Hyponatremia evaluation teach me from basics to clinical cases
"hyponatremia"[MeSH Terms] AND "diagnosis"[MeSH Terms]
Hyponatremia: From Basics to Clinical Cases
Part 1 - The Physiology Foundation
Water and Sodium: Why Na+ Reflects Water Balance
Posm = 2 × [Na+] + glucose/18 Normal: 275-290 mOsm/kg
- AVP (vasopressin/ADH) - released by posterior pituitary in response to osmoreceptors in hypothalamus. Promotes free water reabsorption via V2 receptors in the collecting duct.
- Thirst - drives oral free water intake.
"A key concept is that the absolute plasma Na+ concentration tells one nothing about the volume status of a given patient." - Harrison's Principles, 22E
What Happens to Cells?
Part 2 - Definition and Epidemiology
| Term | Definition |
|---|---|
| Hyponatremia | Serum [Na+] < 135 mEq/L |
| Symptomatic threshold | Usually ≤ 125-130 mEq/L (but varies with acuity) |
| Severe hyponatremia | < 120 mEq/L |
| Acute | Duration < 24-48 hours |
| Chronic | Duration > 48 hours |
- Occurs in up to 22% of hospitalized patients (Harrison's 22E)
- In cancer patients, prevalence: 4-47%; associated with 2-5x increased 90-day mortality (Brenner & Rector)
- Most common electrolyte disorder encountered in clinical medicine
Part 3 - Step-by-Step Diagnostic Framework
Step 1 - Is This True Hypotonic Hyponatremia?
| Type | Measured Posm | Cause | Example |
|---|---|---|---|
| Isotonic (pseudohyponatremia) | Normal (275-290) | Lab artifact | Extreme hyperlipidemia, hyperproteinemia (myeloma) |
| Hypertonic | Elevated (>290) | Osmotically active solute | Hyperglycemia, mannitol, sorbitol |
| Hypotonic (true hyponatremia) | Low (<275) | Excess free water relative to Na+ | All causes below |
In pseudohyponatremia (e.g., severe hyperlipidemia), the lab overestimates plasma water because it assumes plasma is 93% water. The measured osmolality is normal even though reported [Na+] is low. - Harrison's 22E
Step 2 - What is the Volume Status? (ECF Assessment)
| Volume Status | Clinical Signs | Pathophysiology |
|---|---|---|
| Hypovolemic | Orthostatic hypotension, tachycardia, dry mucous membranes, skin tenting, ↑BUN/Cr, ↑uric acid | Na+ and water lost; AVP rises to preserve volume |
| Euvolemic | Normal exam - no edema, no signs of depletion | Water retained without Na+ retention |
| Hypervolemic | Peripheral edema, ascites, elevated JVP, S3 gallop | Na+ and water both retained, but water excess > Na+ |
"Clinically detectable hypovolemia, determined most sensitively by careful measurement of orthostatic changes in BP and pulse, usually indicates some degree of solute depletion. Elevations of BUN and uric acid are useful laboratory correlates." - NKF Primer on Kidney Diseases, 8E
Step 3 - Urine Osmolality (Uosm)
| Uosm | Interpretation |
|---|---|
| < 100 mOsm/kg | AVP is suppressed - kidney is making maximally dilute urine. Think: polydipsia (psychogenic or beer potomania), exercise-associated hyponatremia |
| 100-300 mOsm/kg | Partially diluted urine - mixed picture (partial AVP, or solute depletion limiting water excretion) |
| > 300 mOsm/kg | AVP is active - kidney is concentrating. Most clinical hyponatremia |
| > 400 mOsm/kg | AVP playing dominant role |
"Urine osmolality > 100 mOsm/L H2O with the exception of patients with psychogenic polydipsia, which drives down urine osmolality below 100." - Tintinalli's EM
Uosm ≈ (hundredths + thousandths digits of π) × 35 Example: π = 1.015 → 15 × 35 = 525 mOsm/L
Step 4 - Urine Sodium (UNa)
| Volume Status | UNa | Interpretation |
|---|---|---|
| Hypovolemic | < 20-30 mEq/L | Extra-renal Na+ loss (GI, skin) - kidneys appropriately conserving Na+ |
| Hypovolemic | > 20-30 mEq/L | Renal Na+ wasting (diuretics, adrenal insufficiency, salt-losing nephropathy, CSW) |
| Euvolemic (SIADH) | > 30 mEq/L | Inappropriately high despite low plasma [Na+] |
| Hypervolemic (CHF, cirrhosis, nephrotic) | < 10 mEq/L | Kidneys avidly retaining Na+ due to perceived underfilling |
| Hypervolemic (renal failure) | > 20 mEq/L | Kidneys cannot retain Na+ |
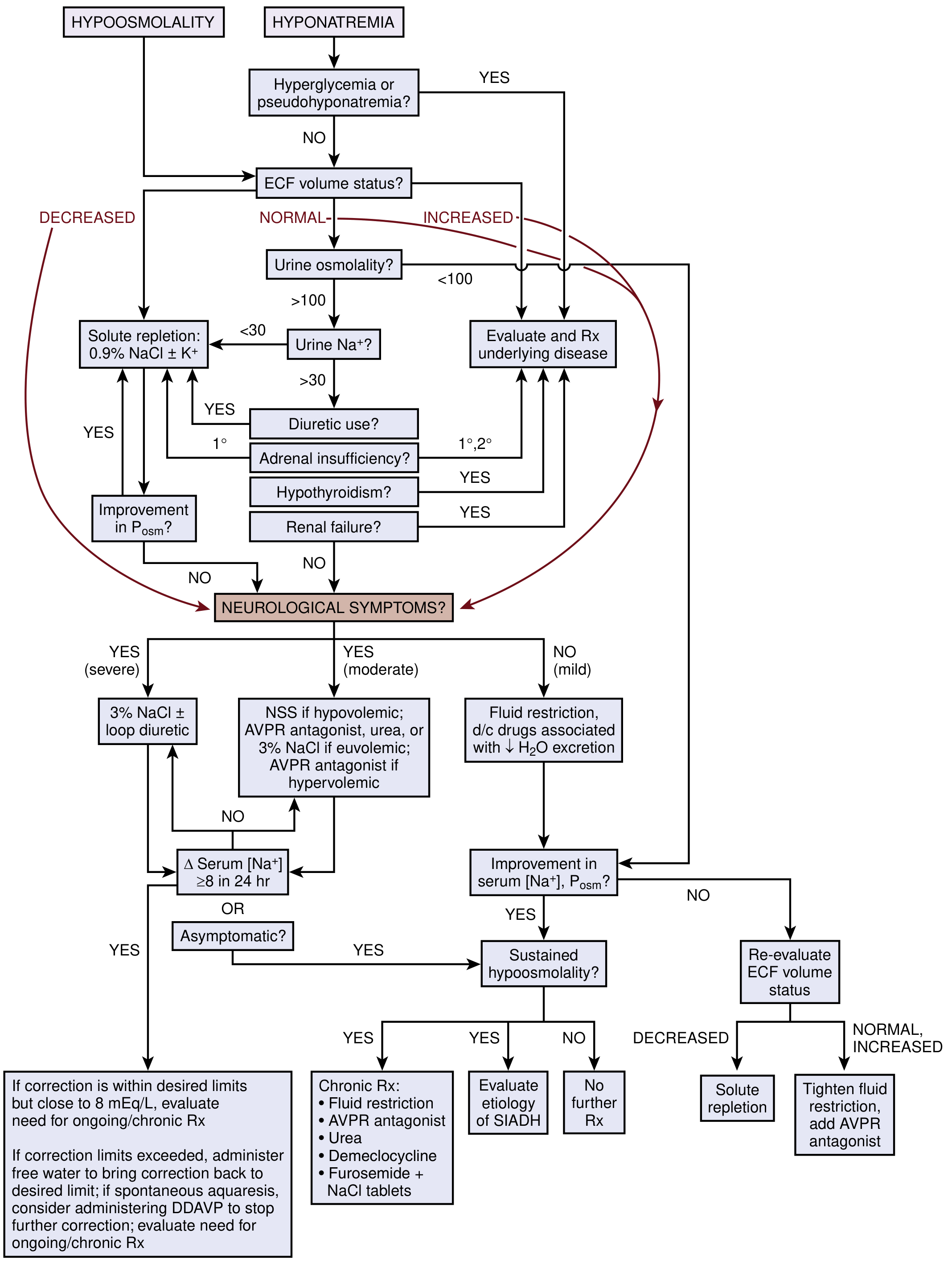
The Master Diagnostic Algorithm
Part 4 - Causes by Volume Category
A. Hypovolemic Hyponatremia
- GI losses: vomiting, diarrhea, NG drainage
- Insensible losses: sweating (especially cystic fibrosis with salty sweat), burns
- Third spacing: pancreatitis, bowel obstruction
- Thiazide diuretics (most common - impairs NaCl cotransporter in DCT)
- Adrenal insufficiency (primary Addison's: ↓aldosterone → Na+ wasting; also hyperkalemia + hyponatremia + hypotension is a classic triad)
- Salt-losing nephropathies: reflux nephropathy, interstitial nephritis, medullary cystic disease, post-ATN recovery
- Cerebral salt wasting (CSW) - seen in intracranial pathology (SAH, TBI); must distinguish from SIADH because treatment differs (CSW requires sodium + volume replacement, not fluid restriction)
B. Euvolemic Hyponatremia
SIADH - Syndrome of Inappropriate Antidiuretic Hormone
| Criterion | Value |
|---|---|
| Hypotonic hyponatremia | Posm < 275 mOsm/kg |
| Inappropriately elevated urine osmolality | Usually > 200 mOsm/kg |
| Elevated urine Na+ | Typically > 20 mEq/L |
| Clinical euvolemia | No signs of volume depletion or overload |
| Normal adrenal, renal, cardiac, hepatic, thyroid function | Rule out other causes |
| Category | Examples |
|---|---|
| CNS disorders | Meningitis, encephalitis, brain abscess, SAH, subdural hematoma, stroke, trauma, psychosis |
| Pulmonary disorders | Pneumonia, TB, lung abscess, empyema, acute respiratory failure, positive-pressure ventilation |
| Malignancy (ectopic AVP) | Small cell lung cancer (most common - 10-15% of SCLC), pancreatic, duodenal, bladder, prostate, lymphoma |
| Medications | SSRIs/SNRIs, thiazides, carbamazepine, oxcarbazepine, cyclophosphamide, vincristine, cisplatin, NSAIDs, opioids, amiodarone, desmopressin, haloperidol, phenothiazines |
| Miscellaneous | Major surgery, pain, nausea, HIV, hypothyroidism (also separate mechanism) |
- Ratio > 1: Aggressively restrict fluids to < 500 mL/day
- Ratio ~1: Restrict to 500-700 mL/day
- Ratio < 1: Restrict to < 1 L/day This predicts responsiveness to fluid restriction.
Other Euvolemic Causes:
- Hypothyroidism: Reduced cardiac output → reduced GFR + non-osmotic AVP release. TSH is essential in the workup.
- Secondary adrenal insufficiency (pituitary/hypothalamic): Unlike primary Addison's (which is hypovolemic with hyperkalemia), secondary AI is euvolemic and normokalemic - aldosterone is intact, only cortisol is deficient. Cosyntropin stimulation test differentiates.
- Beer potomania / low solute intake: Extremely low solute intake limits the kidneys' ability to excrete free water regardless of AVP status. Uosm is typically very low (100-200s), UNa < 20. High risk of ODS upon treatment due to associated hypokalemia + malnutrition.
- Psychogenic polydipsia: Massive water intake overwhelms renal excretion. Uosm < 100 (maximally dilute - AVP is suppressed). Common in schizophrenia.
- Exercise-associated hyponatremia (EAH): Acute, from excessive hypotonic fluid intake during endurance events, combined in ~44% of cases with SIADH. Weight gain during race is the key clue. Uosm < 100 in pure water intoxication. Dangerous because acute onset causes severe symptoms.
C. Hypervolemic Hyponatremia
| Cause | UNa | Key Features |
|---|---|---|
| Congestive heart failure | < 10 mEq/L | ↑JVP, S3, dyspnea, BNP elevated |
| Cirrhosis | < 10 mEq/L | Ascites, spider angiomata, asterixis, ↑bilirubin |
| Nephrotic syndrome | < 10 mEq/L | Massive proteinuria, edema, hypoalbuminemia |
| Advanced renal failure | > 20 mEq/L | ↑Cr, ↑K+, uremic features |
Part 5 - Symptoms and Severity
| Severity | Symptoms |
|---|---|
| Mild (130-135) | Often asymptomatic; nausea, malaise |
| Moderate (125-130) | Headache, lethargy, confusion, muscle cramps |
| Severe (<125, especially acute) | Seizures, obtundation, respiratory arrest, brain herniation, coma, death |
- Acute hyponatremia (< 48 h) - brain hasn't adapted, symptoms occur at higher [Na+] levels, risk of herniation
- Chronic hyponatremia (> 48 h) - brain has adapted by losing organic osmolytes, symptoms may be minimal even at [Na+] 115-120
Part 6 - Treatment
Three Governing Principles (Harrison's 22E)
- Symptom severity determines urgency
- Overcorrection risk - ODS in chronic hyponatremia
- Monitor frequently - response to treatment is unpredictable
Treatment by Category
Symptomatic / Acute / Severe
| Step | Action |
|---|---|
| 1 | Give 100-150 mL of 3% NaCl IV over 15-20 minutes |
| 2 | Check serum [Na+] after each infusion |
| 3 | Stop when symptoms improve OR [Na+] rises 4-6 mEq/L |
| 4 | May repeat up to 3 doses (total 450 mL) |
| 5 | Limit total correction to ≤ 8-12 mEq/L in first 24 h, ≤ 18 mEq/L in 48 h |
Chronic Mild-Moderate Hyponatremia - By Cause
| Cause | Treatment |
|---|---|
| Hypovolemic | Isotonic normal saline (0.9% NaCl) - repletes volume → AVP suppresses → water diuresis corrects [Na+]. Correct K+ as needed. |
| SIADH / euvolemic | Fluid restriction (first-line); oral Na+ supplementation; urea; demeclocycline; vaptans (tolvaptan, conivaptan) |
| CHF / hypervolemic | Treat underlying cause (ACE-I, diuretics, optimize cardiac output); fluid restriction; vaptans for refractory cases |
| Hypothyroidism | Thyroid hormone replacement |
| Adrenal insufficiency | Corticosteroid replacement |
| Beer potomania / low solute | IV saline + resume normal diet; high-risk for ODS |
| EAH (acute) | Hypertonic saline urgently if symptomatic; fluid restriction; stop hypotonic fluid intake |
- U/P ratio > 1 → restrict to < 500 mL/day
- U/P ratio ~1 → 500-700 mL/day
- U/P ratio < 1 → < 1 L/day
Part 7 - Osmotic Demyelination Syndrome (ODS)
Mechanism
Risk Factors for ODS
- Serum [Na+] < 120 mEq/L
- Duration > 48 hours (chronic)
- Hypokalemia
- Alcoholism, cirrhosis
- Malnutrition
- Beer potomania (extremely high risk)
- Use of vaptans
Correction Limits
| Time Period | Max Safe Correction |
|---|---|
| First 24 hours | ≤ 8-10 mEq/L (some guidelines allow up to 12 for acute) |
| First 48 hours | ≤ 18 mEq/L |
Clinical Presentation of ODS
- Dysarthria, dysphagia
- Behavioral changes, lethargy
- Paraparesis or quadriparesis
- Locked-in syndrome (in severe cases)
- Seizures, coma
If Overcorrection Occurs
- Administer 5% dextrose in water at 3 mL/kg/h
- Add desmopressin (DDAVP) to stop further free water excretion
- Loop diuretics
- Goal: bring [Na+] back down toward the safe correction target
Part 8 - Clinical Cases
Case 1 - The Dehydrated Vomiter
- Step 1: Posm 258 - true hypotonic hyponatremia ✓
- Step 2: Clearly hypovolemic (orthostatics, tachycardia, dry MM, ↑BUN/Cr, ↑uric acid presumed)
- Step 3: Uosm 680 - AVP is very active (kidney concentrating urine to preserve volume)
- Step 4: UNa 8 - extra-renal Na+ loss (kidneys are avid for Na+ - GI losses)
Case 2 - The SIADH Patient
- Step 1: Posm 242 - true hypotonic hyponatremia ✓
- Step 2: Euvolemic - no edema, no depletion
- Step 3: Uosm 520 - AVP is active despite hyponatremia (inappropriate)
- Step 4: UNa 65 - very high (kidney not retaining Na+)
- Serum uric acid < 4 → SIADH physiology
- Clinical context: SCLC producing ectopic AVP
Case 3 - The Marathon Runner
- Uosm < 100 → AVP is SUPPRESSED → maximally dilute urine
- This is acute water intoxication, not chronic hyponatremia
- UNa 12 reflects some sodium conservation but is less useful here
- The low Uosm with acute onset during endurance event = Exercise-Associated Hyponatremia (EAH)
- 150 mL of 3% NaCl IV over 20 minutes
- Recheck [Na+], may repeat up to 3 times
- Stop when seizures resolve or [Na+] rises 4-6 mEq/L
- Since this is acute (< 24 hours), the risk of ODS is low - the brain has not had time to adapt by losing osmolytes
Case 4 - Thiazide Mimic of SIADH
- Looks exactly like SIADH - euvolemic, high UNa, high Uosm
- But: started thiazide 3 weeks ago, hypokalemia (K+ 2.8)
- Thiazide mechanism: blocks NaCl cotransporter in DCT (diluting segment) → impairs water excretion + volume depletion → AVP rises + polydipsia
Case 5 - Adrenal Crisis
- Hypovolemic + hyperkalemia + hyponatremia + hypotension → classic triad
- Hyperpigmentation in HIV patient → think primary adrenal insufficiency (Addison's disease - HIV can cause adrenal infiltration by CMV, MAI, or direct HIV)
- High UNa despite hypovolemia → kidneys cannot retain Na+ (no aldosterone)
Part 9 - High-Yield Summary Table
| Condition | Volume | Uosm | UNa | Key Clue | Treatment |
|---|---|---|---|---|---|
| GI losses | ↓ | High | < 20 | Orthostasis, vomiting/diarrhea | 0.9% NS |
| Thiazide | ↓ or euvolemic | High | > 20 | Hypokalemia, recent thiazide | Stop drug, correct K+ |
| Adrenal insufficiency (primary) | ↓ | High | >> 20 | Hyperkalemia, hyperpigmentation | Hydrocortisone + NS |
| CSW | ↓ | High | > 20 | CNS pathology (SAH, TBI) | Na+ + volume |
| SIADH | Euvolemic | > 200 | > 30 | Exclusion diagnosis | Fluid restriction ± urea ± vaptan |
| Hypothyroidism | Euvolemic | Variable | Variable | Fatigue, myxedema, ↑TSH | T4 replacement |
| Secondary AI | Euvolemic | High | > 20 | Normokalemic, pituitary disease | Cortisol |
| Beer potomania | Euvolemic | < 100-200 | < 20 | Alcoholism, low solute diet | NS + diet; high ODS risk |
| Psychogenic polydipsia | Euvolemic | < 100 | Low | Psychiatric hx, schizophrenia | Fluid restriction, treat psych |
| EAH | Euvolemic | < 100 | Low | Post-endurance event, weight gain | Hypertonic saline if severe |
| CHF | ↑ | High | < 10 | Edema, ↑JVP, ↑BNP | Treat CHF, fluid restrict, vaptan |
| Cirrhosis | ↑ | High | < 10 | Ascites, spider angiomata | Treat liver disease, fluid restrict |
| Renal failure | ↑ | Variable | > 20 | ↑Cr, ↑K+ | Dialysis |
Part 10 - Recent Evidence Updates (2024-2026)
- Tolvaptan (PMID 40288608, 2025): Systematic review/meta-analysis confirmed low-dose tolvaptan is effective and safe for SIADH-associated hyponatremia, with comparable efficacy to standard doses but fewer adverse effects.
- Urea (PMID 39362395, 2025): Meta-analysis of urea vs. other treatments for SIADH hyponatremia confirmed urea is effective, safe, inexpensive, and under-utilized. Particularly useful when fluid restriction is poorly tolerated.
- Point-of-care ultrasound (PMID 41528666, 2026): Systematic review supports POCUS as a complementary tool in hyponatremia evaluation for assessing ECF volume status (IVC collapsibility, lung B-lines for CHF, ascites for cirrhosis) - particularly valuable when clinical volume assessment is uncertain.
Quick Reference: The 4-Question Framework
1. Is Posm low? (True hypotonic hyponatremia?)
↓
2. What is the ECF volume? (Hypo / Eu / Hypervolemic?)
↓
3. What is Uosm? (Is AVP active?)
↓
4. What is UNa? (Renal vs. extra-renal? Appropriate vs. inappropriate?)
Convert above data into short presentation
ls /home/daytona/workspace/ 2>/dev/null || echo "workspace empty"
~/hyponatremia-ppt/build.js
const pptxgen = require("pptxgenjs");
const pres = new pptxgen();
pres.layout = "LAYOUT_16x9";
pres.title = "Hyponatremia: Evaluation & Management";
pres.author = "Orris Medical Education";
// ─── PALETTE ───────────────────────────────────────────────────────────────
const C = {
navy: "0A2342", // dominant bg
teal: "0D7377", // accent / header bars
aqua: "14BDAC", // highlight / accent
white: "FFFFFF",
offWhite:"F0F4F8",
yellow: "F5C518", // callout
red: "E63946", // danger / ODS
gray: "94A3B8",
lightBg: "EBF4F6", // light slide bg
darkText:"1E293B",
};
// ─── HELPERS ────────────────────────────────────────────────────────────────
function darkSlide(slide) {
slide.addShape(pres.ShapeType.rect, { x:0, y:0, w:"100%", h:"100%", fill:{color:C.navy}, line:{color:C.navy} });
}
function lightSlide(slide) {
slide.addShape(pres.ShapeType.rect, { x:0, y:0, w:"100%", h:"100%", fill:{color:C.offWhite}, line:{color:C.offWhite} });
}
function tealBar(slide, y=0, h=1.1) {
slide.addShape(pres.ShapeType.rect, { x:0, y:y, w:"100%", h:h, fill:{color:C.teal}, line:{color:C.teal} });
}
function accentLine(slide, y) {
slide.addShape(pres.ShapeType.rect, { x:0.4, y:y, w:1.2, h:0.07, fill:{color:C.aqua}, line:{color:C.aqua} });
}
function sectionTag(slide, label) {
slide.addShape(pres.ShapeType.rect, { x:0, y:0, w:2.6, h:0.38, fill:{color:C.aqua}, line:{color:C.aqua} });
slide.addText(label, { x:0, y:0, w:2.6, h:0.38, fontSize:11, bold:true, color:C.navy, align:"center", valign:"middle", margin:0 });
}
function slideTitle(slide, title, x=0.4, y=0.55, w=9.2, color=C.white) {
slide.addText(title, { x, y, w, h:0.65, fontSize:26, bold:true, color, fontFace:"Calibri", valign:"middle" });
}
function bodyText(slide, items, x, y, w, h, color=C.darkText, size=14) {
const arr = items.map((item, i) => ({
text: item,
options: { bullet: true, breakLine: i < items.length - 1, fontSize: size, color, fontFace:"Calibri" }
}));
slide.addText(arr, { x, y, w, h, valign:"top" });
}
// ══════════════════════════════════════════════════════════════════════════════
// SLIDE 1 — TITLE
// ══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
darkSlide(s);
// teal left accent strip
s.addShape(pres.ShapeType.rect, { x:0, y:0, w:0.18, h:"100%", fill:{color:C.aqua}, line:{color:C.aqua} });
// big aqua circle decoration
s.addShape(pres.ShapeType.ellipse, { x:7.5, y:-1.2, w:4.5, h:4.5, fill:{color:C.teal, transparency:75}, line:{color:C.teal, transparency:75} });
s.addShape(pres.ShapeType.ellipse, { x:8.2, y:2.8, w:2.8, h:2.8, fill:{color:C.aqua, transparency:85}, line:{color:C.aqua, transparency:85} });
s.addText("HYPONATREMIA", { x:0.5, y:1.2, w:9, h:0.7, fontSize:44, bold:true, color:C.aqua, charSpacing:6, fontFace:"Calibri" });
s.addText("Evaluation & Management", { x:0.5, y:2.0, w:9, h:0.55, fontSize:26, color:C.white, fontFace:"Calibri" });
s.addText("From Basics to Clinical Cases", { x:0.5, y:2.65, w:9, h:0.4, fontSize:16, color:C.gray, fontFace:"Calibri", italic:true });
accentLine(s, 3.2);
s.addText("Based on Harrison's 22E · Brenner & Rector · Tintinalli's EM · NKF Primer", {
x:0.5, y:4.8, w:9, h:0.35, fontSize:11, color:C.gray, fontFace:"Calibri", italic:true
});
}
// ══════════════════════════════════════════════════════════════════════════════
// SLIDE 2 — DEFINITION & EPIDEMIOLOGY
// ══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
lightSlide(s);
tealBar(s, 0, 1.05);
sectionTag(s, "BASICS");
slideTitle(s, "Definition & Epidemiology", 0.4, 0.2, 9.2, C.white);
// 4 stat boxes
const boxes = [
{ label:"Definition", val:"Na⁺ < 135 mEq/L", sub:"Symptoms rare until ≤125 mEq/L" },
{ label:"Prevalence", val:"Up to 22%", sub:"Of all hospitalized patients" },
{ label:"Acute", val:"< 48 hours", sub:"Brain not yet adapted — high risk" },
{ label:"Chronic", val:"> 48 hours", sub:"Brain adapted — symptoms milder" },
];
boxes.forEach((b, i) => {
const x = 0.3 + i * 2.38;
s.addShape(pres.ShapeType.rect, { x, y:1.25, w:2.15, h:3.6, fill:{color:C.white}, line:{color:C.teal, pt:2},
shadow:{type:"outer", color:"000000", blur:8, offset:2, angle:135, opacity:0.10} });
s.addShape(pres.ShapeType.rect, { x, y:1.25, w:2.15, h:0.45, fill:{color:C.teal}, line:{color:C.teal} });
s.addText(b.label, { x, y:1.25, w:2.15, h:0.45, fontSize:11, bold:true, color:C.white, align:"center", valign:"middle", margin:0 });
s.addText(b.val, { x, y:1.78, w:2.15, h:1.1, fontSize:17, bold:true, color:C.navy, align:"center", valign:"middle", fontFace:"Calibri" });
s.addText(b.sub, { x, y:2.88, w:2.15, h:1.5, fontSize:11, color:C.darkText, align:"center", valign:"top", fontFace:"Calibri", wrap:true });
});
// severity strip
s.addShape(pres.ShapeType.rect, { x:0.3, y:5.0, w:9.4, h:0.4, fill:{color:C.navy}, line:{color:C.navy} });
s.addText("Severity: Mild 130–135 | Moderate 125–130 | Severe < 125 mEq/L", {
x:0.3, y:5.0, w:9.4, h:0.4, fontSize:12, bold:true, color:C.aqua, align:"center", valign:"middle", margin:0
});
}
// ══════════════════════════════════════════════════════════════════════════════
// SLIDE 3 — PHYSIOLOGY
// ══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
lightSlide(s);
tealBar(s, 0, 1.05);
sectionTag(s, "PHYSIOLOGY");
slideTitle(s, "Why Does Hyponatremia Happen?", 0.4, 0.2, 9.2, C.white);
// two columns
// Left: physiology
s.addShape(pres.ShapeType.rect, { x:0.3, y:1.2, w:4.55, h:4.1, fill:{color:C.white}, line:{color:C.teal, pt:1.5} });
s.addShape(pres.ShapeType.rect, { x:0.3, y:1.2, w:4.55, h:0.42, fill:{color:C.navy}, line:{color:C.navy} });
s.addText("Key Concept: Na⁺ Reflects Water Balance", { x:0.3, y:1.2, w:4.55, h:0.42, fontSize:11.5, bold:true, color:C.aqua, align:"center", valign:"middle", margin:0 });
bodyText(s, [
"Serum [Na⁺] = Total Body Na⁺ / Total Body Water",
"Hyponatremia = excess water relative to sodium",
"AVP (vasopressin) is the main regulator — promotes renal free-water reabsorption",
"Most cases = excess AVP + free water intake",
"Volume status modulates AVP: hypovolemia → ↑AVP even at normal osmolality",
], 0.5, 1.75, 4.2, 3.4, C.darkText, 12.5);
// Right: defense mechanisms
s.addShape(pres.ShapeType.rect, { x:5.15, y:1.2, w:4.55, h:4.1, fill:{color:C.white}, line:{color:C.aqua, pt:1.5} });
s.addShape(pres.ShapeType.rect, { x:5.15, y:1.2, w:4.55, h:0.42, fill:{color:C.aqua}, line:{color:C.aqua} });
s.addText("Two Defense Mechanisms", { x:5.15, y:1.2, w:4.55, h:0.42, fontSize:11.5, bold:true, color:C.navy, align:"center", valign:"middle", margin:0 });
bodyText(s, [
"① AVP release by posterior pituitary → water reabsorption",
"② Thirst → drives oral water intake",
"Defect in either + free water intake → hyponatremia",
"Brain cell swelling → neurological symptoms",
"Chronic: brain adapts by losing organic osmolytes (taurine, glutamate) → less symptomatic",
], 5.35, 1.75, 4.2, 3.4, C.darkText, 12.5);
// formula bar
s.addShape(pres.ShapeType.rect, { x:0.3, y:5.35, w:9.4, h:0.42, fill:{color:C.yellow, transparency:15}, line:{color:C.yellow} });
s.addText("Effective Osmolality = 2×[Na⁺] + Glucose/18 | Normal: 275–290 mOsm/kg", {
x:0.3, y:5.35, w:9.4, h:0.42, fontSize:13, bold:true, color:C.navy, align:"center", valign:"middle", margin:0
});
}
// ══════════════════════════════════════════════════════════════════════════════
// SLIDE 4 — 4-STEP DIAGNOSTIC FRAMEWORK
// ══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
darkSlide(s);
sectionTag(s, "DIAGNOSIS");
slideTitle(s, "The 4-Step Diagnostic Framework", 0.4, 0.2, 9.2, C.aqua);
accentLine(s, 1.0);
const steps = [
{ num:"1", title:"Serum Osmolality", body:"Is this TRUE hypotonic hyponatremia?\nRule out pseudohyponatremia (lipemia, paraprotein)\nand hypertonic (hyperglycemia, mannitol)", color:C.teal },
{ num:"2", title:"ECF Volume Status", body:"Hypovolemic / Euvolemic / Hypervolemic\nMost important clinical step\nOrthostatics, JVP, edema, BUN/Cr, uric acid", color:"1565C0" },
{ num:"3", title:"Urine Osmolality", body:"Is AVP active?\n< 100 = AVP suppressed (polydipsia, EAH)\n> 300 = AVP active (most clinical hyponatremia)", color:"6A0572" },
{ num:"4", title:"Urine Sodium", body:"Renal vs. extra-renal? Appropriate vs. not?\n< 20: extra-renal loss or Na⁺-avid state\n> 30: renal wasting or SIADH", color:"B5451B" },
];
steps.forEach((st, i) => {
const x = 0.25 + i * 2.42;
s.addShape(pres.ShapeType.rect, { x, y:1.18, w:2.2, h:4.15, fill:{color:st.color}, line:{color:st.color} });
s.addShape(pres.ShapeType.ellipse, { x: x+0.7, y:1.25, w:0.8, h:0.8, fill:{color:C.white}, line:{color:C.white} });
s.addText(st.num, { x: x+0.7, y:1.25, w:0.8, h:0.8, fontSize:20, bold:true, color:st.color, align:"center", valign:"middle", margin:0 });
s.addText("STEP "+st.num, { x, y:2.18, w:2.2, h:0.35, fontSize:10, bold:true, color:C.white, align:"center", valign:"middle", margin:0, charSpacing:3 });
s.addText(st.title, { x, y:2.55, w:2.2, h:0.5, fontSize:13.5, bold:true, color:C.yellow, align:"center", valign:"middle", fontFace:"Calibri" });
s.addText(st.body, { x:x+0.1, y:3.1, w:2.0, h:2.1, fontSize:10.5, color:C.white, fontFace:"Calibri", wrap:true, valign:"top" });
});
s.addText("Combine all 4 steps with clinical context → diagnosis is almost always apparent", {
x:0.4, y:5.4, w:9.2, h:0.35, fontSize:12, italic:true, color:C.gray, align:"center"
});
}
// ══════════════════════════════════════════════════════════════════════════════
// SLIDE 5 — URINE VALUES QUICK REF
// ══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
lightSlide(s);
tealBar(s, 0, 1.05);
sectionTag(s, "LAB KEYS");
slideTitle(s, "Key Urine Tests at a Glance", 0.4, 0.2, 9.2, C.white);
// Uosm table
s.addShape(pres.ShapeType.rect, { x:0.3, y:1.15, w:9.4, h:0.42, fill:{color:C.navy}, line:{color:C.navy} });
s.addText("URINE OSMOLALITY (Uosm)", { x:0.3, y:1.15, w:9.4, h:0.42, fontSize:13, bold:true, color:C.aqua, align:"center", valign:"middle", margin:0 });
const uosmRows = [
["< 100 mOsm/kg", "AVP suppressed", "Psychogenic polydipsia, beer potomania, EAH"],
["100 – 300", "Partial suppression", "Mixed picture, solute depletion"],
["> 300 mOsm/kg", "AVP active", "Most clinical hyponatremia"],
["> 400 mOsm/kg", "AVP dominant", "SIADH, severe volume depletion"],
];
const rowColors = [C.lightBg, C.white, C.lightBg, C.white];
uosmRows.forEach((row, i) => {
const y = 1.57 + i * 0.5;
s.addShape(pres.ShapeType.rect, { x:0.3, y, w:9.4, h:0.49, fill:{color:rowColors[i]}, line:{color:C.teal, pt:0.5} });
s.addText(row[0], { x:0.35, y, w:2.4, h:0.49, fontSize:12, bold:true, color:C.teal, valign:"middle" });
s.addText(row[1], { x:2.8, y, w:2.4, h:0.49, fontSize:12, color:C.navy, valign:"middle" });
s.addText(row[2], { x:5.25, y, w:4.4, h:0.49, fontSize:11, color:C.darkText, valign:"middle", italic:true });
});
// UNa strip
s.addShape(pres.ShapeType.rect, { x:0.3, y:3.65, w:9.4, h:0.42, fill:{color:C.teal}, line:{color:C.teal} });
s.addText("URINE SODIUM (UNa)", { x:0.3, y:3.65, w:9.4, h:0.42, fontSize:13, bold:true, color:C.white, align:"center", valign:"middle", margin:0 });
const unaRows = [
["< 20 mEq/L", "Extra-renal loss / Na⁺-avid state", "Diarrhea/vomiting, CHF, cirrhosis, nephrotic"],
["> 20–30 mEq/L", "Renal Na⁺ wasting or SIADH", "Diuretics, adrenal insufficiency, SIADH, CSW"],
];
unaRows.forEach((row, i) => {
const y = 4.07 + i * 0.5;
s.addShape(pres.ShapeType.rect, { x:0.3, y, w:9.4, h:0.49, fill:{color:i===0?C.lightBg:C.white}, line:{color:C.teal, pt:0.5} });
s.addText(row[0], { x:0.35, y, w:2.4, h:0.49, fontSize:12, bold:true, color:C.teal, valign:"middle" });
s.addText(row[1], { x:2.8, y, w:2.9, h:0.49, fontSize:12, color:C.navy, valign:"middle" });
s.addText(row[2], { x:5.75, y, w:3.9, h:0.49, fontSize:11, color:C.darkText, valign:"middle", italic:true });
});
s.addText("Quick Tip: Urine specific gravity 1.015 → Uosm ≈ 15 × 35 = 525 mOsm/L", {
x:0.3, y:5.12, w:9.4, h:0.35, fontSize:11, italic:true, color:C.gray, align:"center"
});
}
// ══════════════════════════════════════════════════════════════════════════════
// SLIDE 6 — THREE VOLUME CATEGORIES
// ══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
darkSlide(s);
sectionTag(s, "CATEGORIES");
slideTitle(s, "Three Volume Categories of Hyponatremia", 0.4, 0.2, 9.2, C.aqua);
accentLine(s, 1.0);
const cats = [
{
title:"HYPOVOLEMIC",
icon:"↓ Volume",
color:C.teal,
signs:["Orthostatic hypotension", "Tachycardia, dry MM", "↑BUN/Cr, ↑uric acid"],
causes:["Extra-renal: GI losses, burns, sweat (UNa < 20)", "Renal: thiazides, adrenal insuff, salt-losing nephropathy (UNa > 20)", "Cerebral salt wasting (CSW)"],
tx:"0.9% Normal Saline",
},
{
title:"EUVOLEMIC",
icon:"= Volume",
color:"1565C0",
signs:["Normal exam", "No edema, no depletion", "Most common in hospital"],
causes:["SIADH (most common)", "Hypothyroidism", "Secondary adrenal insufficiency", "Beer potomania, polydipsia, EAH"],
tx:"Fluid restriction ± urea ± vaptan",
},
{
title:"HYPERVOLEMIC",
icon:"↑ Volume",
color:"6A0572",
signs:["Peripheral edema", "Ascites, ↑JVP, S3 gallop", "\"Effective underfilling\""],
causes:["CHF (UNa < 10)", "Cirrhosis (UNa < 10)", "Nephrotic syndrome (UNa < 10)", "Renal failure (UNa > 20)"],
tx:"Treat underlying cause, fluid restrict",
},
];
cats.forEach((cat, i) => {
const x = 0.22 + i * 3.26;
s.addShape(pres.ShapeType.rect, { x, y:1.18, w:3.05, h:4.15, fill:{color:cat.color, transparency:15}, line:{color:cat.color, pt:2} });
s.addShape(pres.ShapeType.rect, { x, y:1.18, w:3.05, h:0.5, fill:{color:cat.color}, line:{color:cat.color} });
s.addText(cat.icon+" "+cat.title, { x, y:1.18, w:3.05, h:0.5, fontSize:13, bold:true, color:C.white, align:"center", valign:"middle", margin:0 });
s.addText("Signs:", { x:x+0.1, y:1.75, w:2.85, h:0.3, fontSize:11, bold:true, color:C.yellow, valign:"middle" });
cat.signs.forEach((sg, j) => {
s.addText("• "+sg, { x:x+0.15, y:2.05+j*0.34, w:2.8, h:0.33, fontSize:10.5, color:C.white, fontFace:"Calibri" });
});
s.addText("Causes:", { x:x+0.1, y:3.15, w:2.85, h:0.3, fontSize:11, bold:true, color:C.yellow, valign:"middle" });
cat.causes.forEach((c, j) => {
s.addText("• "+c, { x:x+0.15, y:3.45+j*0.32, w:2.8, h:0.31, fontSize:9.5, color:C.white, fontFace:"Calibri", wrap:true });
});
});
}
// ══════════════════════════════════════════════════════════════════════════════
// SLIDE 7 — SIADH DEEP DIVE
// ══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
lightSlide(s);
tealBar(s, 0, 1.05);
sectionTag(s, "SIADH");
slideTitle(s, "SIADH: The Most Common Euvolemic Cause", 0.4, 0.2, 9.2, C.white);
// Criteria box
s.addShape(pres.ShapeType.rect, { x:0.3, y:1.15, w:4.4, h:3.5, fill:{color:C.white}, line:{color:C.teal, pt:2},
shadow:{type:"outer", color:"000000", blur:8, offset:2, angle:135, opacity:0.10} });
s.addShape(pres.ShapeType.rect, { x:0.3, y:1.15, w:4.4, h:0.42, fill:{color:C.teal}, line:{color:C.teal} });
s.addText("Diagnostic Criteria", { x:0.3, y:1.15, w:4.4, h:0.42, fontSize:13, bold:true, color:C.white, align:"center", valign:"middle", margin:0 });
const criteria = [
"Hypotonic hyponatremia (Posm < 275 mOsm/kg)",
"Urine osmolality inappropriately elevated (> 200 mOsm/kg)",
"Urine Na⁺ > 20 mEq/L",
"Clinical euvolemia",
"Normal adrenal, renal, cardiac, hepatic, thyroid function",
"Serum uric acid typically < 4 mg/dL (hypouricemia)",
];
criteria.forEach((c, i) => {
s.addShape(pres.ShapeType.rect, { x:0.3, y:1.57+i*0.38, w:0.38, h:0.34, fill:{color:C.aqua}, line:{color:C.aqua} });
s.addText((i+1).toString(), { x:0.3, y:1.57+i*0.38, w:0.38, h:0.34, fontSize:11, bold:true, color:C.white, align:"center", valign:"middle", margin:0 });
s.addText(c, { x:0.73, y:1.57+i*0.38, w:3.92, h:0.34, fontSize:11, color:C.darkText, valign:"middle" });
});
// Causes box
s.addShape(pres.ShapeType.rect, { x:5.0, y:1.15, w:4.7, h:3.5, fill:{color:C.white}, line:{color:C.navy, pt:1.5} });
s.addShape(pres.ShapeType.rect, { x:5.0, y:1.15, w:4.7, h:0.42, fill:{color:C.navy}, line:{color:C.navy} });
s.addText("Common Causes", { x:5.0, y:1.15, w:4.7, h:0.42, fontSize:13, bold:true, color:C.aqua, align:"center", valign:"middle", margin:0 });
const causeGroups = [
{ cat:"CNS:", items:"Meningitis, SAH, stroke, trauma, psychosis" },
{ cat:"Pulmonary:", items:"Pneumonia, TB, ARDS, PPV" },
{ cat:"Malignancy:", items:"SCLC (most common, 10–15%), lymphoma, pancreas, bladder" },
{ cat:"Drugs:", items:"SSRIs, carbamazepine, cyclophosphamide, NSAIDs, opioids, amiodarone" },
{ cat:"Other:", items:"Surgery, pain, nausea, HIV, hypothyroidism, adrenal insufficiency" },
];
causeGroups.forEach((g, i) => {
s.addText([
{text:g.cat+" ", options:{bold:true, color:C.teal, fontSize:11.5}},
{text:g.items, options:{bold:false, color:C.darkText, fontSize:11.5}}
], { x:5.15, y:1.65+i*0.55, w:4.45, h:0.5, valign:"top", wrap:true });
});
// U/P ratio callout
s.addShape(pres.ShapeType.rect, { x:0.3, y:4.73, w:9.4, h:0.72, fill:{color:C.yellow, transparency:20}, line:{color:C.yellow, pt:1.5} });
s.addText([
{text:"U/P Electrolyte Ratio: ", options:{bold:true, fontSize:12.5, color:C.navy}},
{text:"(Urine [Na⁺]+[K⁺]) / Plasma [Na⁺] | ", options:{fontSize:12, color:C.navy}},
{text:"> 1 → restrict < 500 mL/d | ~1 → 500–700 mL/d | < 1 → < 1 L/d", options:{fontSize:12, color:C.darkText}},
], { x:0.3, y:4.73, w:9.4, h:0.72, valign:"middle", align:"center" });
}
// ══════════════════════════════════════════════════════════════════════════════
// SLIDE 8 — ODS / TREATMENT SAFETY
// ══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
darkSlide(s);
sectionTag(s, "TREATMENT SAFETY");
slideTitle(s, "Osmotic Demyelination Syndrome (ODS)", 0.4, 0.2, 9.2, C.red);
accentLine(s, 1.0);
// Left panel: mechanism + risk
s.addShape(pres.ShapeType.rect, { x:0.25, y:1.15, w:4.6, h:4.15, fill:{color:"1C0A0A"}, line:{color:C.red, pt:2} });
s.addShape(pres.ShapeType.rect, { x:0.25, y:1.15, w:4.6, h:0.42, fill:{color:C.red}, line:{color:C.red} });
s.addText("Why It Happens", { x:0.25, y:1.15, w:4.6, h:0.42, fontSize:13, bold:true, color:C.white, align:"center", valign:"middle", margin:0 });
bodyText(s, [
"Rapid correction of chronic hyponatremia",
"Water exits brain cells → ECF becomes hypertonic relative to cells",
"Cells that lost organic osmolytes cannot maintain volume",
"Myelin damage — pons most vulnerable (central pontine myelinolysis)",
"Symptoms appear 2–6 days AFTER rapid correction (not immediately)",
], 0.4, 1.65, 4.3, 2.5, C.white, 11.5);
s.addText("Risk Factors:", { x:0.4, y:4.2, w:4.3, h:0.3, fontSize:12, bold:true, color:C.yellow, valign:"middle" });
s.addText("Na⁺ < 120 | Duration > 48 h | Hypokalemia | Alcoholism\nCirrhosis | Malnutrition | Beer potomania | Vaptans", {
x:0.4, y:4.52, w:4.3, h:0.72, fontSize:11, color:C.white, fontFace:"Calibri", wrap:true
});
// Right panel: limits + tx
s.addShape(pres.ShapeType.rect, { x:5.15, y:1.15, w:4.6, h:4.15, fill:{color:"0A1A0A"}, line:{color:C.aqua, pt:2} });
s.addShape(pres.ShapeType.rect, { x:5.15, y:1.15, w:4.6, h:0.42, fill:{color:C.aqua}, line:{color:C.aqua} });
s.addText("Correction Limits & Management", { x:5.15, y:1.15, w:4.6, h:0.42, fontSize:12, bold:true, color:C.navy, align:"center", valign:"middle", margin:0 });
// Correction boxes
const limits = [["First 24 h","≤ 8–10 mEq/L","(≤12 if acute)"],["First 48 h","≤ 18 mEq/L","total"]];
limits.forEach((l, i) => {
s.addShape(pres.ShapeType.rect, { x:5.25+i*2.2, y:1.65, w:2.0, h:1.2, fill:{color:"1A2A1A"}, line:{color:C.aqua, pt:1.5} });
s.addText(l[0], { x:5.25+i*2.2, y:1.65, w:2.0, h:0.38, fontSize:11, bold:true, color:C.gray, align:"center", valign:"middle" });
s.addText(l[1], { x:5.25+i*2.2, y:2.03, w:2.0, h:0.45, fontSize:18, bold:true, color:C.yellow, align:"center", valign:"middle" });
s.addText(l[2], { x:5.25+i*2.2, y:2.5, w:2.0, h:0.3, fontSize:10, color:C.gray, align:"center", italic:true });
});
s.addText("If Overcorrected:", { x:5.25, y:2.95, w:4.3, h:0.3, fontSize:12, bold:true, color:C.red, valign:"middle" });
bodyText(s, [
"Give 5% dextrose water at 3 mL/kg/h",
"Add DDAVP to stop further free-water excretion",
"Loop diuretics",
"Target: bring Na⁺ back to safe correction limit",
], 5.25, 3.28, 4.3, 1.85, C.white, 11.5);
// Symptoms bar
s.addShape(pres.ShapeType.rect, { x:0.25, y:5.35, w:9.5, h:0.42, fill:{color:C.red, transparency:20}, line:{color:C.red} });
s.addText("ODS Symptoms (days 2–6 post-correction): Dysarthria · Dysphagia · Paraparesis · Locked-in · Seizures · Coma", {
x:0.25, y:5.35, w:9.5, h:0.42, fontSize:11.5, bold:true, color:C.white, align:"center", valign:"middle", margin:0
});
}
// ══════════════════════════════════════════════════════════════════════════════
// SLIDE 9 — TREATMENT SUMMARY
// ══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
lightSlide(s);
tealBar(s, 0, 1.05);
sectionTag(s, "TREATMENT");
slideTitle(s, "Treatment by Cause", 0.4, 0.2, 9.2, C.white);
// Emergency box
s.addShape(pres.ShapeType.rect, { x:0.3, y:1.15, w:9.4, h:1.5, fill:{color:"FFF3E0"}, line:{color:C.red, pt:2} });
s.addShape(pres.ShapeType.rect, { x:0.3, y:1.15, w:9.4, h:0.42, fill:{color:C.red}, line:{color:C.red} });
s.addText("EMERGENCY: Symptomatic / Seizures / Coma → 3% Hypertonic NaCl", {
x:0.3, y:1.15, w:9.4, h:0.42, fontSize:13, bold:true, color:C.white, align:"center", valign:"middle", margin:0
});
s.addText("150 mL 3% NaCl IV over 20 min → recheck Na⁺ → repeat up to 3× total (450 mL max)\nStop when symptoms resolve OR Na⁺ rises 4–6 mEq/L | Limit: ≤ 8–12 mEq/L / 24 h", {
x:0.5, y:1.6, w:9.0, h:0.96, fontSize:12, color:C.darkText, valign:"middle", wrap:true
});
// Treatment table
const rows = [
{ cause:"Hypovolemic (GI/extra-renal)", tx:"0.9% NaCl — volume repletion → AVP suppresses → aquaresis", color:C.teal },
{ cause:"Thiazide-induced", tx:"Stop thiazide, correct K⁺ (KCl raises Na⁺), consider loop diuretic instead", color:C.teal },
{ cause:"Adrenal insufficiency", tx:"IV hydrocortisone + NS — draw cortisol first, don't delay treatment", color:C.teal },
{ cause:"SIADH", tx:"Fluid restriction (U/P ratio guided) ± oral Na⁺ ± urea ± tolvaptan (inpatient)", color:"1565C0" },
{ cause:"Hypothyroidism", tx:"Thyroid hormone (T4) replacement", color:"1565C0" },
{ cause:"CHF / Cirrhosis", tx:"Treat underlying cause + fluid restriction + vaptan if refractory", color:"6A0572" },
{ cause:"Beer potomania", tx:"0.9% NS + normal diet — HIGH ODS RISK — monitor very closely", color:C.red },
];
rows.forEach((row, i) => {
const y = 2.72 + i * 0.41;
s.addShape(pres.ShapeType.rect, { x:0.3, y, w:9.4, h:0.4, fill:{color:i%2===0?C.white:C.lightBg}, line:{color:C.teal, pt:0.5} });
s.addShape(pres.ShapeType.rect, { x:0.3, y, w:0.14, h:0.4, fill:{color:row.color}, line:{color:row.color} });
s.addText(row.cause, { x:0.5, y, w:3.0, h:0.4, fontSize:11, bold:true, color:C.navy, valign:"middle" });
s.addText(row.tx, { x:3.55, y, w:6.1, h:0.4, fontSize:10.5, color:C.darkText, valign:"middle", wrap:true });
});
}
// ══════════════════════════════════════════════════════════════════════════════
// SLIDE 10 — CLINICAL CASE 1 (Hypovolemic)
// ══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
darkSlide(s);
sectionTag(s, "CASE 1");
slideTitle(s, "Case 1: The Dehydrated Vomiter", 0.4, 0.2, 9.2, C.yellow);
accentLine(s, 1.0);
// Vignette
s.addShape(pres.ShapeType.rect, { x:0.25, y:1.15, w:9.5, h:1.0, fill:{color:C.teal, transparency:80}, line:{color:C.teal, pt:1} });
s.addText("67F | 3 days vomiting | BP 95/60 → 78/50 orthostatic | HR 112 | Dry MM, skin tenting, no edema", {
x:0.4, y:1.2, w:9.2, h:0.9, fontSize:12.5, color:C.white, fontFace:"Calibri", valign:"middle", italic:true
});
// Labs row
const labs = [["Na⁺","124 mEq/L"],["Posm","258 mOsm/kg"],["Uosm","680 mOsm/kg"],["UNa","8 mEq/L"],["BUN","42"],["K⁺","3.1"]];
labs.forEach((l, i) => {
const x = 0.25 + i * 1.6;
s.addShape(pres.ShapeType.rect, { x, y:2.25, w:1.45, h:0.72, fill:{color:C.navy, transparency:30}, line:{color:C.aqua, pt:1.5} });
s.addText(l[0], { x, y:2.25, w:1.45, h:0.35, fontSize:11, bold:true, color:C.aqua, align:"center", valign:"middle", margin:0 });
s.addText(l[1], { x, y:2.6, w:1.45, h:0.37, fontSize:12, bold:true, color:C.yellow, align:"center", valign:"middle", margin:0 });
});
// Analysis
const steps = [
["Step 1 — Posm 258", "TRUE hypotonic hyponatremia ✓"],
["Step 2 — Volume", "HYPOVOLEMIC — orthostatics, tachycardia, ↑BUN"],
["Step 3 — Uosm 680", "AVP very active (concentrating urine to preserve volume)"],
["Step 4 — UNa 8", "EXTRA-RENAL loss — kidneys avid for Na⁺ (GI losses)"],
];
steps.forEach((st, i) => {
const x = 0.25 + (i%2)*4.75;
const y = 3.1 + Math.floor(i/2)*0.9;
s.addShape(pres.ShapeType.rect, { x, y, w:4.45, h:0.82, fill:{color:"0A1A2A"}, line:{color:C.teal, pt:1} });
s.addText(st[0], { x:x+0.1, y, w:4.25, h:0.37, fontSize:11, bold:true, color:C.aqua, valign:"middle" });
s.addText(st[1], { x:x+0.1, y:y+0.37, w:4.25, h:0.4, fontSize:11, color:C.white, valign:"middle", wrap:true });
});
s.addShape(pres.ShapeType.rect, { x:0.25, y:5.0, w:9.5, h:0.42, fill:{color:C.teal}, line:{color:C.teal} });
s.addText("Dx: Hypovolemic hyponatremia (GI losses) | Rx: 0.9% NaCl + correct K⁺ | Monitor Na⁺ q4–6h", {
x:0.25, y:5.0, w:9.5, h:0.42, fontSize:12.5, bold:true, color:C.white, align:"center", valign:"middle", margin:0
});
}
// ══════════════════════════════════════════════════════════════════════════════
// SLIDE 11 — CASE 2 (SIADH / Cancer)
// ══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
lightSlide(s);
tealBar(s, 0, 1.05);
sectionTag(s, "CASE 2");
slideTitle(s, "Case 2: SIADH in Small Cell Lung Cancer", 0.4, 0.2, 9.2, C.white);
s.addShape(pres.ShapeType.rect, { x:0.3, y:1.15, w:9.4, h:0.78, fill:{color:C.navy, transparency:85}, line:{color:C.navy, pt:1} });
s.addText("52M | SCLC | 1 week fatigue, confusion, headache | No edema, no orthostasis", {
x:0.5, y:1.2, w:9.0, h:0.68, fontSize:12.5, color:C.darkText, fontFace:"Calibri", valign:"middle", italic:true
});
const labs = [["Na⁺","118 mEq/L"],["Posm","242 mOsm/kg"],["Uosm","520 mOsm/kg"],["UNa","65 mEq/L"],["Uric Acid","2.8 mg/dL"],["K⁺","3.9"]];
labs.forEach((l, i) => {
const x = 0.3 + i * 1.6;
s.addShape(pres.ShapeType.rect, { x, y:2.05, w:1.45, h:0.72, fill:{color:C.teal, transparency:85}, line:{color:C.teal, pt:1.5} });
s.addText(l[0], { x, y:2.05, w:1.45, h:0.35, fontSize:11, bold:true, color:C.teal, align:"center", valign:"middle", margin:0 });
s.addText(l[1], { x, y:2.4, w:1.45, h:0.37, fontSize:12, bold:true, color:C.navy, align:"center", valign:"middle", margin:0 });
});
const analysis = [
"Posm 242 → true hypotonic hyponatremia",
"Euvolemic — no edema, no depletion signs",
"Uosm 520 → AVP active despite hyponatremia (inappropriate!)",
"UNa 65 → kidney NOT retaining Na⁺",
"Uric acid 2.8 mg/dL → hypouricemia = SIADH physiology",
"SCLC context → paraneoplastic ectopic AVP production",
];
analysis.forEach((a, i) => {
const x = 0.3 + (i%2)*4.75;
const y = 2.88 + Math.floor(i/2)*0.55;
s.addShape(pres.ShapeType.rect, { x, y, w:0.34, h:0.5, fill:{color:C.teal}, line:{color:C.teal} });
s.addText((i+1).toString(), { x, y, w:0.34, h:0.5, fontSize:11, bold:true, color:C.white, align:"center", valign:"middle", margin:0 });
s.addText(a, { x:x+0.38, y, w:4.28, h:0.5, fontSize:11.5, color:C.darkText, valign:"middle", wrap:true });
});
s.addShape(pres.ShapeType.rect, { x:0.3, y:5.55, w:9.4, h:0.42, fill:{color:C.navy}, line:{color:C.navy} });
s.addText("Dx: SIADH (paraneoplastic SCLC) | Rx: Fluid restriction < 1 L/d (U/P = 0.70) ± urea ± tolvaptan | Treat SCLC", {
x:0.3, y:5.55, w:9.4, h:0.42, fontSize:11.5, bold:true, color:C.aqua, align:"center", valign:"middle", margin:0
});
}
// ══════════════════════════════════════════════════════════════════════════════
// SLIDE 12 — CASES 3 & 4 (EAH + Thiazide pitfall)
// ══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
darkSlide(s);
sectionTag(s, "CASES 3 & 4");
slideTitle(s, "More Clinical Cases", 0.4, 0.2, 9.2, C.aqua);
accentLine(s, 1.0);
// Case 3 — Left
s.addShape(pres.ShapeType.rect, { x:0.25, y:1.15, w:4.6, h:4.55, fill:{color:"0A1520"}, line:{color:C.teal, pt:2} });
s.addShape(pres.ShapeType.rect, { x:0.25, y:1.15, w:4.6, h:0.42, fill:{color:C.teal}, line:{color:C.teal} });
s.addText("Case 3 — The Marathon Runner (EAH)", { x:0.25, y:1.15, w:4.6, h:0.42, fontSize:12, bold:true, color:C.white, align:"center", valign:"middle", margin:0 });
s.addText("29F, collapses post-marathon, seizing\nDrank water throughout race, weight gain\nNa⁺ 112 | Posm 228 | Uosm 68 | UNa 12", {
x:0.4, y:1.65, w:4.3, h:0.95, fontSize:11, color:C.gray, fontFace:"Calibri", italic:true, wrap:true
});
s.addText("Key Clue: Uosm < 100 → AVP is SUPPRESSED\n→ Pure water intoxication (not SIADH)\n→ ACUTE onset (< 24 h) = high-risk neurologic\n→ Weight gain during race = excessive free H₂O", {
x:0.4, y:2.65, w:4.3, h:1.4, fontSize:11.5, color:C.white, fontFace:"Calibri", wrap:true
});
s.addShape(pres.ShapeType.rect, { x:0.25, y:4.08, w:4.6, h:0.56, fill:{color:C.red, transparency:20}, line:{color:C.red} });
s.addText("Rx: 150 mL 3% NaCl IV stat (acute → ODS risk low)\nRepeat ×3 max — stop when seizing resolves", {
x:0.35, y:4.1, w:4.4, h:0.52, fontSize:11, bold:true, color:C.white, fontFace:"Calibri", wrap:true
});
// Case 4 — Right
s.addShape(pres.ShapeType.rect, { x:5.15, y:1.15, w:4.6, h:4.55, fill:{color:"100A20"}, line:{color:C.yellow, pt:2} });
s.addShape(pres.ShapeType.rect, { x:5.15, y:1.15, w:4.6, h:0.42, fill:{color:"6A0572"}, line:{color:"6A0572"} });
s.addText("Case 4 — Thiazide Mimic of SIADH", { x:5.15, y:1.15, w:4.6, h:0.42, fontSize:12, bold:true, color:C.white, align:"center", valign:"middle", margin:0 });
s.addText("72F on HCTZ × 3 weeks for HTN\nWeakness, mild confusion, no edema\nNa⁺ 122 | Posm 256 | Uosm 380 | UNa 45 | K⁺ 2.8", {
x:5.3, y:1.65, w:4.3, h:0.95, fontSize:11, color:C.gray, fontFace:"Calibri", italic:true, wrap:true
});
s.addText("Looks exactly like SIADH but...\n► Started thiazide 3 weeks ago\n► Hypokalemia (K⁺ 2.8) — key clue!\n► Thiazide blocks DCT NaCl cotransporter → impairs diluting segment + volume depletion → ↑AVP\n► Do NOT diagnose SIADH until 1–2 weeks after stopping thiazide", {
x:5.3, y:2.65, w:4.3, h:1.9, fontSize:11, color:C.white, fontFace:"Calibri", wrap:true
});
s.addShape(pres.ShapeType.rect, { x:5.15, y:4.08, w:4.6, h:0.56, fill:{color:C.yellow, transparency:30}, line:{color:C.yellow} });
s.addText("Rx: Stop HCTZ · Correct K⁺ (KCl raises Na⁺) · 0.9% NS if symptomatic · Monitor closely", {
x:5.25, y:4.1, w:4.4, h:0.52, fontSize:11, bold:true, color:C.navy, fontFace:"Calibri", wrap:true
});
}
// ══════════════════════════════════════════════════════════════════════════════
// SLIDE 13 — MASTER TABLE
// ══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
lightSlide(s);
tealBar(s, 0, 1.05);
sectionTag(s, "SUMMARY TABLE");
slideTitle(s, "High-Yield Summary Table", 0.4, 0.2, 9.2, C.white);
const hdr = ["Condition","Volume","Uosm","UNa","Key Clue","Treatment"];
const hdrW = [2.0, 0.9, 0.8, 0.7, 2.1, 3.2];
let cx = 0.18;
hdr.forEach((h, i) => {
s.addShape(pres.ShapeType.rect, { x:cx, y:1.12, w:hdrW[i], h:0.38, fill:{color:C.navy}, line:{color:C.navy} });
s.addText(h, { x:cx, y:1.12, w:hdrW[i], h:0.38, fontSize:10.5, bold:true, color:C.aqua, align:"center", valign:"middle", margin:0 });
cx += hdrW[i];
});
const rows = [
["GI / Extra-renal loss","↓","High","< 20","Orthostasis, vomiting","0.9% NS"],
["Thiazide diuretic","↓ / Eu","High","> 20","Hypokalemia","Stop drug, correct K⁺"],
["Adrenal insufficiency (1°)","↓","High",">> 20","Hyperkalemia, pigment.","Hydrocortisone + NS"],
["CSW","↓","High","> 20","CNS pathology (SAH)","Na⁺ + volume"],
["SIADH","Eu","> 200","> 30","Hypouricemia, exclusion dx","Fluid restrict ± urea ± vaptan"],
["Hypothyroidism","Eu","Var.","Var.","↑TSH, myxedema","T4 replacement"],
["Beer potomania","Eu","< 200","< 20","Alcoholism, low solute","NS + diet — HIGH ODS risk!"],
["Psychogenic polydipsia","Eu","< 100","Low","Psych hx, schizophrenia","Fluid restriction"],
["EAH","Eu","< 100","Low","Post-race, weight gain","3% NaCl if severe (acute)"],
["CHF / Cirrhosis","↑","High","< 10","Edema, ascites, ↑BNP","Treat cause, fluid restrict"],
["Renal failure","↑","Var.","> 20","↑Cr, ↑K⁺","Dialysis"],
];
const rowH = 0.37;
rows.forEach((row, ri) => {
let rx = 0.18;
const bg = ri % 2 === 0 ? C.white : C.lightBg;
const volColor = row[1]==="↓" ? C.teal : row[1]==="↑" ? "6A0572" : "1565C0";
hdrW.forEach((w, ci) => {
s.addShape(pres.ShapeType.rect, { x:rx, y:1.5+ri*rowH, w, h:rowH, fill:{color:bg}, line:{color:C.teal, pt:0.5} });
const isVol = ci === 1;
s.addText(row[ci], {
x:rx, y:1.5+ri*rowH, w, h:rowH,
fontSize: ci===5 ? 9 : 10,
bold: ci===0 || ci===1,
color: isVol ? volColor : (ci===4 ? C.teal : C.darkText),
align: ci===0 ? "left" : "center",
valign:"middle",
wrap: true,
margin: ci===0 ? [0,0,0,4] : 0,
});
rx += w;
});
});
}
// ══════════════════════════════════════════════════════════════════════════════
// SLIDE 14 — KEY TAKEAWAYS
// ══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
darkSlide(s);
s.addShape(pres.ShapeType.rect, { x:0, y:0, w:0.18, h:"100%", fill:{color:C.aqua}, line:{color:C.aqua} });
s.addShape(pres.ShapeType.ellipse, { x:7.2, y:-0.8, w:4, h:4, fill:{color:C.teal, transparency:80}, line:{color:C.teal, transparency:80} });
s.addText("Key Takeaways", { x:0.5, y:0.35, w:9, h:0.6, fontSize:30, bold:true, color:C.aqua, fontFace:"Calibri" });
accentLine(s, 1.05);
const takes = [
["1","Serum [Na⁺] reflects water balance, not total body Na⁺ — volume status is the first clinical step"],
["2","Always exclude pseudohyponatremia (check measured Posm) and hypertonic causes (glucose) first"],
["3","Uosm < 100 = AVP suppressed → polydipsia / EAH. Most other cases have Uosm > 100"],
["4","UNa < 20 with hypovolemia = extra-renal loss. High UNa despite low [Na⁺] = SIADH or renal wasting"],
["5","SIADH is a diagnosis of exclusion — rule out hypothyroidism, adrenal insufficiency, diuretics first"],
["6","Correction limit: ≤ 8–10 mEq/L/24 h in chronic hyponatremia to prevent ODS"],
["7","Symptomatic acute hyponatremia → 3% NaCl stat (150 mL bolus, repeat up to 3×)"],
["8","Hypokalemia correction itself raises plasma [Na⁺] — watch for inadvertent overcorrection"],
];
takes.forEach((t, i) => {
const y = 1.2 + i * 0.5;
s.addShape(pres.ShapeType.ellipse, { x:0.45, y:y+0.08, w:0.34, h:0.34, fill:{color:C.teal}, line:{color:C.teal} });
s.addText(t[0], { x:0.45, y:y+0.08, w:0.34, h:0.34, fontSize:11, bold:true, color:C.white, align:"center", valign:"middle", margin:0 });
s.addText(t[1], { x:0.9, y, w:8.8, h:0.48, fontSize:12.5, color:C.white, fontFace:"Calibri", valign:"middle", wrap:true });
});
s.addText("Sources: Harrison's 22E · Brenner & Rector · Tintinalli's EM · NKF Primer · Symptom to Diagnosis 4E", {
x:0.5, y:5.25, w:9, h:0.3, fontSize:9.5, color:C.gray, fontFace:"Calibri", italic:true
});
}
// ══════════════════════════════════════════════════════════════════════════════
// WRITE FILE
// ══════════════════════════════════════════════════════════════════════════════
pres.writeFile({ fileName: "/home/daytona/workspace/hyponatremia-ppt/Hyponatremia_Evaluation.pptx" })
.then(() => console.log("✓ Done: Hyponatremia_Evaluation.pptx"))
.catch(err => { console.error("Error:", err); process.exit(1); });
~/hyponatremia-ppt/build.js
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/hyponatremia-ppt/build.js'
cat > /home/daytona/workspace/hyponatremia-ppt/build.js << 'ENDOFSCRIPT' const pptxgen = require("pptxgenjs"); const pres = new pptxgen(); pres.layout = "LAYOUT_16x9"; pres.title = "Hyponatremia: Evaluation & Management"; pres.author = "Orris Medical Education"; const C = { navy: "0A2342", teal: "0D7377", aqua: "14BDAC", white: "FFFFFF", offWhite:"F0F4F8", yellow: "F5C518", red: "E63946", gray: "94A3B8", lightBg: "EBF4F6", darkText:"1E293B", }; function darkSlide(slide) { slide.addShape(pres.ShapeType.rect, { x:0, y:0, w:"100%", h:"100%", fill:{color:C.navy}, line:{color:C.navy} }); } function lightSlide(slide) { slide.addShape(pres.ShapeType.rect, { x:0, y:0, w:"100%", h:"100%", fill:{color:C.offWhite}, line:{color:C.offWhite} }); } function tealBar(slide, y=0, h=1.05) { slide.addShape(pres.ShapeType.rect, { x:0, y:y, w:"100%", h:h, fill:{color:C.teal}, line:{color:C.teal} }); } function accentLine(slide, y) { slide.addShape(pres.ShapeType.rect, { x:0.4, y:y, w:1.2, h:0.07, fill:{color:C.aqua}, line:{color:C.aqua} }); } function sectionTag(slide, label) { slide.addShape(pres.ShapeType.rect, { x:0, y:0, w:2.6, h:0.38, fill:{color:C.aqua}, line:{color:C.aqua} }); slide.addText(label, { x:0, y:0, w:2.6, h:0.38, fontSize:11, bold:true, color:C.navy, align:"center", valign:"middle", margin:0 }); } function slideTitle(slide, title, x, y, w, color) { x = x||0.4; y = y||0.2; w = w||9.2; color = color||C.white; slide.addText(title, { x, y, w, h:0.65, fontSize:26, bold:true, color, fontFace:"Calibri", valign:"middle" }); } // ─── SLIDE 1: TITLE ─────────────────────────────────────────────────────────── { const s = pres.addSlide(); darkSlide(s); s.addShape(pres.ShapeType.rect, { x:0, y:0, w:0.18, h:"100%", fill:{color:C.aqua}, line:{color:C.aqua} }); s.addShape(pres.ShapeType.ellipse, { x:7.5, y:-1.2, w:4.5, h:4.5, fill:{color:C.teal, transparency:75}, line:{color:C.teal, transparency:75} }); s.addShape(pres.ShapeType.ellipse, { x:8.2, y:2.8, w:2.8, h:2.8, fill:{color:C.aqua, transparency:85}, line:{color:C.aqua, transparency:85} }); s.addText("HYPONATREMIA", { x:0.5, y:1.2, w:9, h:0.7, fontSize:44, bold:true, color:C.aqua, charSpacing:6, fontFace:"Calibri" }); s.addText("Evaluation & Management", { x:0.5, y:2.0, w:9, h:0.55, fontSize:26, color:C.white, fontFace:"Calibri" }); s.addText("From Basics to Clinical Cases", { x:0.5, y:2.65, w:9, h:0.4, fontSize:16, color:C.gray, fontFace:"Calibri", italic:true }); accentLine(s, 3.2); s.addText("Based on Harrison's 22E · Brenner & Rector · Tintinalli's EM · NKF Primer", { x:0.5, y:4.8, w:9, h:0.35, fontSize:11, color:C.gray, fontFace:"Calibri", italic:true }); } // ─── SLIDE 2: DEFINITION & EPIDEMIOLOGY ─────────────────────────────────────── { const s = pres.addSlide(); lightSlide(s); tealBar(s, 0, 1.05); sectionTag(s, "BASICS"); slideTitle(s, "Definition & Epidemiology", 0.4, 0.2, 9.2, C.white); const boxes = [ { label:"Definition", val:"Na\u207a < 135 mEq/L", sub:"Symptoms rare until \u2264125 mEq/L" }, { label:"Prevalence", val:"Up to 22%", sub:"Of all hospitalized patients" }, { label:"Acute", val:"< 48 hours", sub:"Brain not yet adapted — high risk" }, { label:"Chronic", val:"> 48 hours", sub:"Brain adapted — symptoms milder" }, ]; boxes.forEach((b, i) => { const x = 0.3 + i * 2.38; s.addShape(pres.ShapeType.rect, { x, y:1.25, w:2.15, h:3.6, fill:{color:C.white}, line:{color:C.teal, pt:2}, shadow:{type:"outer", color:"000000", blur:8, offset:2, angle:135, opacity:0.10} }); s.addShape(pres.ShapeType.rect, { x, y:1.25, w:2.15, h:0.45, fill:{color:C.teal}, line:{color:C.teal} }); s.addText(b.label, { x, y:1.25, w:2.15, h:0.45, fontSize:11, bold:true, color:C.white, align:"center", valign:"middle", margin:0 }); s.addText(b.val, { x, y:1.78, w:2.15, h:1.1, fontSize:17, bold:true, color:C.navy, align:"center", valign:"middle", fontFace:"Calibri" }); s.addText(b.sub, { x, y:2.88, w:2.15, h:1.5, fontSize:11, color:C.darkText, align:"center", valign:"top", fontFace:"Calibri", wrap:true }); }); s.addShape(pres.ShapeType.rect, { x:0.3, y:5.0, w:9.4, h:0.4, fill:{color:C.navy}, line:{color:C.navy} }); s.addText("Severity: Mild 130-135 | Moderate 125-130 | Severe < 125 mEq/L", { x:0.3, y:5.0, w:9.4, h:0.4, fontSize:12, bold:true, color:C.aqua, align:"center", valign:"middle", margin:0 }); } // ─── SLIDE 3: PHYSIOLOGY ────────────────────────────────────────────────────── { const s = pres.addSlide(); lightSlide(s); tealBar(s, 0, 1.05); sectionTag(s, "PHYSIOLOGY"); slideTitle(s, "Why Does Hyponatremia Happen?", 0.4, 0.2, 9.2, C.white); s.addShape(pres.ShapeType.rect, { x:0.3, y:1.2, w:4.55, h:4.1, fill:{color:C.white}, line:{color:C.teal, pt:1.5} }); s.addShape(pres.ShapeType.rect, { x:0.3, y:1.2, w:4.55, h:0.42, fill:{color:C.navy}, line:{color:C.navy} }); s.addText("Key Concept", { x:0.3, y:1.2, w:4.55, h:0.42, fontSize:12, bold:true, color:C.aqua, align:"center", valign:"middle", margin:0 }); s.addText([ {text:"Serum [Na+] = Total Body Na+ / Total Body Water\n", options:{bold:true, breakLine:false}}, {text:"Hyponatremia = excess water relative to sodium\n"}, {text:"AVP (vasopressin) = main regulator — promotes renal free-water reabsorption\n"}, {text:"Most cases: excess AVP + free water intake\n"}, {text:"Volume status modulates AVP: hypovolemia raises AVP even at normal osmolality"}, ], { x:0.5, y:1.72, w:4.2, h:3.4, fontSize:12.5, color:C.darkText, fontFace:"Calibri", valign:"top", wrap:true }); s.addShape(pres.ShapeType.rect, { x:5.15, y:1.2, w:4.55, h:4.1, fill:{color:C.white}, line:{color:C.aqua, pt:1.5} }); s.addShape(pres.ShapeType.rect, { x:5.15, y:1.2, w:4.55, h:0.42, fill:{color:C.aqua}, line:{color:C.aqua} }); s.addText("Two Defense Mechanisms", { x:5.15, y:1.2, w:4.55, h:0.42, fontSize:12, bold:true, color:C.navy, align:"center", valign:"middle", margin:0 }); s.addText([ {text:"1 AVP release by posterior pituitary -> water reabsorption\n"}, {text:"2 Thirst -> drives oral water intake\n"}, {text:"Defect in either + free water intake -> hyponatremia\n\n"}, {text:"Brain cell swelling -> neurological symptoms\n\n"}, {text:"Chronic: brain adapts by exporting organic osmolytes (taurine, glutamate, myoinositol) -> less symptomatic"}, ], { x:5.35, y:1.72, w:4.2, h:3.4, fontSize:12.5, color:C.darkText, fontFace:"Calibri", valign:"top", wrap:true }); s.addShape(pres.ShapeType.rect, { x:0.3, y:5.35, w:9.4, h:0.42, fill:{color:C.yellow, transparency:15}, line:{color:C.yellow} }); s.addText("Effective Osmolality = 2 x [Na+] + Glucose/18 | Normal: 275-290 mOsm/kg", { x:0.3, y:5.35, w:9.4, h:0.42, fontSize:13, bold:true, color:C.navy, align:"center", valign:"middle", margin:0 }); } // ─── SLIDE 4: 4-STEP FRAMEWORK ──────────────────────────────────────────────── { const s = pres.addSlide(); darkSlide(s); sectionTag(s, "DIAGNOSIS"); slideTitle(s, "The 4-Step Diagnostic Framework", 0.4, 0.2, 9.2, C.aqua); accentLine(s, 1.0); const steps = [ { num:"1", title:"Serum Osmolality", body:"Is this TRUE hypotonic hyponatremia?\nRule out pseudohyponatremia\n(lipemia, paraprotein)\nand hypertonic causes\n(hyperglycemia, mannitol)", color:C.teal }, { num:"2", title:"ECF Volume Status", body:"Hypovolemic / Euvolemic\n/ Hypervolemic\nMost important clinical step\nOrthostatics, JVP, edema,\nBUN/Cr, uric acid", color:"1565C0" }, { num:"3", title:"Urine Osmolality", body:"Is AVP active?\n< 100 = AVP suppressed\n(polydipsia, EAH)\n> 300 = AVP active\n(most clinical hyponatremia)", color:"6A0572" }, { num:"4", title:"Urine Sodium", body:"Renal vs. extra-renal?\nAppropriate vs. not?\n< 20: extra-renal or Na-avid\n> 30: renal wasting or SIADH", color:"B5451B" }, ]; steps.forEach((st, i) => { const x = 0.25 + i * 2.42; s.addShape(pres.ShapeType.rect, { x, y:1.18, w:2.2, h:4.15, fill:{color:st.color}, line:{color:st.color} }); s.addShape(pres.ShapeType.ellipse, { x:x+0.7, y:1.25, w:0.8, h:0.8, fill:{color:C.white}, line:{color:C.white} }); s.addText(st.num, { x:x+0.7, y:1.25, w:0.8, h:0.8, fontSize:20, bold:true, color:st.color, align:"center", valign:"middle", margin:0 }); s.addText("STEP "+st.num, { x, y:2.18, w:2.2, h:0.35, fontSize:10, bold:true, color:C.white, align:"center", valign:"middle", margin:0, charSpacing:3 }); s.addText(st.title, { x, y:2.55, w:2.2, h:0.5, fontSize:13.5, bold:true, color:C.yellow, align:"center", valign:"middle", fontFace:"Calibri" }); s.addText(st.body, { x:x+0.1, y:3.1, w:2.0, h:2.1, fontSize:10.5, color:C.white, fontFace:"Calibri", wrap:true, valign:"top" }); }); s.addText("Combine all 4 steps with clinical context -> diagnosis is almost always apparent", { x:0.4, y:5.4, w:9.2, h:0.35, fontSize:12, italic:true, color:C.gray, align:"center" }); } // ─── SLIDE 5: URINE TEST QUICK REF ──────────────────────────────────────────── { const s = pres.addSlide(); lightSlide(s); tealBar(s, 0, 1.05); sectionTag(s, "LAB KEYS"); slideTitle(s, "Key Urine Tests at a Glance", 0.4, 0.2, 9.2, C.white); s.addShape(pres.ShapeType.rect, { x:0.3, y:1.15, w:9.4, h:0.42, fill:{color:C.navy}, line:{color:C.navy} }); s.addText("URINE OSMOLALITY (Uosm)", { x:0.3, y:1.15, w:9.4, h:0.42, fontSize:13, bold:true, color:C.aqua, align:"center", valign:"middle", margin:0 }); const uosmRows = [ ["< 100 mOsm/kg", "AVP suppressed", "Psychogenic polydipsia, beer potomania, EAH"], ["100 - 300", "Partial suppression", "Mixed picture, solute depletion"], ["> 300 mOsm/kg", "AVP active", "Most clinical hyponatremia"], ["> 400 mOsm/kg", "AVP dominant", "SIADH, severe volume depletion"], ]; uosmRows.forEach((row, i) => { const y = 1.57 + i * 0.5; s.addShape(pres.ShapeType.rect, { x:0.3, y, w:9.4, h:0.49, fill:{color:i%2===0?C.lightBg:C.white}, line:{color:C.teal, pt:0.5} }); s.addText(row[0], { x:0.35, y, w:2.4, h:0.49, fontSize:12, bold:true, color:C.teal, valign:"middle" }); s.addText(row[1], { x:2.8, y, w:2.4, h:0.49, fontSize:12, color:C.navy, valign:"middle" }); s.addText(row[2], { x:5.25, y, w:4.4, h:0.49, fontSize:11, color:C.darkText, valign:"middle", italic:true }); }); s.addShape(pres.ShapeType.rect, { x:0.3, y:3.65, w:9.4, h:0.42, fill:{color:C.teal}, line:{color:C.teal} }); s.addText("URINE SODIUM (UNa)", { x:0.3, y:3.65, w:9.4, h:0.42, fontSize:13, bold:true, color:C.white, align:"center", valign:"middle", margin:0 }); const unaRows = [ ["< 20 mEq/L", "Extra-renal loss / Na-avid state", "Diarrhea/vomiting, CHF, cirrhosis, nephrotic"], ["> 20-30 mEq/L", "Renal Na wasting or SIADH", "Diuretics, adrenal insufficiency, SIADH, CSW"], ]; unaRows.forEach((row, i) => { const y = 4.07 + i * 0.5; s.addShape(pres.ShapeType.rect, { x:0.3, y, w:9.4, h:0.49, fill:{color:i===0?C.lightBg:C.white}, line:{color:C.teal, pt:0.5} }); s.addText(row[0], { x:0.35, y, w:2.4, h:0.49, fontSize:12, bold:true, color:C.teal, valign:"middle" }); s.addText(row[1], { x:2.8, y, w:2.9, h:0.49, fontSize:12, color:C.navy, valign:"middle" }); s.addText(row[2], { x:5.75, y, w:3.9, h:0.49, fontSize:11, color:C.darkText, valign:"middle", italic:true }); }); s.addText("Quick Tip: Urine specific gravity 1.015 -> Uosm approx 15 x 35 = 525 mOsm/L", { x:0.3, y:5.12, w:9.4, h:0.35, fontSize:11, italic:true, color:C.gray, align:"center" }); } // ─── SLIDE 6: THREE VOLUME CATEGORIES ───────────────────────────────────────── { const s = pres.addSlide(); darkSlide(s); sectionTag(s, "CATEGORIES"); slideTitle(s, "Three Volume Categories", 0.4, 0.2, 9.2, C.aqua); accentLine(s, 1.0); const cats = [ { title:"HYPOVOLEMIC", icon:"DOWN Vol", color:C.teal, signs:["Orthostatic hypotension", "Tachycardia, dry MM", "High BUN/Cr, high uric acid"], causes:["Extra-renal: GI losses, burns, sweat (UNa < 20)", "Renal: thiazides, adrenal insufficiency, salt-losing nephropathy (UNa > 20)", "Cerebral salt wasting (CSW)"], tx:"0.9% Normal Saline", }, { title:"EUVOLEMIC", icon:"NORMAL Vol", color:"1565C0", signs:["Normal exam", "No edema, no depletion", "Most common in hospital"], causes:["SIADH (most common)", "Hypothyroidism", "Secondary adrenal insufficiency", "Beer potomania, polydipsia, EAH"], tx:"Fluid restriction +/- urea +/- vaptan", }, { title:"HYPERVOLEMIC", icon:"UP Vol", color:"6A0572", signs:["Peripheral edema", "Ascites, high JVP, S3", "'Effective underfilling'"], causes:["CHF (UNa < 10)", "Cirrhosis (UNa < 10)", "Nephrotic syndrome (UNa < 10)", "Renal failure (UNa > 20)"], tx:"Treat underlying cause, restrict fluids", }, ]; cats.forEach((cat, i) => { const x = 0.22 + i * 3.26; s.addShape(pres.ShapeType.rect, { x, y:1.18, w:3.05, h:4.15, fill:{color:cat.color, transparency:15}, line:{color:cat.color, pt:2} }); s.addShape(pres.ShapeType.rect, { x, y:1.18, w:3.05, h:0.5, fill:{color:cat.color}, line:{color:cat.color} }); s.addText(cat.title, { x, y:1.18, w:3.05, h:0.5, fontSize:13, bold:true, color:C.white, align:"center", valign:"middle", margin:0 }); s.addText("Signs:", { x:x+0.1, y:1.75, w:2.85, h:0.3, fontSize:11, bold:true, color:C.yellow, valign:"middle" }); cat.signs.forEach((sg, j) => { s.addText(" " + sg, { x:x+0.1, y:2.08+j*0.34, w:2.85, h:0.33, fontSize:10.5, color:C.white, fontFace:"Calibri", wrap:true }); }); s.addText("Causes:", { x:x+0.1, y:3.22, w:2.85, h:0.3, fontSize:11, bold:true, color:C.yellow, valign:"middle" }); cat.causes.forEach((c, j) => { s.addText(" " + c, { x:x+0.1, y:3.55+j*0.32, w:2.85, h:0.31, fontSize:9.5, color:C.white, fontFace:"Calibri", wrap:true }); }); }); } // ─── SLIDE 7: SIADH ─────────────────────────────────────────────────────────── { const s = pres.addSlide(); lightSlide(s); tealBar(s, 0, 1.05); sectionTag(s, "SIADH"); slideTitle(s, "SIADH: Most Common Euvolemic Cause", 0.4, 0.2, 9.2, C.white); s.addShape(pres.ShapeType.rect, { x:0.3, y:1.15, w:4.4, h:3.5, fill:{color:C.white}, line:{color:C.teal, pt:2}, shadow:{type:"outer", color:"000000", blur:8, offset:2, angle:135, opacity:0.10} }); s.addShape(pres.ShapeType.rect, { x:0.3, y:1.15, w:4.4, h:0.42, fill:{color:C.teal}, line:{color:C.teal} }); s.addText("Diagnostic Criteria", { x:0.3, y:1.15, w:4.4, h:0.42, fontSize:13, bold:true, color:C.white, align:"center", valign:"middle", margin:0 }); const criteria = [ "Hypotonic hyponatremia (Posm < 275 mOsm/kg)", "Urine osmolality elevated (> 200 mOsm/kg)", "Urine Na > 20 mEq/L", "Clinical euvolemia", "Normal adrenal, renal, cardiac, hepatic, thyroid", "Serum uric acid < 4 mg/dL (hypouricemia)", ]; criteria.forEach((c, i) => { s.addShape(pres.ShapeType.rect, { x:0.3, y:1.57+i*0.38, w:0.38, h:0.34, fill:{color:C.aqua}, line:{color:C.aqua} }); s.addText((i+1).toString(), { x:0.3, y:1.57+i*0.38, w:0.38, h:0.34, fontSize:11, bold:true, color:C.white, align:"center", valign:"middle", margin:0 }); s.addText(c, { x:0.73, y:1.57+i*0.38, w:3.92, h:0.34, fontSize:11, color:C.darkText, valign:"middle" }); }); s.addShape(pres.ShapeType.rect, { x:5.0, y:1.15, w:4.7, h:3.5, fill:{color:C.white}, line:{color:C.navy, pt:1.5} }); s.addShape(pres.ShapeType.rect, { x:5.0, y:1.15, w:4.7, h:0.42, fill:{color:C.navy}, line:{color:C.navy} }); s.addText("Common Causes", { x:5.0, y:1.15, w:4.7, h:0.42, fontSize:13, bold:true, color:C.aqua, align:"center", valign:"middle", margin:0 }); const causes = [ { cat:"CNS:", items:"Meningitis, SAH, stroke, trauma, psychosis" }, { cat:"Pulmonary:", items:"Pneumonia, TB, ARDS, positive-pressure ventilation" }, { cat:"Malignancy:", items:"SCLC (most common, 10-15%), lymphoma, pancreas, bladder" }, { cat:"Drugs:", items:"SSRIs, carbamazepine, cyclophosphamide, NSAIDs, opioids, amiodarone" }, { cat:"Other:", items:"Surgery, pain, nausea, HIV" }, ]; causes.forEach((g, i) => { s.addText([ {text:g.cat+" ", options:{bold:true, color:C.teal, fontSize:11.5}}, {text:g.items, options:{bold:false, color:C.darkText, fontSize:11.5}} ], { x:5.15, y:1.65+i*0.55, w:4.45, h:0.5, valign:"top", wrap:true }); }); s.addShape(pres.ShapeType.rect, { x:0.3, y:4.73, w:9.4, h:0.72, fill:{color:C.yellow, transparency:20}, line:{color:C.yellow, pt:1.5} }); s.addText([ {text:"U/P Electrolyte Ratio: ", options:{bold:true, fontSize:12.5, color:C.navy}}, {text:"(Urine [Na+]+[K+]) / Plasma [Na+] | >1 -> restrict < 500 mL/d | ~1 -> 500-700 mL/d | <1 -> < 1 L/d", options:{fontSize:12, color:C.darkText}}, ], { x:0.3, y:4.73, w:9.4, h:0.72, valign:"middle", align:"center" }); } // ─── SLIDE 8: ODS ───────────────────────────────────────────────────────────── { const s = pres.addSlide(); darkSlide(s); sectionTag(s, "TREATMENT SAFETY"); slideTitle(s, "Osmotic Demyelination Syndrome (ODS)", 0.4, 0.2, 9.2, C.red); accentLine(s, 1.0); s.addShape(pres.ShapeType.rect, { x:0.25, y:1.15, w:4.6, h:4.15, fill:{color:"1C0A0A"}, line:{color:C.red, pt:2} }); s.addShape(pres.ShapeType.rect, { x:0.25, y:1.15, w:4.6, h:0.42, fill:{color:C.red}, line:{color:C.red} }); s.addText("Why It Happens", { x:0.25, y:1.15, w:4.6, h:0.42, fontSize:13, bold:true, color:C.white, align:"center", valign:"middle", margin:0 }); s.addText([ {text:"Rapid correction of chronic hyponatremia\n"}, {text:"Water exits brain cells -> ECF becomes hypertonic\n"}, {text:"Cells that lost organic osmolytes cannot maintain volume\n"}, {text:"Myelin damage -- pons most vulnerable (central pontine myelinolysis)\n"}, {text:"Symptoms appear 2-6 days AFTER rapid correction -- NOT immediately"}, ], { x:0.4, y:1.65, w:4.3, h:2.5, fontSize:11.5, color:C.white, fontFace:"Calibri", valign:"top", wrap:true }); s.addText("Risk Factors:", { x:0.4, y:4.2, w:4.3, h:0.3, fontSize:12, bold:true, color:C.yellow, valign:"middle" }); s.addText("Na < 120 | Duration > 48 h | Hypokalemia | Alcoholism\nCirrhosis | Malnutrition | Beer potomania | Vaptans", { x:0.4, y:4.52, w:4.3, h:0.72, fontSize:11, color:C.white, fontFace:"Calibri", wrap:true }); s.addShape(pres.ShapeType.rect, { x:5.15, y:1.15, w:4.6, h:4.15, fill:{color:"0A1A0A"}, line:{color:C.aqua, pt:2} }); s.addShape(pres.ShapeType.rect, { x:5.15, y:1.15, w:4.6, h:0.42, fill:{color:C.aqua}, line:{color:C.aqua} }); s.addText("Correction Limits & Management", { x:5.15, y:1.15, w:4.6, h:0.42, fontSize:12, bold:true, color:C.navy, align:"center", valign:"middle", margin:0 }); const limits = [["First 24 h","8-10 mEq/L","(up to 12 if acute)"],["First 48 h","18 mEq/L","total limit"]]; limits.forEach((l, i) => { s.addShape(pres.ShapeType.rect, { x:5.25+i*2.2, y:1.65, w:2.0, h:1.2, fill:{color:"1A2A1A"}, line:{color:C.aqua, pt:1.5} }); s.addText(l[0], { x:5.25+i*2.2, y:1.65, w:2.0, h:0.38, fontSize:11, bold:true, color:C.gray, align:"center", valign:"middle" }); s.addText(l[1], { x:5.25+i*2.2, y:2.03, w:2.0, h:0.45, fontSize:18, bold:true, color:C.yellow, align:"center", valign:"middle" }); s.addText(l[2], { x:5.25+i*2.2, y:2.5, w:2.0, h:0.3, fontSize:10, color:C.gray, align:"center", italic:true }); }); s.addText("If Overcorrected:", { x:5.25, y:2.95, w:4.3, h:0.3, fontSize:12, bold:true, color:C.red, valign:"middle" }); s.addText([ {text:"Give 5% dextrose water at 3 mL/kg/h\n"}, {text:"Add DDAVP to stop further free-water excretion\n"}, {text:"Loop diuretics\n"}, {text:"Target: bring Na+ back to safe correction limit"}, ], { x:5.25, y:3.28, w:4.3, h:1.85, fontSize:11.5, color:C.white, fontFace:"Calibri", valign:"top", wrap:true }); s.addShape(pres.ShapeType.rect, { x:0.25, y:5.35, w:9.5, h:0.42, fill:{color:C.red, transparency:20}, line:{color:C.red} }); s.addText("ODS Symptoms (days 2-6 post-correction): Dysarthria Dysphagia Paraparesis Locked-in Seizures Coma", { x:0.25, y:5.35, w:9.5, h:0.42, fontSize:11.5, bold:true, color:C.white, align:"center", valign:"middle", margin:0 }); } // ─── SLIDE 9: TREATMENT ─────────────────────────────────────────────────────── { const s = pres.addSlide(); lightSlide(s); tealBar(s, 0, 1.05); sectionTag(s, "TREATMENT"); slideTitle(s, "Treatment by Cause", 0.4, 0.2, 9.2, C.white); s.addShape(pres.ShapeType.rect, { x:0.3, y:1.15, w:9.4, h:1.5, fill:{color:"FFF3E0"}, line:{color:C.red, pt:2} }); s.addShape(pres.ShapeType.rect, { x:0.3, y:1.15, w:9.4, h:0.42, fill:{color:C.red}, line:{color:C.red} }); s.addText("EMERGENCY: Symptomatic / Seizures / Coma -> 3% Hypertonic NaCl", { x:0.3, y:1.15, w:9.4, h:0.42, fontSize:13, bold:true, color:C.white, align:"center", valign:"middle", margin:0 }); s.addText("150 mL 3% NaCl IV over 20 min -> recheck Na -> repeat up to 3x (450 mL max)\nStop when symptoms resolve OR Na rises 4-6 mEq/L | Limit: 8-12 mEq/L / 24 h", { x:0.5, y:1.6, w:9.0, h:0.96, fontSize:12, color:C.darkText, valign:"middle", wrap:true }); const rows = [ { cause:"Hypovolemic (GI/extra-renal)", tx:"0.9% NaCl -- volume repletion -> AVP suppresses -> aquaresis", color:C.teal }, { cause:"Thiazide-induced", tx:"Stop thiazide, correct K+ (itself raises Na+), consider loop diuretic instead", color:C.teal }, { cause:"Adrenal insufficiency (primary)", tx:"IV hydrocortisone + NS -- draw cortisol first, do not delay", color:C.teal }, { cause:"SIADH", tx:"Fluid restriction (U/P ratio guided) +/- oral Na +/- urea +/- tolvaptan (inpatient start)", color:"1565C0" }, { cause:"Hypothyroidism", tx:"Thyroid hormone (T4) replacement", color:"1565C0" }, { cause:"CHF / Cirrhosis", tx:"Treat underlying cause + fluid restriction + vaptan if refractory", color:"6A0572" }, { cause:"Beer potomania", tx:"0.9% NS + normal diet -- HIGH ODS RISK -- monitor very closely", color:C.red }, ]; rows.forEach((row, i) => { const y = 2.72 + i * 0.41; s.addShape(pres.ShapeType.rect, { x:0.3, y, w:9.4, h:0.4, fill:{color:i%2===0?C.white:C.lightBg}, line:{color:C.teal, pt:0.5} }); s.addShape(pres.ShapeType.rect, { x:0.3, y, w:0.14, h:0.4, fill:{color:row.color}, line:{color:row.color} }); s.addText(row.cause, { x:0.5, y, w:3.0, h:0.4, fontSize:11, bold:true, color:C.navy, valign:"middle" }); s.addText(row.tx, { x:3.55, y, w:6.1, h:0.4, fontSize:10.5, color:C.darkText, valign:"middle", wrap:true }); }); } // ─── SLIDE 10: CASE 1 ───────────────────────────────────────────────────────── { const s = pres.addSlide(); darkSlide(s); sectionTag(s, "CASE 1"); slideTitle(s, "Case 1: The Dehydrated Vomiter", 0.4, 0.2, 9.2, C.yellow); accentLine(s, 1.0); s.addShape(pres.ShapeType.rect, { x:0.25, y:1.15, w:9.5, h:0.9, fill:{color:C.teal, transparency:80}, line:{color:C.teal, pt:1} }); s.addText("67F | 3 days vomiting | BP 95/60 -> 78/50 orthostatic | HR 112 | Dry mucous membranes, skin tenting, no edema", { x:0.4, y:1.18, w:9.2, h:0.82, fontSize:12.5, color:C.white, fontFace:"Calibri", valign:"middle", italic:true, wrap:true }); const labs = [["Na+","124 mEq/L"],["Posm","258 mOsm/kg"],["Uosm","680 mOsm/kg"],["UNa","8 mEq/L"],["BUN","42"],["K+","3.1"]]; labs.forEach((l, i) => { const x = 0.25 + i * 1.6; s.addShape(pres.ShapeType.rect, { x, y:2.18, w:1.45, h:0.72, fill:{color:C.navy, transparency:30}, line:{color:C.aqua, pt:1.5} }); s.addText(l[0], { x, y:2.18, w:1.45, h:0.35, fontSize:11, bold:true, color:C.aqua, align:"center", valign:"middle", margin:0 }); s.addText(l[1], { x, y:2.53, w:1.45, h:0.37, fontSize:12, bold:true, color:C.yellow, align:"center", valign:"middle", margin:0 }); }); const analysis = [ ["Step 1 -- Posm 258","TRUE hypotonic hyponatremia confirmed"], ["Step 2 -- Volume","HYPOVOLEMIC -- orthostatics, tachycardia, high BUN"], ["Step 3 -- Uosm 680","AVP very active (kidney concentrating to preserve volume)"], ["Step 4 -- UNa 8","EXTRA-RENAL Na loss -- kidneys avid for sodium (GI losses)"], ]; analysis.forEach((st, i) => { const x = 0.25 + (i%2)*4.75; const y = 3.05 + Math.floor(i/2)*0.95; s.addShape(pres.ShapeType.rect, { x, y, w:4.45, h:0.85, fill:{color:"0A1A2A"}, line:{color:C.teal, pt:1} }); s.addText(st[0], { x:x+0.1, y, w:4.25, h:0.38, fontSize:11, bold:true, color:C.aqua, valign:"middle" }); s.addText(st[1], { x:x+0.1, y:y+0.38, w:4.25, h:0.4, fontSize:11, color:C.white, valign:"middle", wrap:true }); }); s.addShape(pres.ShapeType.rect, { x:0.25, y:5.02, w:9.5, h:0.42, fill:{color:C.teal}, line:{color:C.teal} }); s.addText("Dx: Hypovolemic hyponatremia (GI losses) | Rx: 0.9% NaCl + correct K+ | Monitor Na q4-6h", { x:0.25, y:5.02, w:9.5, h:0.42, fontSize:12.5, bold:true, color:C.white, align:"center", valign:"middle", margin:0 }); } // ─── SLIDE 11: CASE 2 ───────────────────────────────────────────────────────── { const s = pres.addSlide(); lightSlide(s); tealBar(s, 0, 1.05); sectionTag(s, "CASE 2"); slideTitle(s, "Case 2: SIADH in Small Cell Lung Cancer", 0.4, 0.2, 9.2, C.white); s.addShape(pres.ShapeType.rect, { x:0.3, y:1.15, w:9.4, h:0.78, fill:{color:C.navy, transparency:85}, line:{color:C.navy, pt:1} }); s.addText("52M | SCLC | 1 week: fatigue, confusion, headache | No edema, no orthostasis", { x:0.5, y:1.2, w:9.0, h:0.68, fontSize:12.5, color:C.darkText, fontFace:"Calibri", valign:"middle", italic:true }); const labs = [["Na+","118 mEq/L"],["Posm","242 mOsm/kg"],["Uosm","520 mOsm/kg"],["UNa","65 mEq/L"],["Uric Acid","2.8 mg/dL"],["K+","3.9"]]; labs.forEach((l, i) => { const x = 0.3 + i * 1.6; s.addShape(pres.ShapeType.rect, { x, y:2.05, w:1.45, h:0.72, fill:{color:C.teal, transparency:85}, line:{color:C.teal, pt:1.5} }); s.addText(l[0], { x, y:2.05, w:1.45, h:0.35, fontSize:11, bold:true, color:C.teal, align:"center", valign:"middle", margin:0 }); s.addText(l[1], { x, y:2.4, w:1.45, h:0.37, fontSize:12, bold:true, color:C.navy, align:"center", valign:"middle", margin:0 }); }); const steps = [ "Posm 242 -> true hypotonic hyponatremia", "Euvolemic -- no edema, no depletion signs", "Uosm 520 -> AVP active despite hyponatremia (inappropriate!)", "UNa 65 -> kidney NOT retaining sodium", "Uric acid 2.8 mg/dL -> hypouricemia = SIADH physiology", "SCLC context -> paraneoplastic ectopic AVP production", ]; steps.forEach((a, i) => { const x = 0.3 + (i%2)*4.75; const y = 2.88 + Math.floor(i/2)*0.55; s.addShape(pres.ShapeType.rect, { x, y, w:0.34, h:0.5, fill:{color:C.teal}, line:{color:C.teal} }); s.addText((i+1).toString(), { x, y, w:0.34, h:0.5, fontSize:11, bold:true, color:C.white, align:"center", valign:"middle", margin:0 }); s.addText(a, { x:x+0.38, y, w:4.28, h:0.5, fontSize:11.5, color:C.darkText, valign:"middle", wrap:true }); }); s.addShape(pres.ShapeType.rect, { x:0.3, y:5.55, w:9.4, h:0.42, fill:{color:C.navy}, line:{color:C.navy} }); s.addText("Dx: SIADH paraneoplastic (SCLC) | Rx: Fluid restriction < 1 L/d +/- urea +/- tolvaptan | Treat SCLC", { x:0.3, y:5.55, w:9.4, h:0.42, fontSize:11.5, bold:true, color:C.aqua, align:"center", valign:"middle", margin:0 }); } // ─── SLIDE 12: CASES 3 & 4 ──────────────────────────────────────────────────── { const s = pres.addSlide(); darkSlide(s); sectionTag(s, "CASES 3 & 4"); slideTitle(s, "More Clinical Cases", 0.4, 0.2, 9.2, C.aqua); accentLine(s, 1.0); // Case 3 s.addShape(pres.ShapeType.rect, { x:0.25, y:1.15, w:4.6, h:4.55, fill:{color:"0A1520"}, line:{color:C.teal, pt:2} }); s.addShape(pres.ShapeType.rect, { x:0.25, y:1.15, w:4.6, h:0.42, fill:{color:C.teal}, line:{color:C.teal} }); s.addText("Case 3 - Marathon Runner (EAH)", { x:0.25, y:1.15, w:4.6, h:0.42, fontSize:12, bold:true, color:C.white, align:"center", valign:"middle", margin:0 }); s.addText("29F, collapses post-marathon, seizing\nDrank water continuously, gained weight during race\nNa 112 | Posm 228 | Uosm 68 | UNa 12", { x:0.4, y:1.65, w:4.3, h:0.9, fontSize:11, color:C.gray, fontFace:"Calibri", italic:true, wrap:true }); s.addText([ {text:"Key Clue: Uosm < 100 -> AVP is SUPPRESSED\n", options:{bold:true, color:C.yellow}}, {text:"-> Pure water intoxication (not SIADH)\n"}, {text:"-> ACUTE onset (< 24 h) = high neurologic risk\n"}, {text:"-> Weight gain during race = excessive free water intake\n"}, {text:"-> 44% of EAH cases also have SIADH component"}, ], { x:0.4, y:2.62, w:4.3, h:1.6, fontSize:11.5, color:C.white, fontFace:"Calibri", wrap:true, valign:"top" }); s.addShape(pres.ShapeType.rect, { x:0.25, y:4.28, w:4.6, h:0.56, fill:{color:C.red, transparency:20}, line:{color:C.red} }); s.addText("Rx: 150 mL 3% NaCl IV stat (acute - ODS risk low)\nRepeat up to 3x max -- stop when seizures resolve", { x:0.35, y:4.30, w:4.4, h:0.52, fontSize:11, bold:true, color:C.white, fontFace:"Calibri", wrap:true }); // Case 4 s.addShape(pres.ShapeType.rect, { x:5.15, y:1.15, w:4.6, h:4.55, fill:{color:"100A20"}, line:{color:C.yellow, pt:2} }); s.addShape(pres.ShapeType.rect, { x:5.15, y:1.15, w:4.6, h:0.42, fill:{color:"6A0572"}, line:{color:"6A0572"} }); s.addText("Case 4 - Thiazide Mimic of SIADH", { x:5.15, y:1.15, w:4.6, h:0.42, fontSize:12, bold:true, color:C.white, align:"center", valign:"middle", margin:0 }); s.addText("72F on HCTZ x 3 weeks for HTN\nWeakness, mild confusion, no edema\nNa 122 | Posm 256 | Uosm 380 | UNa 45 | K+ 2.8", { x:5.3, y:1.65, w:4.3, h:0.9, fontSize:11, color:C.gray, fontFace:"Calibri", italic:true, wrap:true }); s.addText([ {text:"Looks exactly like SIADH but...\n", options:{bold:true, color:C.yellow}}, {text:"Started thiazide 3 weeks ago\n"}, {text:"Hypokalemia (K+ 2.8) -- key clue! Few other hyponatremia causes also cause hypokalemia\n"}, {text:"Thiazide blocks DCT -> impairs diluting segment + volume depletion -> AVP rises\n"}, {text:"Do NOT diagnose SIADH until 1-2 weeks after stopping thiazide"}, ], { x:5.3, y:2.62, w:4.3, h:1.75, fontSize:11, color:C.white, fontFace:"Calibri", wrap:true, valign:"top" }); s.addShape(pres.ShapeType.rect, { x:5.15, y:4.28, w:4.6, h:0.56, fill:{color:C.yellow, transparency:30}, line:{color:C.yellow} }); s.addText("Rx: Stop HCTZ | Correct K+ (KCl itself raises Na+) | 0.9% NS if symptomatic | Monitor closely", { x:5.25, y:4.30, w:4.4, h:0.52, fontSize:11, bold:true, color:C.navy, fontFace:"Calibri", wrap:true }); } // ─── SLIDE 13: MASTER TABLE ─────────────────────────────────────────────────── { const s = pres.addSlide(); lightSlide(s); tealBar(s, 0, 1.05); sectionTag(s, "SUMMARY TABLE"); slideTitle(s, "High-Yield Summary Table", 0.4, 0.2, 9.2, C.white); const hdr = ["Condition","Vol","Uosm","UNa","Key Clue","Treatment"]; const hdrW = [2.0, 0.7, 0.75, 0.7, 2.2, 3.35]; let cx = 0.18; hdr.forEach((h, i) => { s.addShape(pres.ShapeType.rect, { x:cx, y:1.12, w:hdrW[i], h:0.38, fill:{color:C.navy}, line:{color:C.navy} }); s.addText(h, { x:cx, y:1.12, w:hdrW[i], h:0.38, fontSize:10.5, bold:true, color:C.aqua, align:"center", valign:"middle", margin:0 }); cx += hdrW[i]; }); const rows = [ ["GI / Extra-renal loss","Down","High","< 20","Orthostasis, vomiting","0.9% NS"], ["Thiazide diuretic","Down/Eu","High","> 20","Hypokalemia","Stop drug, correct K+"], ["Adrenal insufficiency","Down","High",">> 20","Hyperkalemia, pigmentation","Hydrocortisone + NS"], ["Cerebral salt wasting","Down","High","> 20","CNS pathology (SAH)","Na+ + volume"], ["SIADH","Eu","> 200","> 30","Hypouricemia, exclusion","Fluid restrict +/- urea/vaptan"], ["Hypothyroidism","Eu","Var","Var","High TSH, myxedema","T4 replacement"], ["Beer potomania","Eu","< 200","< 20","Alcoholism, low solute","NS + diet -- HIGH ODS risk!"], ["Psychogenic polydipsia","Eu","< 100","Low","Psych hx, schizophrenia","Fluid restriction"], ["EAH (exercise)","Eu","< 100","Low","Post-race, weight gain","3% NaCl if severe (acute)"], ["CHF / Cirrhosis","Up","High","< 10","Edema, ascites, high BNP","Treat cause, restrict fluids"], ["Renal failure","Up","Var","> 20","High Cr, high K+","Dialysis"], ]; const rH = 0.37; rows.forEach((row, ri) => { let rx = 0.18; hdrW.forEach((w, ci) => { const bg = ri % 2 === 0 ? C.white : C.lightBg; const vCol = row[1]==="Down" ? C.teal : row[1]==="Up" ? "6A0572" : "1565C0"; s.addShape(pres.ShapeType.rect, { x:rx, y:1.5+ri*rH, w, h:rH, fill:{color:bg}, line:{color:C.teal, pt:0.5} }); s.addText(row[ci], { x:rx, y:1.5+ri*rH, w, h:rH, fontSize: ci===5 ? 9 : 10, bold: ci===0 || ci===1, color: ci===1 ? vCol : (ci===4 ? C.teal : C.darkText), align: ci===0 ? "left" : "center", valign:"middle", wrap:true, margin: ci===0 ? [0,0,0,4] : 0, }); rx += w; }); }); } // ─── SLIDE 14: KEY TAKEAWAYS ────────────────────────────────────────────────── { const s = pres.addSlide(); darkSlide(s); s.addShape(pres.ShapeType.rect, { x:0, y:0, w:0.18, h:"100%", fill:{color:C.aqua}, line:{color:C.aqua} }); s.addShape(pres.ShapeType.ellipse, { x:7.2, y:-0.8, w:4, h:4, fill:{color:C.teal, transparency:80}, line:{color:C.teal, transparency:80} }); s.addText("Key Takeaways", { x:0.5, y:0.3, w:9, h:0.6, fontSize:30, bold:true, color:C.aqua, fontFace:"Calibri" }); accentLine(s, 1.0); const takes = [ ["1","Serum [Na+] reflects water balance, not total body Na+ -- volume status is the critical first clinical step"], ["2","Always exclude pseudohyponatremia (check measured Posm) and hypertonic causes (glucose) first"], ["3","Uosm < 100 = AVP suppressed -> polydipsia or EAH. Most other hyponatremia has Uosm > 100"], ["4","UNa < 20 with hypovolemia = extra-renal loss. High UNa despite low [Na+] = SIADH or renal Na+ wasting"], ["5","SIADH is a diagnosis of exclusion -- rule out hypothyroidism, adrenal insufficiency, diuretics first"], ["6","Correction limit: 8-10 mEq/L / 24 h in chronic hyponatremia -- exceeding this causes ODS"], ["7","Symptomatic acute hyponatremia -> 3% NaCl bolus 150 mL over 20 min, repeat up to 3x"], ["8","Hypokalemia correction itself raises plasma [Na+] -- watch for inadvertent overcorrection"], ]; takes.forEach((t, i) => { const y = 1.18 + i * 0.5; s.addShape(pres.ShapeType.ellipse, { x:0.45, y:y+0.08, w:0.34, h:0.34, fill:{color:C.teal}, line:{color:C.teal} }); s.addText(t[0], { x:0.45, y:y+0.08, w:0.34, h:0.34, fontSize:11, bold:true, color:C.white, align:"center", valign:"middle", margin:0 }); s.addText(t[1], { x:0.9, y, w:8.8, h:0.48, fontSize:12.5, color:C.white, fontFace:"Calibri", valign:"middle", wrap:true }); }); s.addText("Sources: Harrison's 22E | Brenner & Rector | Tintinalli's EM | NKF Primer | Symptom to Diagnosis 4E", { x:0.5, y:5.25, w:9, h:0.3, fontSize:9.5, color:C.gray, fontFace:"Calibri", italic:true }); } // ─── WRITE ──────────────────────────────────────────────────────────────────── pres.writeFile({ fileName: "/home/daytona/workspace/hyponatremia-ppt/Hyponatremia_Evaluation.pptx" }) .then(() => console.log("Done: Hyponatremia_Evaluation.pptx")) .catch(err => { console.error("Error:", err); process.exit(1); }); ENDOFSCRIPT echo "Script written successfully"
cd /home/daytona/workspace/hyponatremia-ppt && node build.js 2>&1
ls -lh /home/daytona/workspace/hyponatremia-ppt/Hyponatremia_Evaluation.pptx
Hyponatremia Evaluation
Presentation · PPTX
| Slide | Content |
|---|---|
| 1 | Title slide (dark navy + aqua theme) |
| 2 | Definition & Epidemiology - 4 stat cards |
| 3 | Physiology - why hyponatremia happens |
| 4 | The 4-Step Diagnostic Framework |
| 5 | Urine Osmolality + Urine Sodium quick reference |
| 6 | Three Volume Categories (hypo/eu/hyper) |
| 7 | SIADH deep dive - criteria + causes + U/P ratio |
| 8 | ODS - mechanism, limits, treatment if overcorrected |
| 9 | Treatment by cause (including emergency 3% NaCl protocol) |
| 10 | Clinical Case 1: Dehydrated vomiter (hypovolemic) |
| 11 | Clinical Case 2: SIADH in SCLC |
| 12 | Clinical Cases 3 & 4: Marathon runner (EAH) + Thiazide pitfall |
| 13 | High-yield summary table - all 11 conditions |
| 14 | 8 key takeaways |