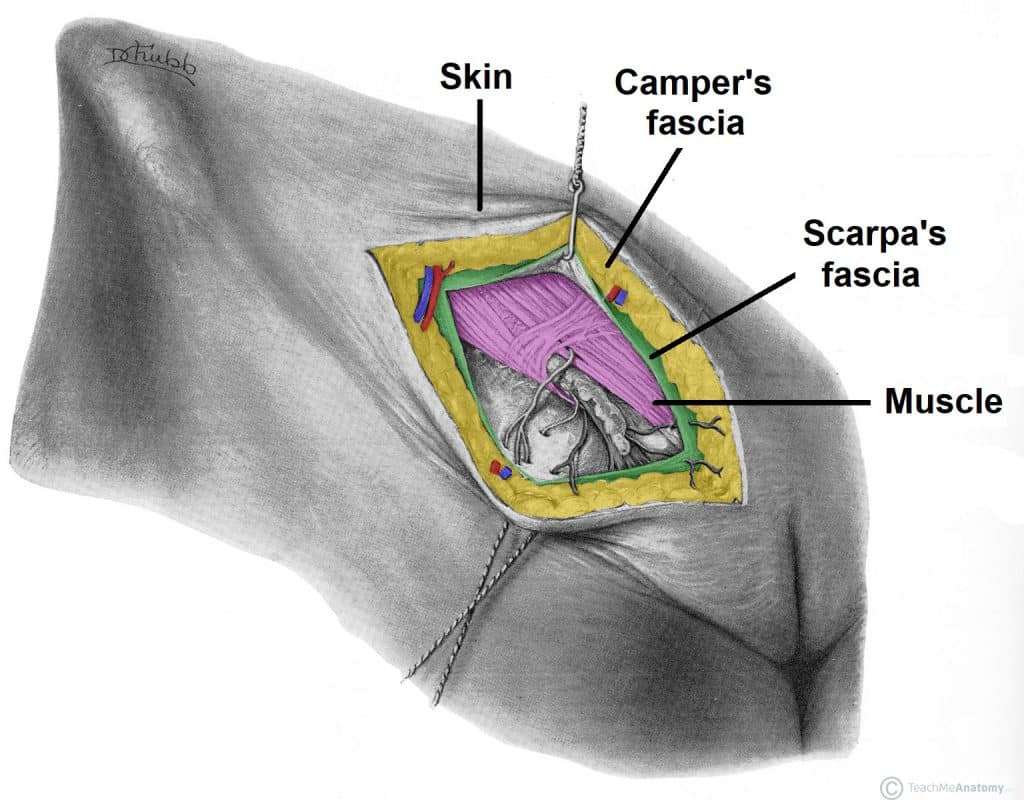
🫁 Superficial Fascia of the Anterior Abdominal Wall
Lecture Context: Part of the "Layers of Anterior Abdominal Wall" series.
- Previous lecture: Umbilicus (Skin of Anterior Abdominal Wall)
- This lecture: Superficial Fascia (Camper's + Scarpa's) in detail
- Next lecture: Muscles of Anterior Abdominal Wall
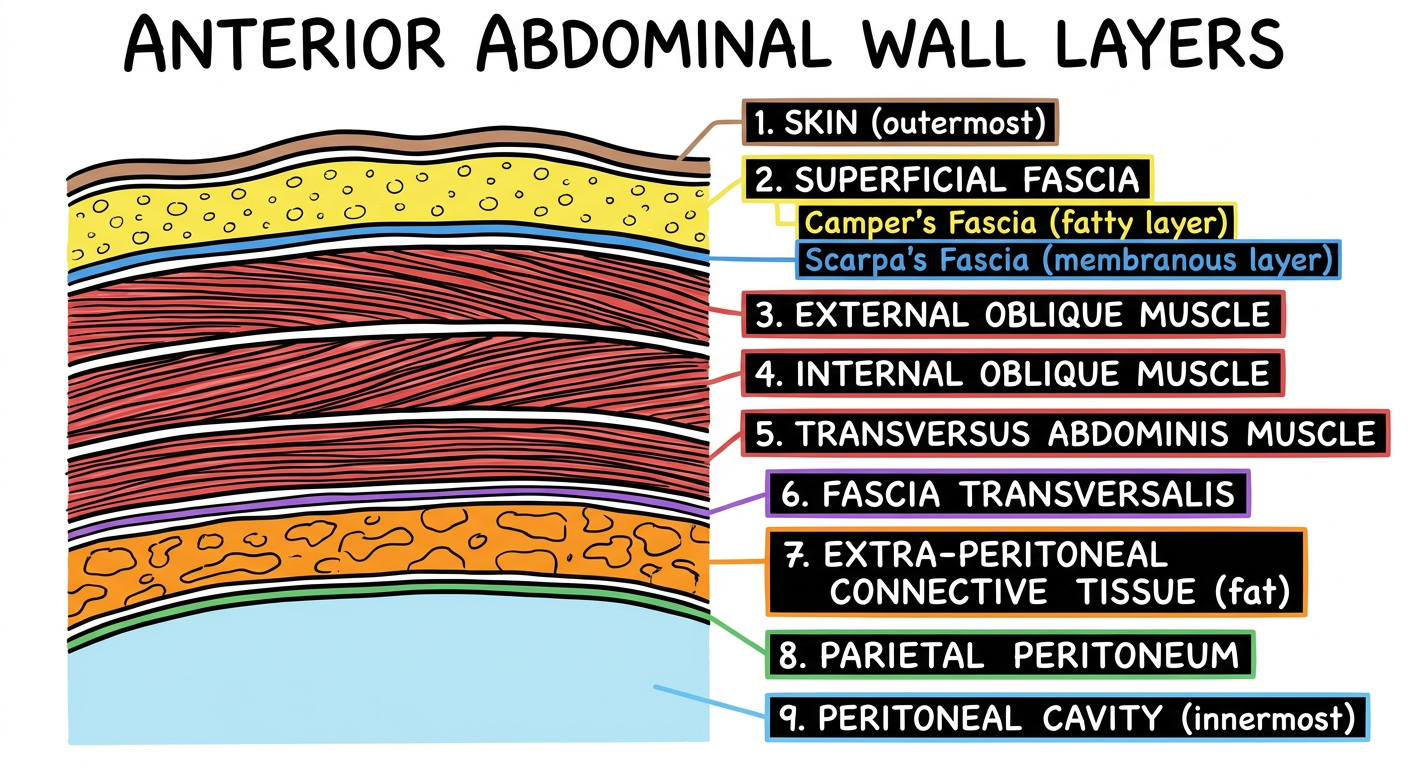
1. Layers of Anterior Abdominal Wall (Overview)
| Order | Layer |
|---|---|
| 1 | Skin |
| 2 | Superficial Fascia (Camper's + Scarpa's) |
| 3 | External Oblique Muscle |
| 4 | Internal Oblique Muscle |
| 5 | Transversus Abdominis Muscle |
| 6 | Fascia Transversalis |
| 7 | Extra-peritoneal Connective Tissue (fatty) |
| 8 | Parietal Peritoneum |
| 9 | Peritoneal Cavity |
2. Why is There NO Deep Fascia in the Abdomen?
This is a high-yield viva question!
- During pregnancy - uterus enlarges
- In obesity - fat accumulates in the abdomen
- After eating - stomach expands
Deep fascia IS present in the penis - called Buck's Fascia.
3. Superficial Fascia - Two Layers
| Layer | Name | Type | Location |
|---|---|---|---|
| Outer | Camper's Fascia | Fatty layer | Superficial / outer |
| Inner | Scarpa's Fascia | Membranous layer | Deep / inner |

4. Below vs Above the Umbilicus
| Region | Distinguishability |
|---|---|
| Above umbilicus | Looks like a single layer - not well-differentiated |
| Below umbilicus | Well-differentiated into Camper's (fatty) and Scarpa's (membranous) |
In obese individuals, the abdomen "hangs" below - that is the thick Camper's fascia storing fat inferiorly.
5. Continuity of Fascia (Most Important Section)
5A. Scarpa's Fascia Continuity (Membranous Layer)
Scarpa's Fascia (abdomen)
↓
Superficial Fascia of Penis
↓
Dartos Muscle (scrotum) ← Main contribution = CAMPER'S fascia
↓
Colles' Fascia (perineum) ← Main contribution = SCARPA'S fascia
↓
Merges with Perineal Membrane
↓
Ends at / merges with Urogenital Diaphragm
5B. Camper's Fascia Continuity (Fatty Layer)
- Camper's fascia is ABSENT in the penis (no fat in the penis)
- Goes to scrotum → forms Dartos Muscle (main contributor)
- Then extends as Colles' Fascia into perineum
Summary Table of Contributions:
| Structure Formed | Main Contributor |
|---|---|
| Dartos Muscle (scrotum) | Camper's Fascia |
| Colles' Fascia (perineum) | Scarpa's Fascia |
6. Scarpa's Fascia extends into Lower Limb
- Scarpa's fascia extends beyond the inguinal ligament into the lower limb
- It extends up to the Holden's Line
What is Holden's Line?
A line connecting both pubic tubercles.
- At Holden's Line, Scarpa's fascia merges with the Deep Fascia of the thigh - i.e., Fascia Lata
| Structure | Boundary |
|---|---|
| Scarpa's Fascia | Extends from abdomen → crosses inguinal ligament → lower limb |
| Ends at | Holden's Line (line connecting both pubic tubercles) |
| Merges with | Fascia Lata (deep fascia of thigh) |
7. Key Points on Perineum Structures (Preview)
| Structure | Role |
|---|---|
| Colles' Fascia + Perineal Membrane | Together, these separate the Superficial Perineal Pouch from the Ischioanal (Ischiorectal) Fossa |
| Superficial Perineal Pouch | Closed posteriorly by the fusion of Colles' Fascia & Perineal Membrane |
| Ischioanal Fossa | Cannot communicate with superficial perineal pouch when they are properly fused |
If Colles' Fascia and Perineal Membrane fail to merge → the two spaces communicate with each other.
8. Watershed Area (Umbilicus)
High-yield concept for exams!
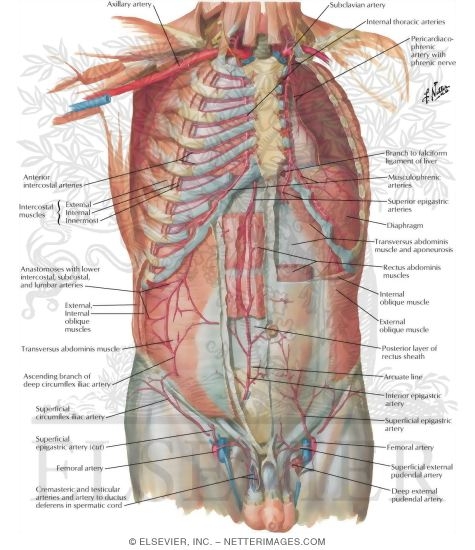
9. Blood Supply of Anterior Abdominal Wall
Arterial Supply
Heart
→ Arch of Aorta
→ Brachiocephalic Trunk → Right Subclavian Artery
→ Left Subclavian Artery
→ Internal Thoracic Artery (from 1st part of Subclavian)
→ Terminal branches:
├── Musculophrenic Artery
└── SUPERIOR EPIGASTRIC ARTERY → supplies ABOVE umbilicus
Heart
→ Arch of Aorta → Aorta
→ Common Iliac Arteries (terminal branches of Aorta)
→ External Iliac Artery + Internal Iliac Artery
→ INFERIOR EPIGASTRIC ARTERY (branch of External Iliac) → below umbilicus
→ External Iliac → becomes FEMORAL ARTERY (after crossing inguinal ligament)
→ SUPERFICIAL EPIGASTRIC ARTERY (branch of Femoral) → below umbilicus
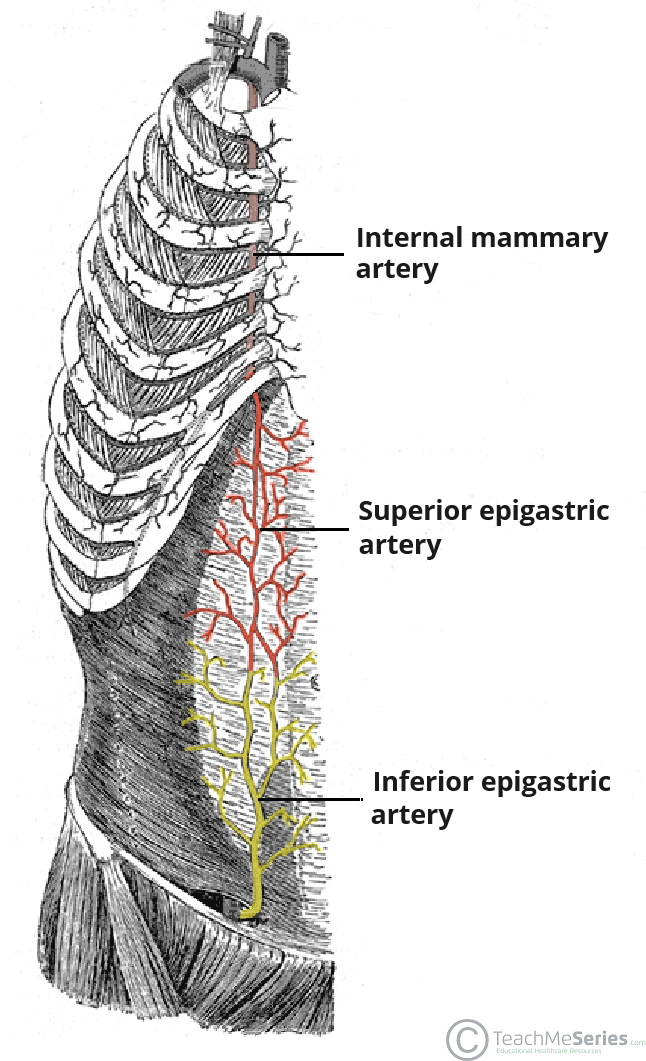
Arterial Supply Summary:
| Region | Arteries |
|---|---|
| Above umbilicus | Superior Epigastric Artery (from Internal Thoracic) + Posterior Intercostal Arteries |
| Below umbilicus | Inferior Epigastric Artery (from External Iliac) + Superficial Epigastric Artery (from Femoral) |
10. Venous Drainage
| Region | Vein | Drains into |
|---|---|---|
| Above umbilicus | Lateral Thoracic Vein | Axillary Vein → Subclavian Vein → SVC → Heart |
| Below umbilicus | Superficial Epigastric Vein | Great Saphenous Vein → Femoral Vein → External Iliac Vein → IVC → Heart |
11. Lymphatic Drainage
| Region | Drains to |
|---|---|
| Above umbilicus | Axillary Lymph Nodes |
| Below umbilicus | Superficial Inguinal Lymph Nodes |
This opposite drainage pattern (axillary vs inguinal) is why the umbilicus is the watershed area - lymph from above and below flows in completely opposite directions.
12. Complete Watershed Area Summary
| Feature | Above Umbilicus | Below Umbilicus |
|---|---|---|
| Arterial supply | Superior Epigastric A. | Inferior + Superficial Epigastric A. |
| Venous drainage | Axillary Vein | Great Saphenous → Femoral Vein |
| Lymph drainage | Axillary nodes | Superficial Inguinal nodes |
13. Quick Recall Diagram (for Exams)
UMBILICUS (Watershed Line)
______________|_______________
| |
ABOVE BELOW
| |
Arterial: Superior Epigastric Inferior Epigastric
Venous: → Axillary Vein → Great Saphenous Vein
Lymph: → Axillary LN → Sup. Inguinal LN
14. What's Coming in the Next Lecture
- Inguinal Ligament
- Inguinal Canal
- Rectus Sheath
- Individual muscle short notes (External Oblique, Internal Oblique, Transversus Abdominis)
Do NOT skip the muscles lecture - it is the foundation for all subsequent abdominal wall topics.
Can you add some more important points for neet pg and inicet with some important diagrams and clinical cases if related and do it quickly
Scarpa fascia Colles fascia urine extravasation clinical significance NEET PG anatomy
anterior abdominal wall superficial fascia NEET PG important questions inicet MCQ
🔥 NEET PG / INI-CET Add-ons: Superficial Fascia of Anterior Abdominal Wall
🩺 CLINICAL CASE 1 - Extravasation of Urine (Most Asked!)
Scenario:
A man falls from a bicycle (straddle injury) and ruptures his bulbous urethra. He presents with swelling of scrotum, penis, and lower abdomen. Where does the urine go and where does it NOT go?
Mechanism:
- Rupture of the bulbous (spongy) urethra is below the perineal membrane
- Urine leaks into the superficial perineal pouch
- It then tracks through fascial planes:
Superficial Perineal Pouch
↓ (via Colles' Fascia)
Scrotum / Dartos fascia
↓
Penis (Buck's fascia outside, deep)
↓
Lower anterior abdominal wall (under Scarpa's fascia)

Where urine DOES spread (NEET PG favourite):
| ✅ Spreads to | ❌ Does NOT spread to |
|---|---|
| Scrotum | Thigh (Scarpa's merges with Fascia Lata at Holden's Line = barrier) |
| Penis | Anal triangle / ischioanal fossa (Colles' + perineal membrane = barrier) |
| Lower anterior abdominal wall (under Scarpa's) | Peritoneal cavity |
| Perineum (superficial perineal pouch) | Gluteal region |

🩺 CLINICAL CASE 2 - Rupture of Membranous Urethra
Scenario:
A patient with pelvic fracture develops rupture of membranous urethra (above the perineal membrane). Where does urine extravasate?
- Rupture is above the perineal membrane → urine stays in the deep perineal pouch / extraperitoneal space
- If perineal membrane is also torn → urine can enter superficial perineal pouch too
- Does NOT enter ischioanal fossa (Colles' fascia + perineal membrane act as a wall)
Exam tip: Straddle injury = bulbous urethra. Pelvic fracture = membranous urethra.
🩺 CLINICAL CASE 3 - Fournier's Gangrene
Scenario:
A diabetic male presents with necrotizing fasciitis of scrotum and perineum spreading to the abdominal wall. Explain the anatomical basis.
- Infection tracks along Dartos fascia → Colles' fascia → Scarpa's fascia (same continuity chain!)
- Spread goes up to Holden's Line but NOT into thighs (Scarpa's fused with Fascia Lata)
- Clinical urgency: Wide debridement of all these fascial planes is required
⚡ HIGH-YIELD NEET PG / INI-CET FACTS
Camper's Fascia:
- Fatty layer (outer)
- Absent in penis (no fat in the penis)
- Present in labia majora in females
- Main contributor to Dartos muscle of scrotum
Scarpa's Fascia:
- Membranous layer (inner)
- Continues as:
- Superficial fascia of penis → Dartos fascia
- Colles' fascia in perineum (main contributor)
- Extends into lower limb up to Holden's Line → fuses with Fascia Lata
- Clinical role: Contains extravasated urine and limits spread
Buck's Fascia:
- Deep fascia of penis (NO deep fascia elsewhere in abdomen)
- Encloses corpora cavernosa and corpus spongiosum
- Rupture of urethra within Buck's fascia → urine stays in penile shaft only
📊 Fascia Comparison Table (Exam Table)
| Fascia | Type | Location | Continuous With |
|---|---|---|---|
| Camper's | Fatty | Outer superficial fascia | Dartos muscle (scrotum) |
| Scarpa's | Membranous | Inner superficial fascia | Colles' fascia (perineum), Fascia Lata (at Holden's line) |
| Colles' | Membranous | Perineum | Scarpa's fascia superiorly, Perineal membrane posteriorly |
| Buck's | Deep fascia | Penis only | No equivalent in abdomen |
| Fascia Lata | Deep fascia | Thigh | Scarpa's fascia at Holden's line |
🧠 Important MCQ-Style One-Liners
| Fact | Answer |
|---|---|
| Superficial fascia has 2 layers below which structure? | Umbilicus |
| Why no deep fascia in abdomen? | Expansion needed (pregnancy, obesity, eating) |
| Scarpa's fascia ends at? | Holden's Line (merges with Fascia Lata) |
| Holden's Line connects? | Both pubic tubercles |
| Main contributor to Dartos muscle? | Camper's fascia |
| Main contributor to Colles' fascia? | Scarpa's fascia |
| Deep fascia present in penis is called? | Buck's fascia |
| Lymph above umbilicus drains to? | Axillary lymph nodes |
| Lymph below umbilicus drains to? | Superficial inguinal lymph nodes |
| Superior epigastric artery is branch of? | Internal thoracic artery (branch of Subclavian) |
| Inferior epigastric artery is branch of? | External iliac artery |
| Superficial epigastric artery is branch of? | Femoral artery |
| Watershed area of abdominal wall is? | Umbilicus |
| Venous drainage above umbilicus goes to? | Axillary vein (via lateral thoracic vein) |
| Venous drainage below umbilicus goes to? | Great Saphenous Vein → Femoral vein |
| Camper's fascia is absent in? | Penis |
| Urine extravasation in straddle injury - barrier preventing spread to thigh? | Scarpa's fascia fusing with Fascia Lata at Holden's Line |
🩸 Blood Supply - Exam Diagram
Anastomosis: Critical viva point!
- Superior Epigastric (from subclavian via internal thoracic) anastomoses with Inferior Epigastric (from external iliac) at/near the umbilicus
- This anastomosis is clinically important - it's a collateral pathway between the subclavian and external iliac systems
- Obstruction of aorta (e.g. coarctation) → blood reroutes through this pathway
🔗 Fascia Continuity Chain Diagram (Draw in Exams)
SCARPA'S FASCIA (abdomen - membranous)
|
↓ crosses inguinal ligament
lower limb → till HOLDEN'S LINE
| |
fuses with FASCIA LATA ↓ also continues
(BARRIER = no |
spread to thigh) ↓
SUPERFICIAL FASCIA of PENIS
|
↓
DARTOS FASCIA (scrotum)
[Main = Camper's; some Scarpa's]
|
↓
COLLES' FASCIA (perineum)
[Main = Scarpa's; some Camper's]
|
↓
Merges with PERINEAL MEMBRANE
|
↓
Ends at UROGENITAL DIAPHRAGM
🚨 Previous Year Question Patterns (NEET PG / INI-CET)
-
Q: After straddle injury, urine extravasates into all EXCEPT? → A: Thigh (Holden's line = barrier)
-
Q: True about Scarpa's fascia? → Membranous layer, merges with Fascia Lata at Holden's line, continues as Colles' fascia
-
Q: Fascia absent in abdomen but present in penis? → Buck's fascia (deep fascia)
-
Q: Camper's fascia is absent in? → Penis
-
Q: Watershed area of anterior abdominal wall? → Umbilicus (different arterial, venous, lymphatic above and below)
-
Q: Superficial inguinal nodes drain which region? → Below umbilicus (skin of lower abdomen, perineum, external genitalia, lower limb)
-
Q: Internal thoracic artery terminates as? → Superior Epigastric + Musculophrenic arteries
Can you add direct images from the lecture
📚 Superficial Fascia of Anterior Abdominal Wall
Complete Notes with Lecture Diagrams
📌 DIAGRAM 1 — Layers of Anterior Abdominal Wall (Outside → Inside)
📌 DIAGRAM 2 — Fascia Continuity Chain
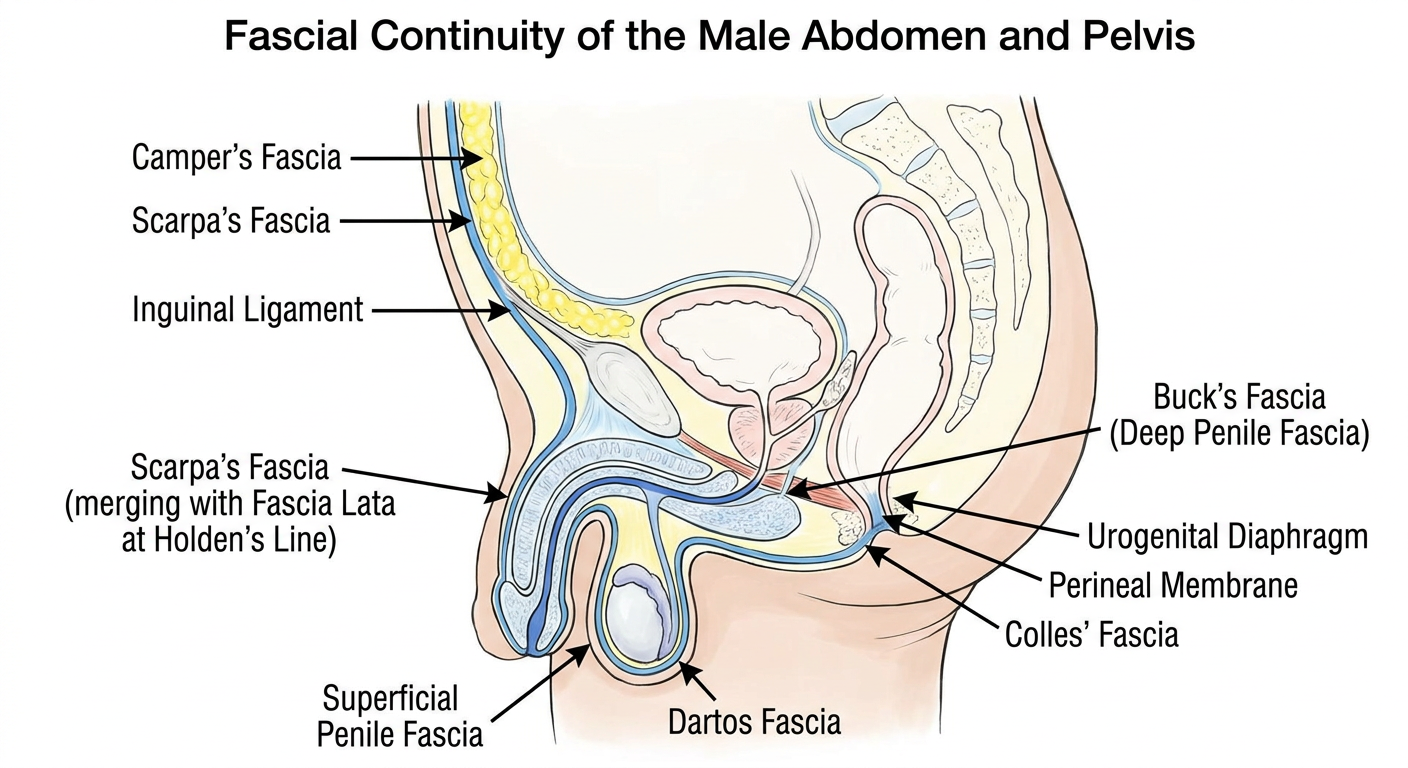
| Step | Structure | Key Note |
|---|---|---|
| 1 | Scarpa's Fascia (abdomen) | Membranous layer |
| 2 | Superficial Fascia of Penis | Scarpa's continues here |
| 3 | Dartos Muscle (scrotum) | Camper's = main contributor |
| 4 | Colles' Fascia (perineum) | Scarpa's = main contributor |
| 5 | Perineal Membrane | Colles' merges here |
| 6 | Urogenital Diaphragm | Terminal point |
📌 DIAGRAM 3 — Arterial Blood Supply
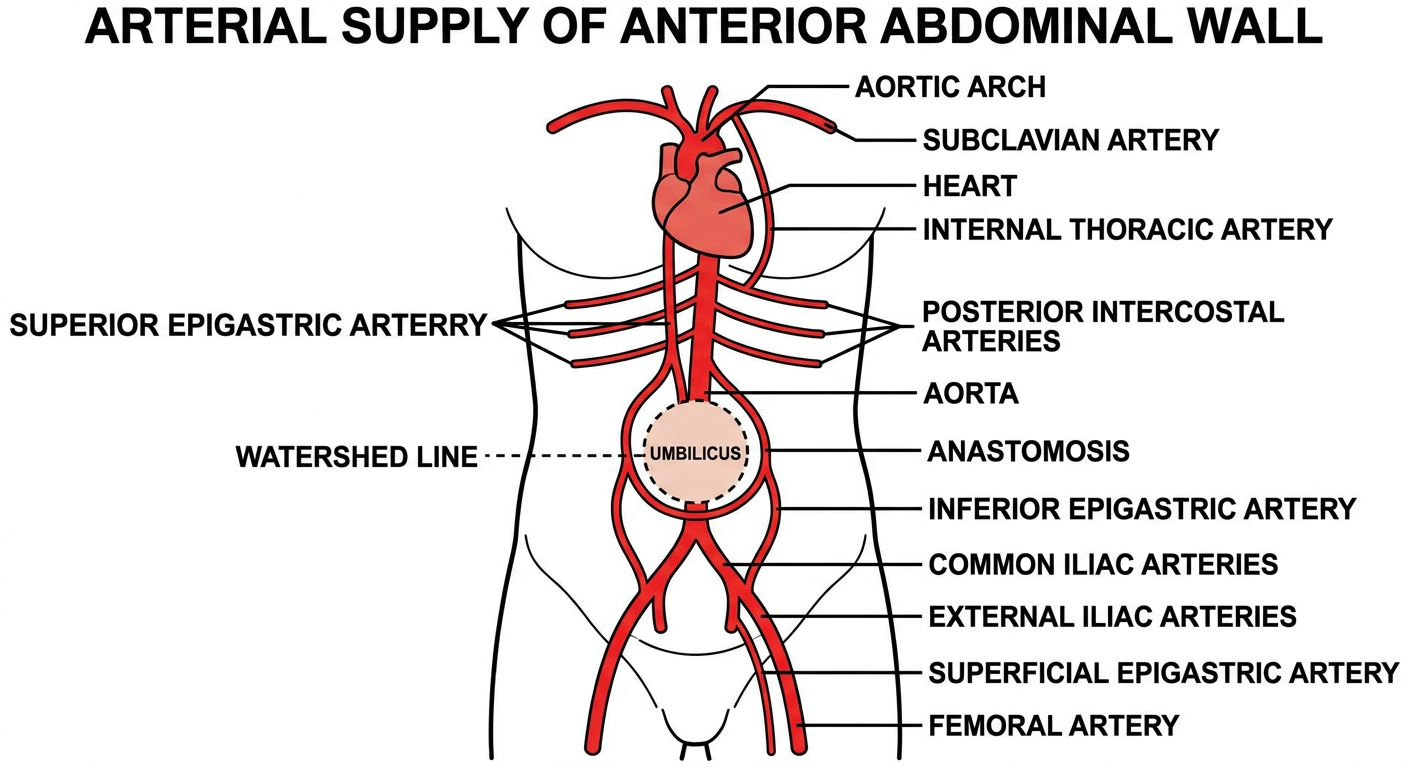
Heart → Aortic Arch → Subclavian A. → Internal Thoracic A.
↓
Superior Epigastric A. (supplies above umbilicus)
+ Musculophrenic A.
Heart → Aorta → Common Iliac → External Iliac A.
↓
Inferior Epigastric A. (supplies below umbilicus)
External Iliac → Femoral A.
↓
Superficial Epigastric A. (also below umbilicus)
⭐ Anastomosis between Superior + Inferior Epigastric arteries occurs near the umbilicus - important collateral pathway!
📌 DIAGRAM 4 — Watershed Area: Venous + Lymphatic Drainage
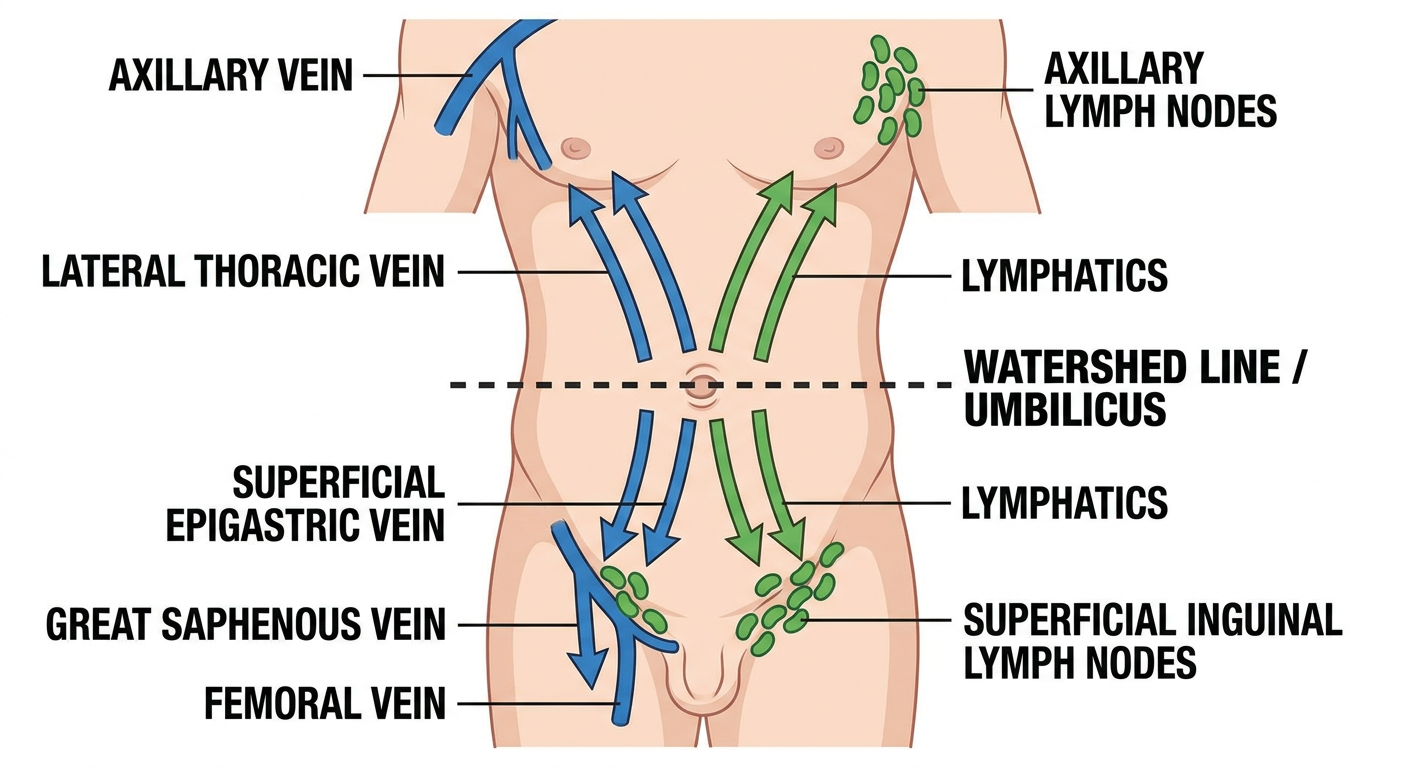
| Above Umbilicus | Below Umbilicus | |
|---|---|---|
| Veins | Lateral Thoracic V. → Axillary Vein | Superficial Epigastric V. → Great Saphenous V. → Femoral V. |
| Lymph | → Axillary Lymph Nodes | → Superficial Inguinal LN |
📌 DIAGRAM 5 — Clinical: Urine Extravasation (Straddle Injury)
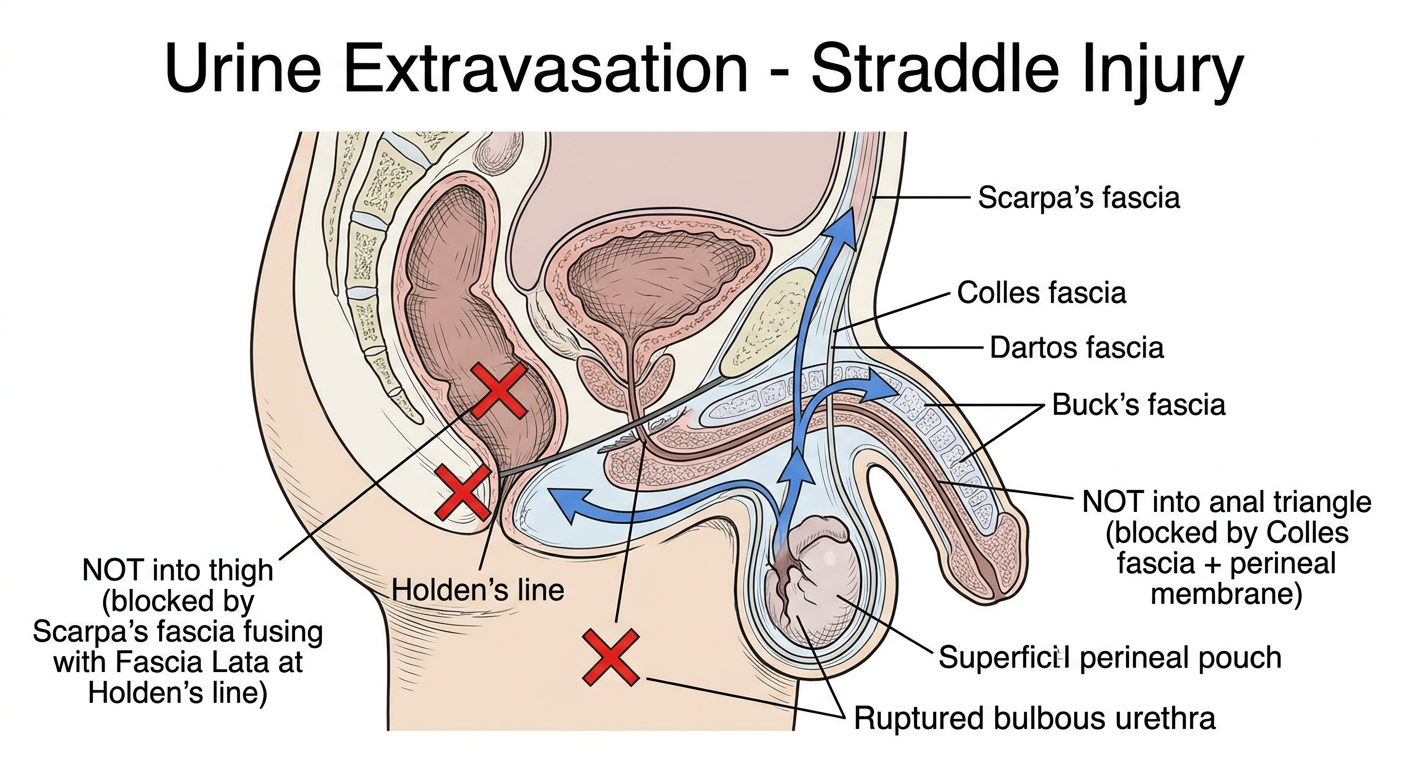
- ✅ Superficial perineal pouch
- ✅ Scrotum (via Dartos fascia)
- ✅ Penis (superficial fascia)
- ✅ Lower anterior abdominal wall (under Scarpa's fascia)
- ❌ Thigh - Scarpa's fused with Fascia Lata at Holden's Line (barrier!)
- ❌ Anal triangle - Colles' fascia + Perineal membrane seal it off
- ❌ Peritoneal cavity
- ❌ Gluteal region
⚡ NEET PG / INI-CET One-Liners (Rapid Revision)
| Question | Answer |
|---|---|
| Fascia absent in abdomen but present in penis? | Buck's fascia |
| Camper's fascia is absent in? | Penis |
| Scarpa's fascia ends at? | Holden's Line (merges with Fascia Lata) |
| Main contributor to Dartos muscle? | Camper's fascia |
| Main contributor to Colles' fascia? | Scarpa's fascia |
| Urine in straddle injury doesn't reach thigh because? | Scarpa's fuses with Fascia Lata at Holden's Line |
| Superior Epigastric A. is branch of? | Internal Thoracic A. (from Subclavian) |
| Inferior Epigastric A. is branch of? | External Iliac A. |
| Watershed area of abdominal wall? | Umbilicus |
| Lymph below umbilicus → ? | Superficial Inguinal LN |
| Lymph above umbilicus → ? | Axillary LN |