Diabetic retinopathy
Reading File
Finding Sources
Searching PubMed
"diabetic retinopathy"[MeSH Terms] AND treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a thorough, textbook-grounded overview of diabetic retinopathy (DR).
Diabetic Retinopathy
Overview
Diabetic retinopathy is the most common cause of new blindness in working-age adults in industrialized countries. It affects approximately 40% of all people with diabetes, rising to 67% of type 2 diabetics 10 years after diagnosis; 10% will develop proliferative disease. Type 1 diabetes carries a higher overall risk. The key insight from major trials (ETDRS, DCCT, UKPDS) is that with effective screening, glycemic control, and timely treatment, the risk of severe visual loss can be reduced to less than 5%.
- Kanski's Clinical Ophthalmology, 10th ed.
Pathogenesis
The primary target is the retinal capillary. Chronic hyperglycemia causes:
- Pericyte loss - pericytes are the supporting cells of retinal capillaries; their loss leads to microaneurysm formation and vascular instability. Pericytes are directly involved in the pathogenesis of diabetic retinopathy.
- Basement membrane thickening - increases vascular permeability
- Endothelial dysfunction - breakdown of the blood-retinal barrier
- Localized retinal ischemia - upregulates VEGF (vascular endothelial growth factor), driving pathological neovascularization
The cascade: capillary leakage → occlusion → ischemia → VEGF release → neovascularization.
- Textbook of Family Medicine, 9e | Histology: A Text and Atlas
Histopathology
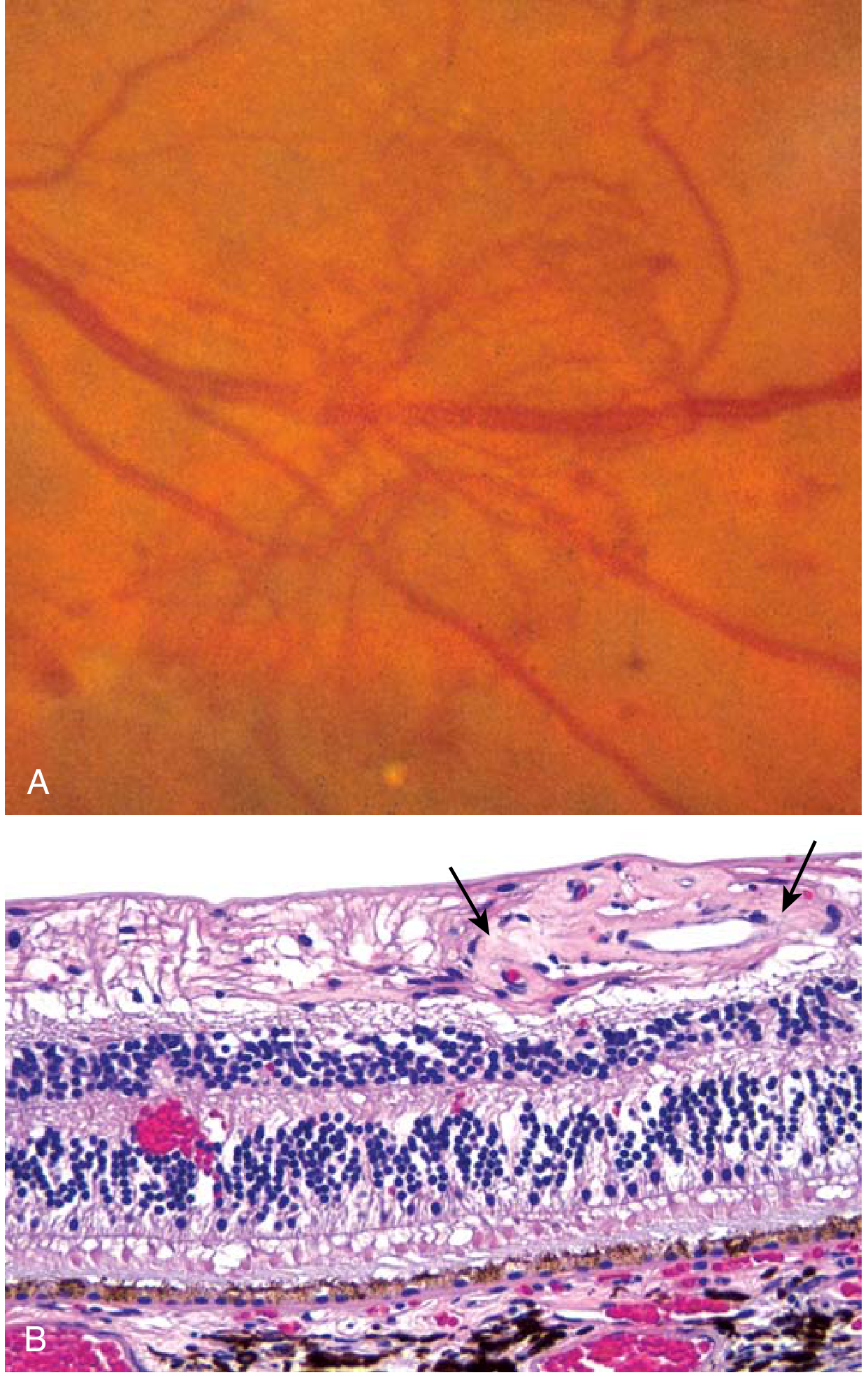
Robbins & Kumar Basic Pathology - neovascular membrane (A) and histological section showing abnormal subretinal vessels with hemorrhage (B).
Classification (Disease Severity Scale)
| Stage | Features |
|---|---|
| No retinopathy | Normal fundus |
| Mild NPDR | Microaneurysms only |
| Moderate NPDR | Microaneurysms + intraretinal hemorrhages, hard exudates, cotton-wool spots (CWS), venous beading |
| Severe NPDR | >20 intraretinal hemorrhages in all 4 quadrants, OR venous beading in ≥2 quadrants, OR prominent IRMA in ≥1 quadrant - in absence of PDR (the "4-2-1" rule) |
| PDR | Neovascularization of disc (NVD), retina (NVE), iris (rubeosis), or angle; +/- vitreous/preretinal hemorrhage; traction retinal detachment |
| Diabetic Macular Edema (DME) | Can occur at any stage; threatens vision when involving or approaching the fovea |
Wills Eye Manual | Goldman-Cecil Medicine
Risk Factors
- Duration of diabetes - most important predictor; DR rare in the first 5 years of type 1 DM
- Poor glycemic control - higher HbA1c = greater risk
- Hypertension - especially in type 2 DM with maculopathy; target <140/80 mmHg
- Nephropathy - severe nephropathy worsens DR; renal transplantation may improve it
- Pregnancy - can cause rapid progression; ~5% of mild DR and ~33% of moderate DR progress to PDR during pregnancy
- Hyperlipidemia, anemia, cataract surgery
- Drugs - pioglitazone is associated with worsening of diabetic macular oedema
- Note: Sudden improvement in glycemic control can transiently worsen retinopathy
- Kanski's Clinical Ophthalmology, 10th ed.
Clinical Features & Symptoms
DR is largely asymptomatic even at the severe proliferative stage. Symptoms arise only when:
- Macular edema impairs central vision
- Vitreous hemorrhage causes floaters or vision loss
- Traction retinal detachment occurs
Other ophthalmic complications of diabetes include:
- Accelerated cataract formation
- Neovascular glaucoma (NVG)
- Ocular motor nerve palsies (CN III or VI)
- Unstable refraction (transient, resolves with glucose control)
- Harrison's Principles of Internal Medicine, 22nd ed.
Diagnosis
- Dilated fundoscopy - first-line; reveals microaneurysms, hemorrhages, exudates
- Fluorescein angiography (FA) - detects capillary non-perfusion, leakage, neovascularization extent
- Optical Coherence Tomography (OCT) - gold standard for detecting and quantifying diabetic macular oedema (DMO)
- Goldman-Cecil Medicine
Differential Diagnosis for NPDR
| Condition | Key distinguishing features |
|---|---|
| CRVO | Disc swelling, dilated/tortuous veins, splinter hemorrhages, usually unilateral |
| BRVO | Hemorrhages along a vein, do not cross horizontal raphe |
| Hypertensive retinopathy | Flame hemorrhages, AV nicking, microaneurysms rare |
| OIS | Midperipheral hemorrhages, no exudates, pain, NVI |
| Radiation retinopathy | History of radiation, microaneurysms rare |
Wills Eye Manual
Treatment
1. Systemic Control (Prevention & Slowing Progression)
- Tight glycemic control (DCCT/UKPDS): prevents development and delays progression; limited effect on advanced disease
- Blood pressure control: especially beneficial in type 2 DM; RAS blockers may be particularly advantageous
- Harrison's / Kanski's
2. Diabetic Macular Oedema (DMO) - First-Line Treatment
Intravitreal anti-VEGF agents have replaced laser as the primary treatment for centre-involving DMO:
- Ranibizumab (DRCR.net Protocol I): more effective than focal/grid laser; benefits sustained over 5 years
- Aflibercept, bevacizumab, ranibizumab: no difference in visual acuity at 5 years for most patients; aflibercept preferred when VA is 6/15 or worse (Protocol T)
- Faricimab (newest): dual inhibitor of VEGF-A and angiopoietin-2; as effective as aflibercept/ranibizumab with up to 16-week dosing intervals after loading phase (YOSEMITE and RHINE studies)
Laser photocoagulation for DMO (focal/modified grid): still useful for off-centre thickening threatening the fovea; reduces risk of moderate visual loss by 50% vs. observation but less effective than anti-VEGF.
Intravitreal steroids (triamcinolone, sustained-release implants): useful in pseudophakic eyes, during pregnancy (when anti-VEGF is contraindicated), or when anti-VEGF fails. Risk of cataract and raised IOP.
- Kanski's Clinical Ophthalmology, 10th ed.
3. Proliferative Diabetic Retinopathy (PDR)
Panretinal Photocoagulation (PRP) - still the mainstay of PDR treatment in most healthcare systems.
PRP is indicated for any of the following "high-risk characteristics":
- NVD ≥ 1/4-1/3 disc area
- Any NVD with preretinal or vitreous hemorrhage (VH)
- NVE ≥ 1/2 disc area with preretinal/VH
- Any NVI or NVA (neovascularization of iris/angle)
Anti-VEGF therapy is an alternative to PRP for PDR; preferred when:
- DME is also present
- VH obscures peripheral retinal view
- Caution: patients lost to follow-up have worse outcomes with anti-VEGF alone vs. PRP
A 2025 meta-analysis (PMID 39128789) confirms anti-VEGF vs. PRP are comparable approaches for PDR, providing updated evidence on this comparison.
4. Vitrectomy
Indicated for:
- Dense, non-clearing vitreous hemorrhage
- Traction retinal detachment involving/progressing within the macula
- Macular epiretinal membrane or vitreomacular traction
- Dense premacular hemorrhage
- Chronic DME unresponsive to other treatments
- Wills Eye Manual
Screening Recommendations
| Diabetes Type | First Exam | Follow-up |
|---|---|---|
| Type 1 | 5 years after diagnosis | Annual dilated fundoscopy |
| Type 2 | At diagnosis (hyperglycemia often pre-dates diagnosis by years) | Annual dilated fundoscopy |
| Pregnancy | Before or early in first trimester | Varies by baseline severity (up to 2-weekly if DR present) |
Textbook of Family Medicine, 9e | Harrison's 22nd ed.
Special Note on Semaglutide (GLP-1 agonists)
A 2025 meta-analysis (PMID 40810985) in JAMA Ophthalmology reported ocular adverse events with semaglutide, including worsening retinopathy - particularly with rapid glycemic lowering. This mirrors the known "early worsening" phenomenon and is relevant when initiating these agents in patients with pre-existing DR.
Prognosis
Prognosis is highly dependent on early detection. With timely screening, glycemic control, and optimized treatment, significant vision loss can be prevented in the majority of patients. Advanced proliferative disease with traction detachment and hemorrhage carries a guarded prognosis.
- Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.