Bacterial growth
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
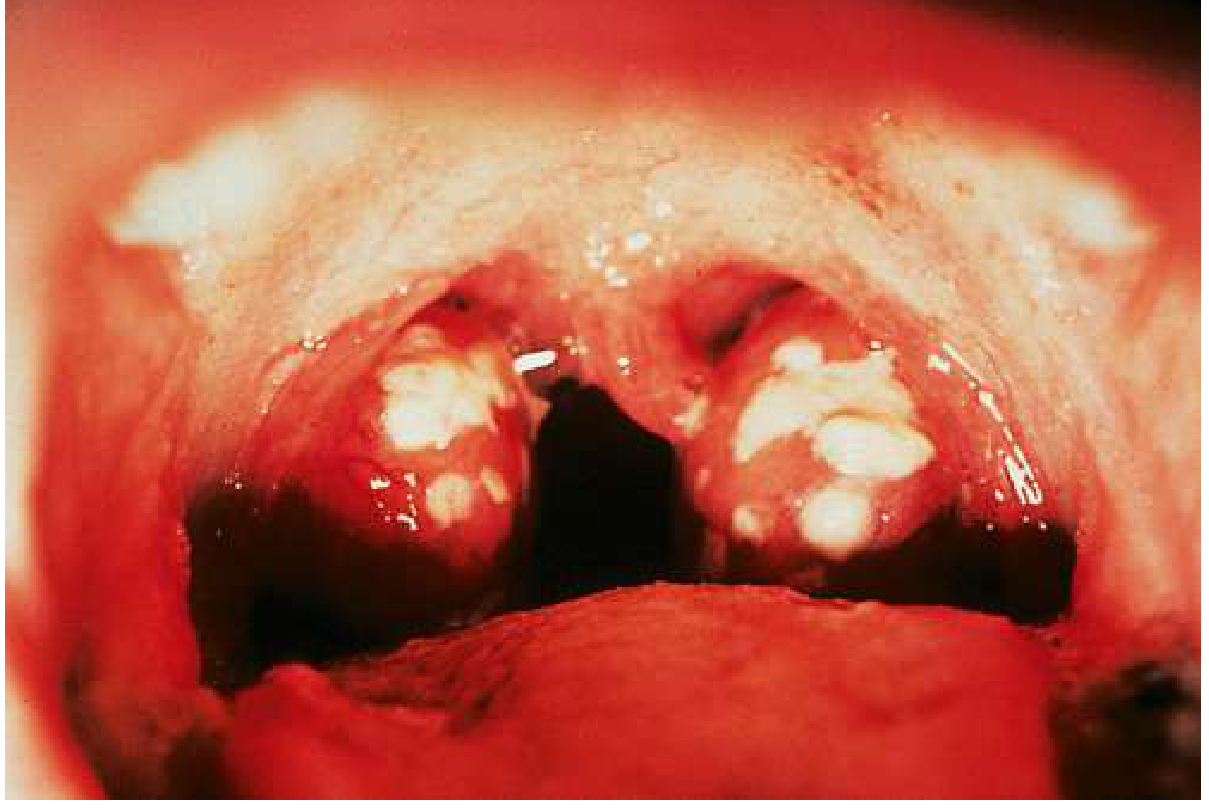
Bacterial pharyngitis Apurva
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
Reading File
I now have comprehensive content. Here is a thorough overview of bacterial pharyngitis for Apurva:
Bacterial Pharyngitis
Overview
Pharyngitis is inflammation of the pharynx and/or tonsils. Bacteria account for roughly 30–40% of pharyngitis in children and 5–15% (up to 23%) in adults. The dominant pathogen is Streptococcus pyogenes (Group A β-hemolytic Streptococcus, GABHS/GAS).
Causative Organisms
| Organism | Notes |
|---|---|
| Group A β-hemolytic Streptococcus (S. pyogenes) | Most common bacterial cause; Lancefield Group A |
| Group C & G streptococci (S. dysgalactiae subsp. equisimilis) | Mirrors GAS clinically; no rheumatic fever risk; penicillin-sensitive |
| Fusobacterium necrophorum | Gram-negative anaerobe; risk of Lemierre's syndrome |
| Neisseria gonorrhoeae | Associated with genital infection; sexually active patients |
| Corynebacterium diphtheriae | Diphtheria; rare in immunized populations |
| Arcanobacterium haemolyticum | Adolescents; may cause a scarlatiniform rash |
GAS Pharyngitis — The Main Focus
Pathogenesis
S. pyogenes is a rapidly growing gram-positive coccus arranged in chains. Virulence is determined by:
- Anti-phagocytic factors: capsule, M protein, C5a peptidase
- Adhesins: M protein, lipoteichoic acid, F protein
- Toxins: streptococcal pyrogenic exotoxins (SPE-A, B, C), streptolysin O & S, streptokinase, DNases
Spread is via respiratory droplets. After colonization, disease occurs before protective anti-M protein antibodies develop.
Clinical Features
After an incubation of 2–5 days, sudden onset of:
- Sore throat, painful swallowing (odynophagia)
- Fever, chills, headache, nausea/vomiting
- Tonsillar swelling (62%), tonsillar exudate (39%), tender anterior cervical lymphadenopathy (76%)
- Uvular edema, myalgias, malaise
- Absent: rhinorrhea, conjunctivitis (these favour viral)
Diagnosis
Modified Centor Score (McIsaac Score)
Step 1 — Calculate score:
| Criterion | Points |
|---|---|
| Temperature > 38°C | +1 |
| Absence of cough | +1 |
| Swollen, tender anterior cervical nodes | +1 |
| Tonsillar swelling or exudate | +1 |
| Age 3–14 years | +1 |
| Age > 44 years | −1 |
Step 2 — Management by score:
| Score | Risk of GAS | Action |
|---|---|---|
| ≤ 0 | 1–2.5% | No testing, no antibiotics |
| 1–2 | 5–17% | Rapid antigen test; treat if positive |
| 3 | 28–35% | Rapid antigen test; treat if positive |
| ≥ 4 | 51–53% | Empirical antibiotics, no testing needed |
Laboratory Tests
- Rapid antigen detection test (RADT): sensitivity ~85–86%, specificity 94–96%
- Throat swab culture: gold standard
- Rapid nucleic acid testing: sensitivity 97.5%, specificity 95% — preferred when available
- If RADT negative in children/adolescents → send culture
- If RADT negative in adults → culture usually not needed (low GAS incidence + low rheumatic fever risk)
- ASO titre: confirms rheumatic fever / post-streptococcal GN
- Anti-DNase B: confirms GN after pharyngitis or pyoderma
Clinical diagnosis alone is only ~75% accurate, even with all classic features — laboratory testing is essential.
Treatment
GAS Pharyngitis
- Penicillin VK 500 mg twice daily × 10 days — first line (GAS has never been resistant to penicillin)
- Benzathine penicillin G 1.2 million units IM single dose — excellent compliance
- Amoxicillin — acceptable alternative; palatable for children
- Penicillin allergy: first-generation cephalosporin or clindamycin
- Adjunct: Single dose of PO/IM dexamethasone in moderate-to-severe cases → faster pain relief, reduced time to resolution (no significant side effects)
Untreated, symptoms resolve in 7–10 days. Antibiotics shorten illness by ~24–48 hours and, critically, prevent rheumatic fever (if started within 10 days). Antibiotics do not prevent post-streptococcal GN.
Non-GAS Bacterial Pharyngitis
- Groups C & G streptococci: penicillin (60% asymptomatic colonisers → treat only symptomatic patients); clindamycin or fluoroquinolones as alternatives
- Diphtheria: diphtheria antitoxin + metronidazole
- Gonococcal: same as genital gonorrhoea treatment
- F. necrophorum: metronidazole + ceftriaxone (or piperacillin-tazobactam) — high macrolide resistance
Complications
Suppurative
| Complication | Notes |
|---|---|
| Peritonsillar abscess | Most common; polymicrobial; F. necrophorum #1 in age 15–24 |
| Retropharyngeal abscess | Especially children |
| Lemierre's syndrome | F. necrophorum; suppurative thrombophlebitis of internal jugular vein; septic emboli |
| Otitis media, sinusitis | Less common |
Non-Suppurative (Immunological — GAS only)
| Complication | Notes |
|---|---|
| Rheumatic fever | Immunologically mediated; delayed 1–5 weeks; PREVENTED by antibiotics |
| Post-streptococcal GN | Associated with pharyngitis AND pyoderma; NOT prevented by antibiotics |
| Streptococcal toxic shock syndrome | Uncommon sequela |
| Scarlet fever | GAS + pyrogenic exotoxin; "sandpaper" rash, strawberry tongue, Pastia's lines; children 2–8 years |
Key Distinctions
| Feature | Bacterial (GAS) | Viral |
|---|---|---|
| Onset | Sudden | Gradual |
| Fever | Often high | Variable |
| Cough | Absent | Present |
| Rhinorrhea | Absent | Present |
| Conjunctivitis | Absent | May be present (adenovirus) |
| Exudate | Common | Less common |
Sources: Tintinalli's Emergency Medicine 9e, Goldman-Cecil Medicine 2 Volume Set, Medical Microbiology 9e
This is a shared conversation. Sign in to Orris to start your own chat.