All about usg with images basic
basic ultrasound USG physics principles B-mode Doppler image formation 2024
USG ultrasound transducer types linear curvilinear phased array applications clinical
ultrasound echogenicity hyperechoic hypoechoic anechoic artifacts acoustic shadowing posterior enhancement
ultrasound B-mode M-mode echogenicity anechoic hyperechoic hypoechoic diagram clinical examples
Ultrasonography (USG) - A Comprehensive Basics Guide
1. What Is Ultrasound?
| Term | Definition |
|---|---|
| Frequency | Cycles per second (Hz). Clinical USG uses 1-20 MHz |
| Wavelength | Distance per cycle. Higher frequency = shorter wavelength = better resolution |
| Propagation speed | ~1540 m/s in soft tissue (varies by medium) |
| Impedance | Resistance of a medium to sound propagation (density × velocity) |
| Attenuation | Loss of sound energy as waves travel deeper into tissue |
- High frequency (7-15 MHz) = excellent resolution, but shallow penetration (superficial structures)
- Low frequency (2-5 MHz) = deeper penetration, lower resolution (deep structures: liver, kidney)
2. The Piezoelectric Effect - How Images Are Made
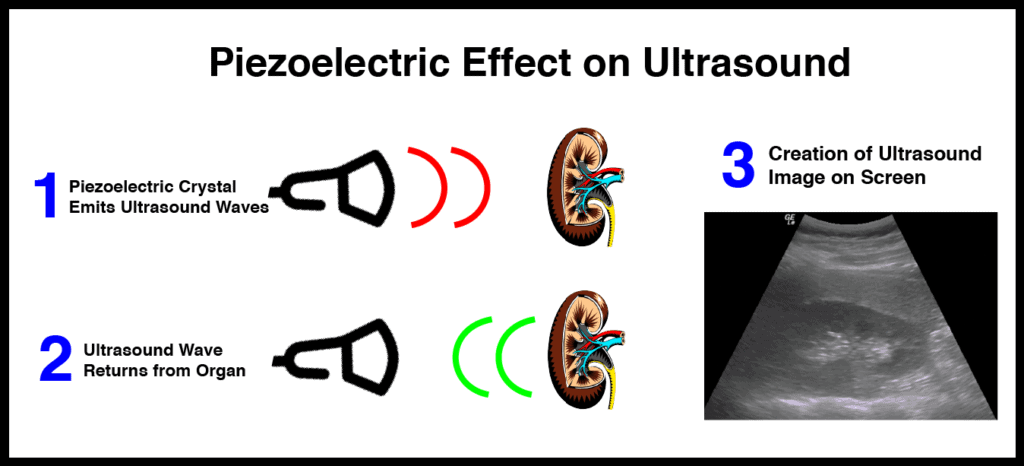
The cycle is: Transmit brief pulse → Switch to receive mode → Detect returning echoes → Calculate depth from time of flight → Build image pixel by pixel
3. Internal Structure of the Transducer
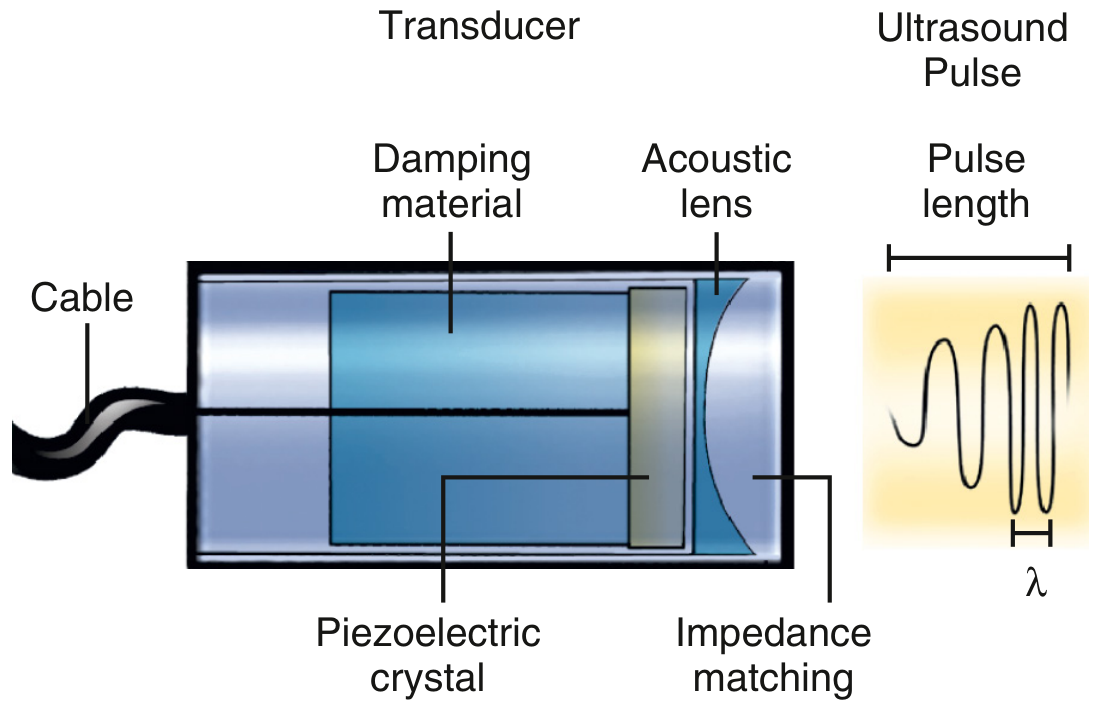
- Piezoelectric crystal - generates and receives sound waves
- Damping material - shortens pulse length, improves axial resolution
- Acoustic lens - focuses the beam
- Impedance matching layer - reduces reflection at skin interface; coupling gel also helps here
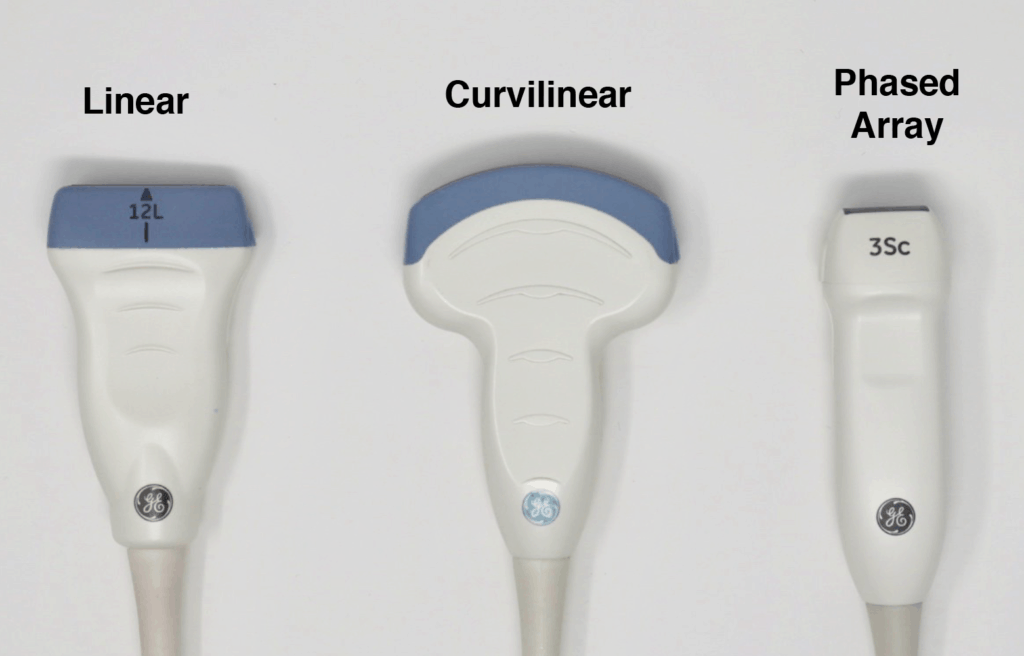
4. Types of Transducers (Probes)

| Probe Type | Frequency | Footprint | Best For |
|---|---|---|---|
| Linear (High-frequency) | 5-15 MHz | Wide, flat | Superficial: thyroid, vessels, breast, tendons, nerves, vascular access |
| Curvilinear (Convex) | 2-5 MHz | Curved, wide | Deep abdominal/pelvic organs: liver, kidney, OB |
| Phased Array (Sector) | 2-5 MHz | Small footprint | Cardiac (echocardiography), intercostal windows |
| Endocavity | 5-10 MHz | Inserted internally | Transvaginal, transrectal |
| Microconvex | 4-8 MHz | Small curved | Neonatal head, emergency point-of-care |
5. Imaging Modes
A-Mode (Amplitude Mode)
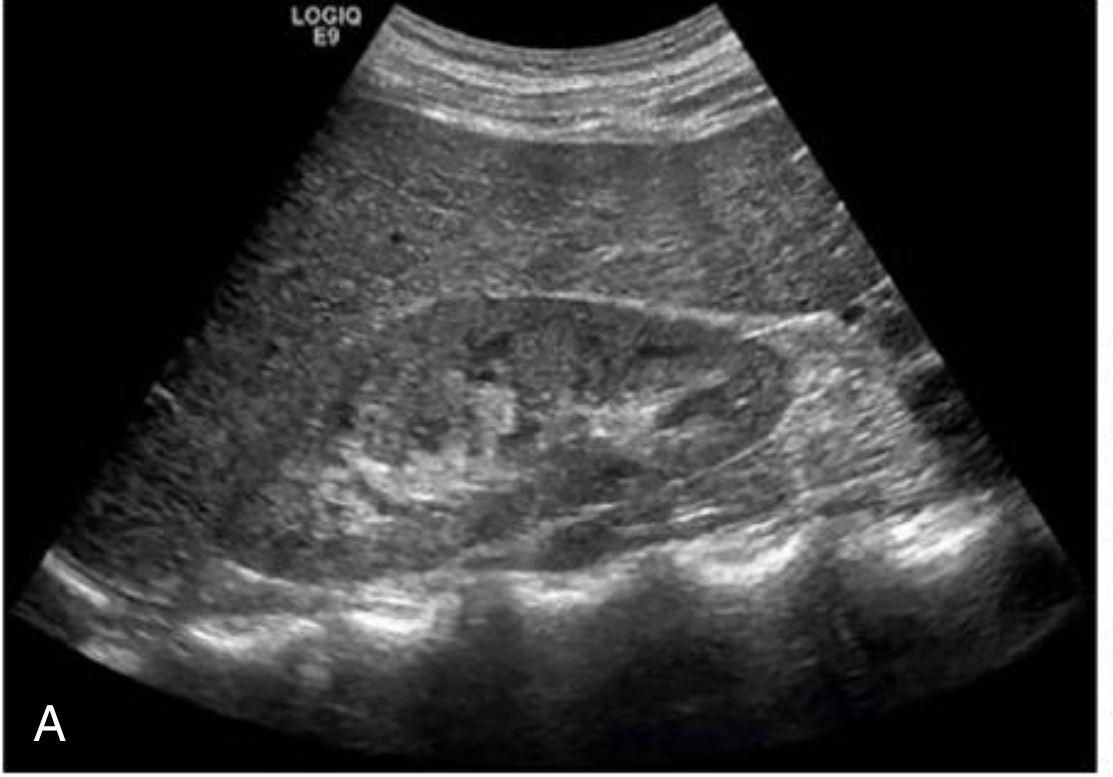
B-Mode (Brightness Mode) - The Standard
M-Mode (Motion Mode)
- Measure IVC diameter and respiratory variation (volume status)
- Assess cardiac valve excursion
- Detect pleural sliding in lung USG
Doppler Modes
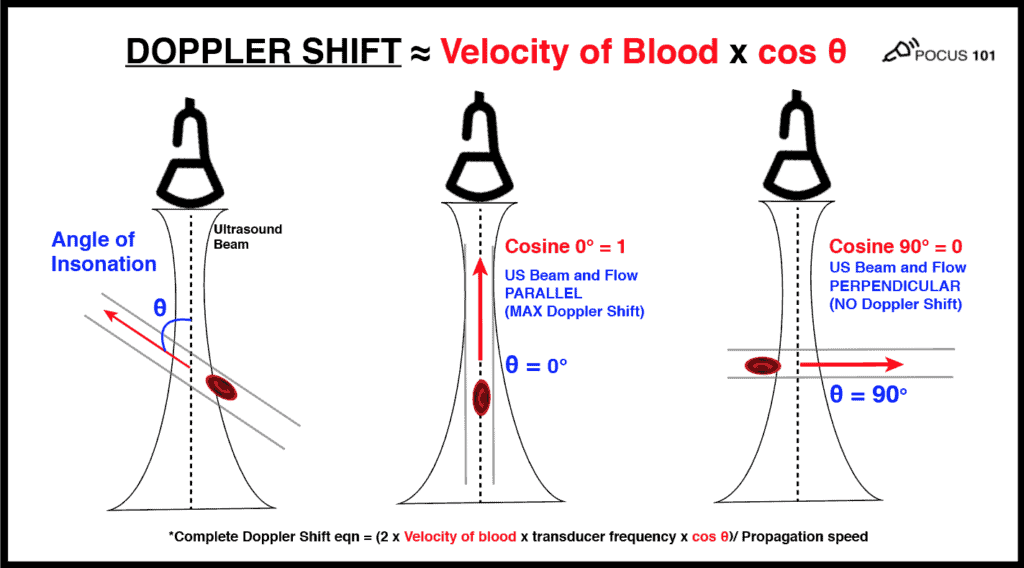
6. Doppler Types
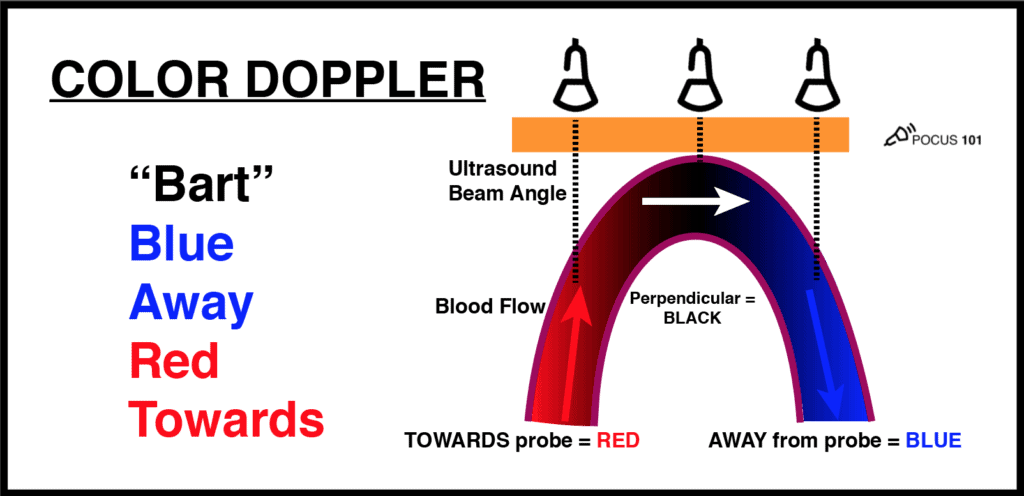
Color Doppler
- Blue Away, Red Towards (relative to probe)
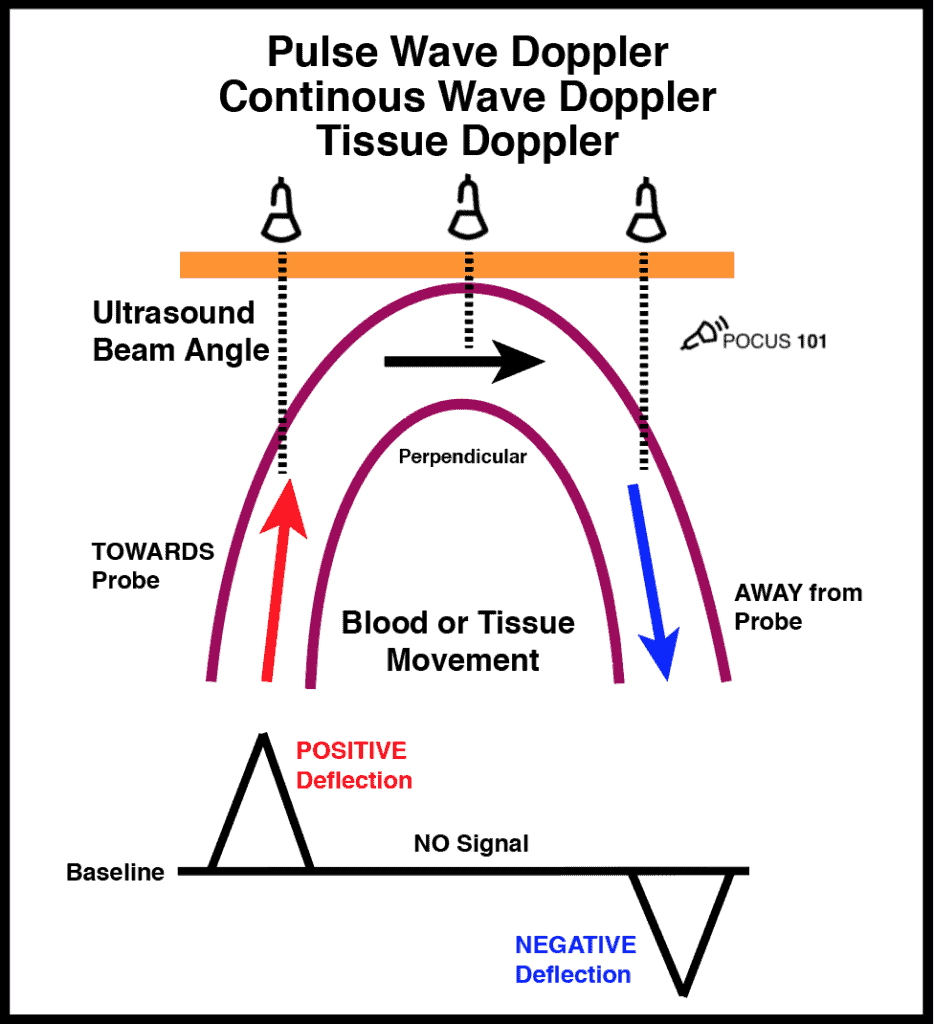
Pulsed Wave (PW) Doppler
Continuous Wave (CW) Doppler
Power Doppler
7. Echogenicity - How Tissues Appear
| Term | Appearance | Examples |
|---|---|---|
| Anechoic | Black (no echoes) | Fluid: urine in bladder, bile, blood in vessels, cysts, effusions |
| Hypoechoic | Darker gray than reference | Lymph nodes, muscle, thyroid adenoma, most solid tumors |
| Isoechoic | Same brightness as reference tissue | Normal thyroid vs. some nodules |
| Hyperechoic | Brighter/whiter than reference | Fat, renal sinus, gallstone, bone, bowel gas |
| Echogenic | Bright reflector (general term) | Air, calcium, foreign bodies |
8. Common USG Artifacts
| Artifact | Appearance | Cause | Clinical Use |
|---|---|---|---|
| Acoustic shadowing | Dark stripe posterior to a bright structure | Strong reflector/attenuator (stone, bone, gas) blocks deeper transmission | Identifies gallstones, renal calculi, calcifications |
| Posterior acoustic enhancement | Brighter area deep to a fluid collection | Fluid attenuates sound less than surrounding tissue | Confirms cystic vs. solid nature |
| Reverberation | Equally spaced parallel lines | Sound bouncing between two strong reflectors | Seen with metallic objects, near-field artifacts |
| A-lines (lung) | Horizontal lines parallel to pleural line | Reverberation at air-tissue interface | Normal lung, pneumothorax |
| B-lines (comet-tail lung) | Vertical hyperechoic lines from pleural line to screen edge | Fluid-thickened subpleural interlobular septa | Pulmonary edema, interstitial lung disease |
| Mirror artifact | Duplicate image on other side of strong reflector | Reflection at diaphragm | Pseudomasses below/above diaphragm |
| Aliasing | Mosaic color wrap-around in Doppler | Velocity exceeds Nyquist limit in PW Doppler | Sign of high-velocity flow |
9. Image Optimization Controls
| Control | Function |
|---|---|
| Gain | Overall brightness of the image. Too much = noise; too little = dark |
| TGC (Time Gain Compensation) | Depth-selective gain to compensate for attenuation |
| Depth | Adjusts how deep the image shows |
| Focus | Sets the focal zone for best lateral resolution |
| Frequency | On broadband probes, switch to higher frequency for better superficial detail |
| Harmonic imaging | Uses tissue harmonics at double the transmitted frequency - reduces noise/clutter |
10. Safety: ALARA Principle
- Thermal effects - heating of tissue (especially bone)
- Mechanical effects (cavitation) - gas bubble formation
- Thermal Index (TI) - estimated temperature rise
- Mechanical Index (MI) - risk of cavitation
11. Clinical Applications at a Glance
| System | What USG Shows |
|---|---|
| Abdomen | Liver, gallbladder stones/wall, bile ducts, pancreas, spleen, ascites |
| Kidney/Urinary | Hydronephrosis, stones, cysts, masses, cortical thickness |
| Cardiac (Echo) | Chambers, valves, pericardial effusion, wall motion |
| Obstetric | Fetal biometry, placenta, amniotic fluid, fetal heart |
| Vascular | DVT, carotid stenosis, AAA, portal hypertension |
| Thyroid/Neck | Nodules (TIRADS), lymph nodes, parathyroid |
| Lung (POCUS) | Pneumothorax (A-lines only), pulmonary edema (B-lines), effusion |
| MSK | Tendons (rotator cuff tears), joints (effusion), nerves |
| POCUS/EM | FAST exam (trauma), volume status (IVC), cardiac arrest |
12. Advantages and Limitations
- No ionizing radiation (safe in pregnancy, pediatrics)
- Real-time imaging
- Portable, bedside use (POCUS)
- Doppler for vascular assessment
- Guides procedures (biopsy, drainage, vascular access) - significantly lowers complication rates
- Relatively inexpensive
- Operator-dependent (significant skill required)
- Poor through gas (bowel, lungs under normal conditions) and bone
- Limited by body habitus (obesity reduces penetration)
- Limited field of view compared to CT/MRI
- Cannot penetrate deep calcifications
In pregnancy usg basic with images all important things
obstetric ultrasound basics first second third trimester fetal biometry anomaly scan 2024
pregnancy ultrasound first trimester gestational sac yolk sac crown rump length CRL images nuchal translucency
second trimester anomaly scan 18-20 weeks fetal biometry BPD HC AC FL placenta AFI images
pregnancy USG nuchal translucency NT scan ectopic pregnancy biophysical profile Doppler umbilical artery images
placenta previa types grades ultrasound image umbilical artery Doppler waveform IUGR normal abnormal
Obstetric Ultrasound (USG) in Pregnancy - Complete Basics Guide
Why USG in Pregnancy?
Routine Scans in Pregnancy - Overview
| Trimester | Weeks | Scan Name | Primary Purpose |
|---|---|---|---|
| First | 6-10 | Early pregnancy / viability scan | Confirm IUP, cardiac activity, number |
| First | 11-14 | Dating + NT scan | Gestational age, NT, early anomaly |
| Second | 18-20 | Anomaly scan / TIFFA | Fetal anatomy, biometry, placenta |
| Third | 28-32 | Growth scan | Growth, AFI, presentation, Doppler |
| Third | 36-40 | Term scan | Presentation, EFW, AFI, placenta |
FIRST TRIMESTER SCAN (6-14 Weeks)
Transabdominal vs. Transvaginal
- Gestational sac: 4.5 weeks (TVS) / ~5.5 weeks (TAS)
- Yolk sac: 5.5 weeks (TVS)
- Fetal pole: 6.0 weeks (TVS)
- Cardiac activity: detected when CRL ≥ 5 mm on TVS
Normal Early Pregnancy Progression
| Gestational Age | Sonographic Finding |
|---|---|
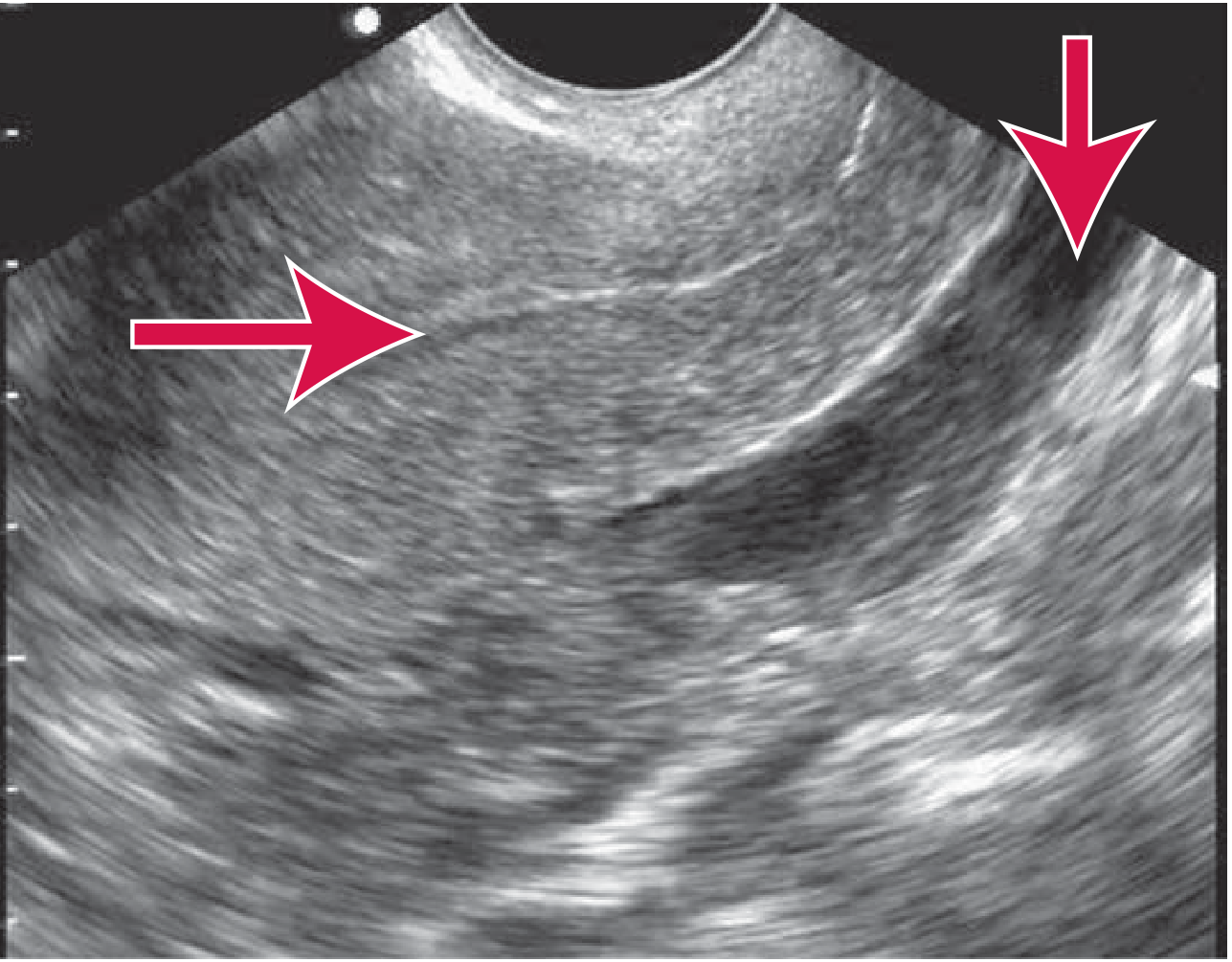
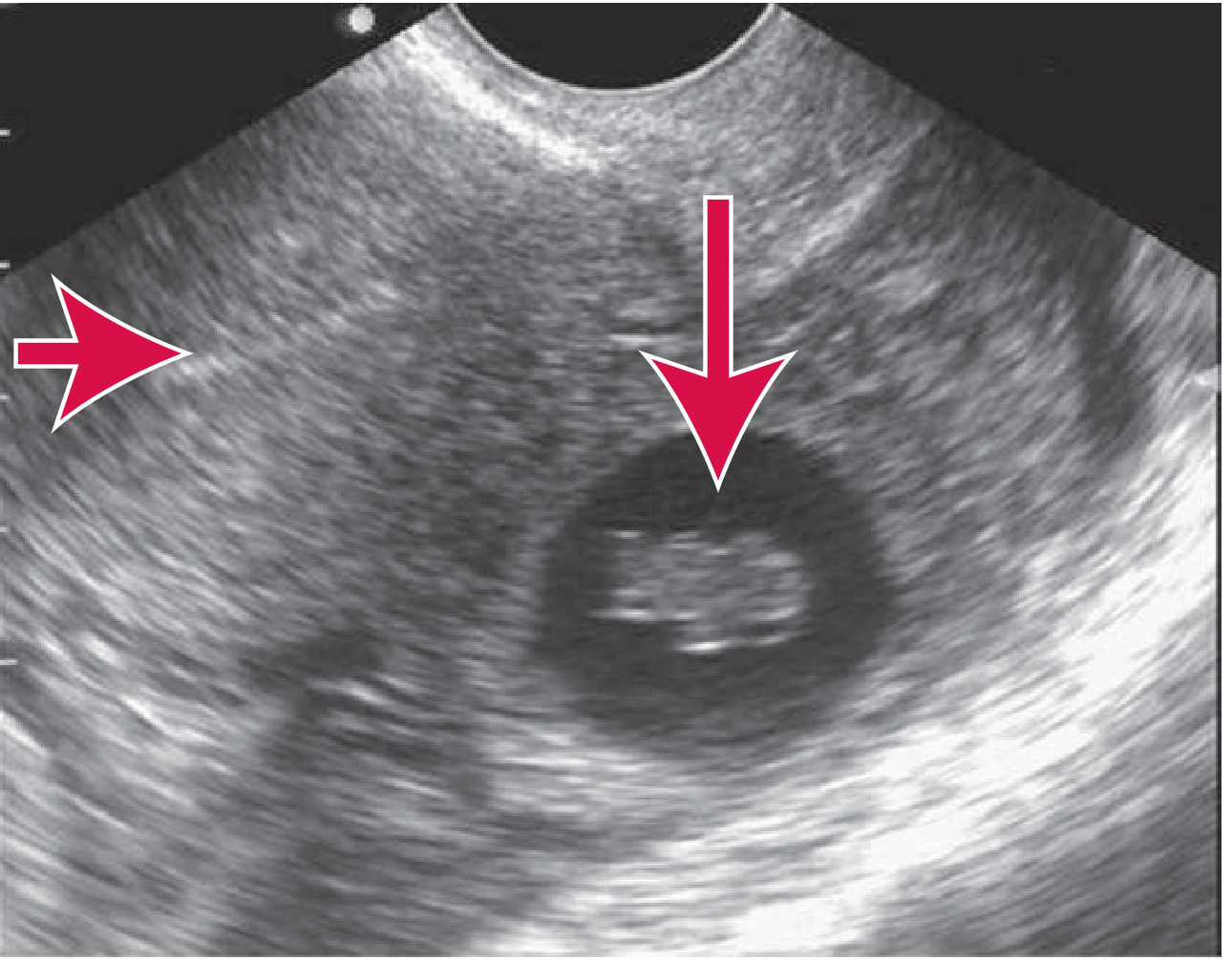
| 4-5 weeks | Gestational sac (anechoic ring in uterine cavity) |
| 5-5.5 weeks | Yolk sac appears within sac |
| 6 weeks | Fetal pole visible, cardiac activity seen |
| 7-8 weeks | Embryonic movement, limb buds |
| 10-13 weeks | Fetal anatomy begins to be visible |
What to Report in First Trimester
- Intrauterine pregnancy confirmed? (location - rule out ectopic)
- Number of gestational sacs / embryos
- Cardiac activity - present or absent
- Gestational age (CRL most accurate)
- Uterus, adnexae (any masses/cysts)
- NT measurement at 11-14 weeks
GESTATIONAL AGE DATING - Key Measurements
Dating Parameters by Gestational Age
| Weeks | Best Parameter | Comment |
|---|---|---|
| 7-10 wks | GS (gestational sac) + CRL average | |
| 11-14 wks | CRL (most accurate) | ± 5 days accuracy |
| 15-28 wks | BPD most accurate; + HC, FL, AC | ± 1 week |
| After 28 wks | Average of BPD, HC, FL, AC | ± 2-3 weeks accuracy |
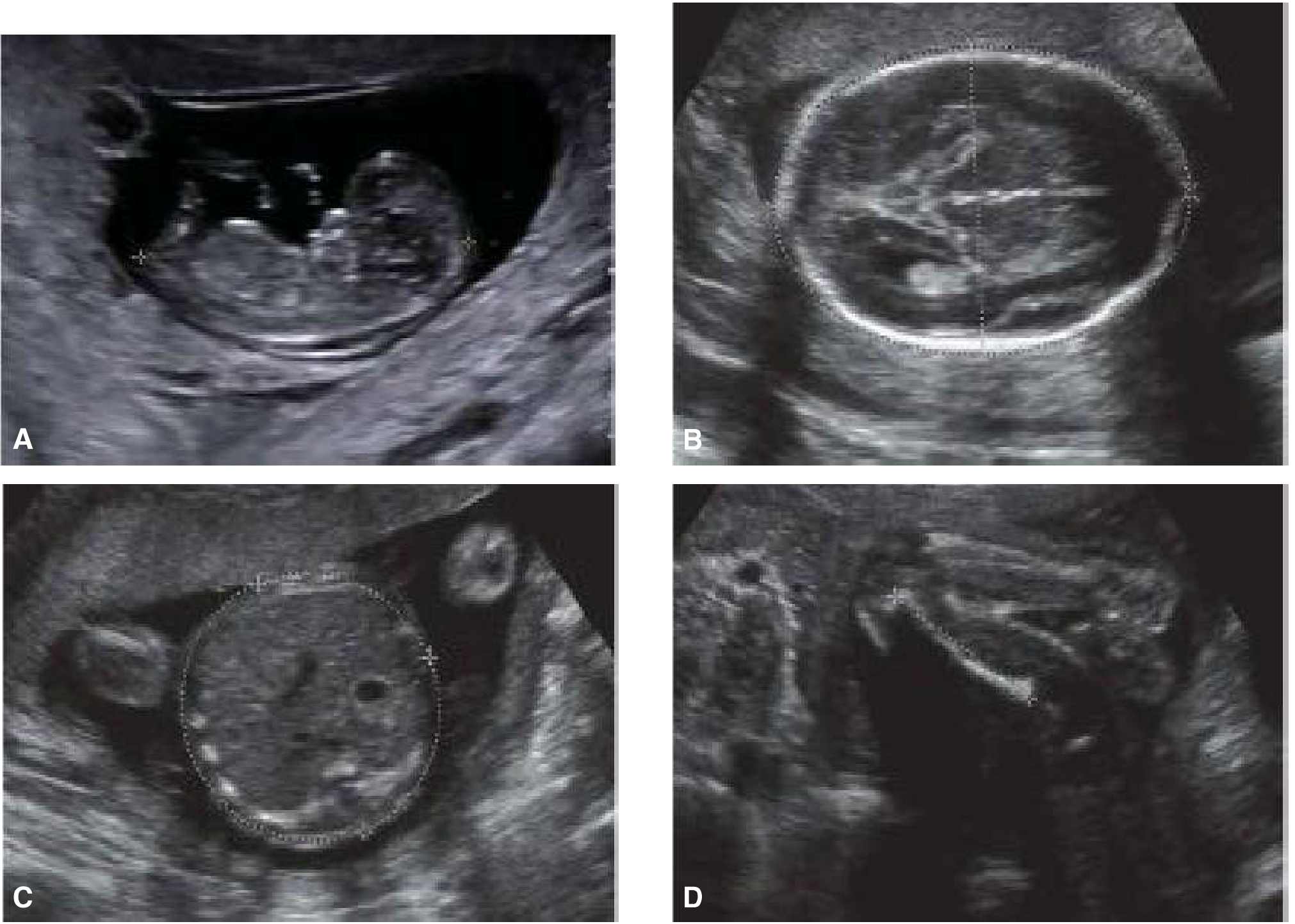
CRL - Crown Rump Length
- Measured from top of head to bottom of rump (NOT legs)
- Most accurate dating parameter in the first trimester
- Performed at 11-14 weeks

BPD - Biparietal Diameter
- Plane: Transverse cross-section at level of thalami
- Midline falx cerebri interrupted by cavum septi pellucidi
- Measurement: Outer table of proximal parietal bone to inner table of distal parietal bone
- No cerebellum visible in this plane
HC - Head Circumference
- Same plane as BPD
- Trace outer edges of cranial bones with ellipse
- Formula: HC = 1.62 × (BPD + OFD)
- More reliable than BPD alone in dolichocephaly/brachycephaly
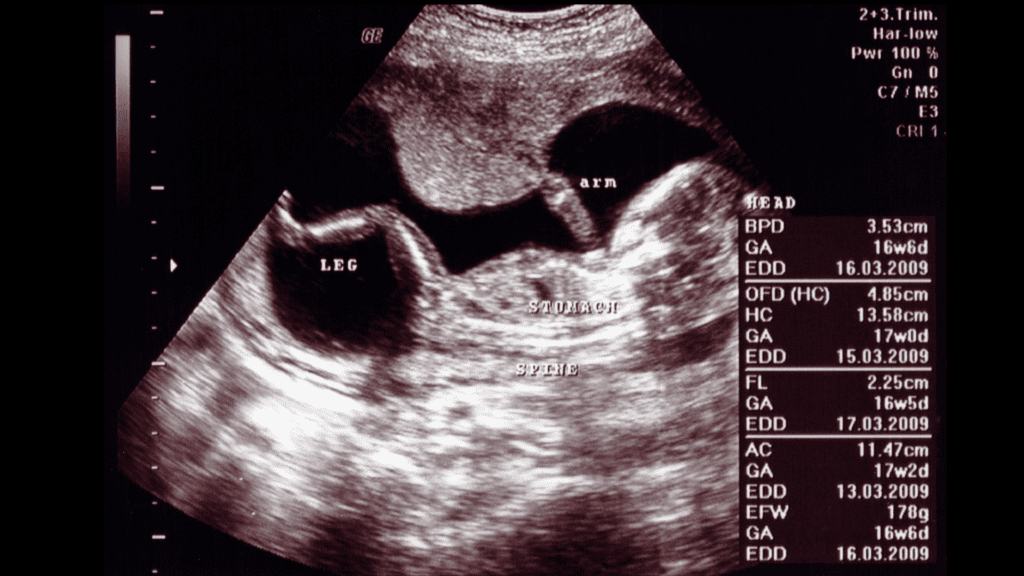
AC - Abdominal Circumference
- Plane: Transverse at level of portal sinus
- Must show: Stomach bubble + umbilical vein (at portal sinus) - no kidneys visible
- Formula: AC = 1.57 × (LAD + TAD)
- Most sensitive for detecting IUGR (asymmetric type)
- Least accurate for dating but best for growth assessment
FL - Femur Length
- Ossified femoral diaphysis length (exclude distal epiphysis)
- Femur seen at ~45° angle from fetal spine
- FL/BPD ratio normal = 79% ± 8% (from 22-40 weeks)

NUCHAL TRANSLUCENCY (NT)

- When: 11 weeks 0 days to 13 weeks 6 days (CRL 45-84 mm)
- What: Fluid-filled translucent space at the back of fetal neck
- Normal: < 3.0 mm (or < 95th percentile for CRL)
- Increased NT (≥ 3.0 mm) associated with:
- Trisomy 21 (Down syndrome) - most common
- Trisomy 18 (Edwards), Trisomy 13 (Patau)
- Turner syndrome
- Cardiac defects
- Other structural anomalies
- Detection rate for Down syndrome: ~85-90%
SECOND TRIMESTER SCAN - TIFFA / Anomaly Scan (18-20 Weeks)
Fetal Anatomy Checklist (Required by AIUM Standards)
- Midline falx cerebri
- Lateral cerebral ventricles (atrium ≤ 10 mm = normal)
- Cavum septum pellucidum (CSP)
- Choroid plexus (normally hyperechoic, fills ventricles early)
- Cerebellum (dumbbell shape, measure transcerebellar diameter)
- Cisterna magna (2-10 mm)
- Nuchal fold (NF) 15-20 weeks: < 5 mm normal; ≥ 6 mm = risk for trisomy 21
- Lips (cleft lip/palate)
- Nose, profile
- Cervical, thoracic, lumbar, sacral - longitudinal and transverse
- Screen for spina bifida: "lemon sign" (frontal bone indentation) + "banana sign" (cerebellar herniation)
- Right and left ventricles roughly equal size
- Interventricular septum intact
- Atrioventricular valves visible and functioning
- Also obtain: LVOT, RVOT views
- Stomach bubble visible (if absent - check for esophageal atresia or swallowing issues)
- Kidneys (echogenic initially, renal pelvis AP diameter ≤ 7 mm)
- Urinary bladder visible
- Umbilical cord insertion site
- Anterior abdominal wall intact (rule out omphalocele/gastroschisis)
- Count bones and digits (both femora, tibiae, humeri, radii-ulnae)
PLACENTA
Normal Placenta Appearance
- Homogeneous, moderately echogenic structure on the uterine wall
- Thickness: ~1 mm per week gestation (up to ~4 cm at term)
- Posterior position most common; anterior, fundal also normal
Placental Grading (Grannum Classification)
| Grade | Timing | Features |
|---|---|---|
| 0 | Early | Homogeneous, smooth chorionic plate |
| I | Mid pregnancy | Subtle calcifications |
| II | ~36 weeks | Comma-shaped calcifications, indentations |
| III | Term | Complete septations, echogenic cotyledons |
Placenta Previa
- Low-lying placenta: Placental edge < 20 mm from internal cervical os
- Placenta previa: Placental edge covers the internal cervical os
- Diagnosis confirmed by transvaginal scan (transabdominal overestimates)
- Follow-up at 32 weeks for both low-lying and previa
- (Creasy & Resnik's Maternal-Fetal Medicine)
AMNIOTIC FLUID ASSESSMENT
Amniotic Fluid Index (AFI)
| AFI Value | Classification |
|---|---|
| 8-18 cm | Normal |
| < 5 cm | Oligohydramnios |
| 5-8 cm | Borderline |
| > 20-24 cm | Polyhydramnios |
Single Deepest Pocket (SDP)
- Normal: 2-8 cm
- < 2 cm = oligohydramnios
-
8 cm = polyhydramnios
Clinical Significance
| Finding | Causes |
|---|---|
| Oligohydramnios | Renal agenesis/dysplasia, IUGR, PROM, post-term pregnancy |
| Polyhydramnios | Fetal anomalies (esophageal atresia, anencephaly), maternal diabetes, twin-twin transfusion |
ECTOPIC PREGNANCY - USG Diagnosis
USG Findings in Ectopic Pregnancy
| Finding | Significance |
|---|---|
| Confirmed IUP in uterus | Effectively excludes ectopic (except heterotopic) |
| Empty uterus + adnexal mass | High suspicion for ectopic |
| Empty uterus + free fluid + echogenic adnexal mass | Near 100% risk of ectopic |
| Living embryo outside uterus | Diagnostic of ectopic (<10% cases) |
| "Pseudogestational sac" | Intrauterine fluid collection in ectopic - do not confuse with true GS |
- Gestational sac at 4.5 weeks
- Yolk sac at 5.5 weeks
- Fetal pole at 6.0 weeks (TAS approximately 1 week later)
DOPPLER IN PREGNANCY
Umbilical Artery Doppler
- S/D ratio (Systolic/Diastolic)
- Resistive Index (RI) = (S-D)/S
- Pulsatility Index (PI) = (S-D)/mean

| Umbilical Artery Finding | Significance |
|---|---|
| Normal diastolic flow | Normal placental resistance |
| Elevated S/D ratio | Increased placental resistance - IUGR risk |
| Absent End-Diastolic Flow (AEDF) | Severe placental insufficiency - fetal compromise |
| Reversed End-Diastolic Flow (REDF) | Imminent fetal danger - consider immediate delivery |
Middle Cerebral Artery (MCA) Doppler
- Normally high resistance vessel
- In fetal hypoxia: "brain-sparing effect" - MCA resistance falls (increased diastolic flow)
- MCA Pulsatility Index decreases = fetal compromise
- Cerebro-placental ratio (CPR) = MCA PI / UA PI (normal >1)
Uterine Artery Doppler
- Done at 11-14 weeks or 20-24 weeks
- Elevated resistance + notching = risk of preeclampsia and IUGR
BIOPHYSICAL PROFILE (BPP)
| Parameter | Normal (score 2) | Duration |
|---|---|---|
| Fetal breathing movements | ≥ 1 episode of ≥ 30 sec in 30 min | |
| Fetal movements | ≥ 3 body/limb movements in 30 min | |
| Fetal tone | ≥ 1 active extension/flexion (hand open/close, limb movement) | |
| Amniotic fluid | Single deepest pocket ≥ 2 cm | |
| Non-stress test (NST) | Reactive (2 accelerations ≥ 15 bpm × 15 sec in 20 min) |
- 8-10/10: Normal - low risk of fetal asphyxia
- 6/10: Equivocal - repeat in 24 hours
- 4/10: Abnormal - consider delivery
- 0-2/10: Strongly abnormal - deliver
FETAL PRESENTATION & PRESENTATION TYPES
- Cephalic (vertex): Head down - normal
- Breech: Bottom/feet down (frank, complete, footling)
- Transverse: Horizontal lie
- Oblique: Diagonal lie
COMMON ABNORMALITIES DETECTED ON OBSTETRIC USG
| Condition | USG Finding |
|---|---|
| Anencephaly | Absent calvarium, "frog-eye" appearance |
| Spina bifida | Lemon sign + banana sign; defect in spine |
| Hydrocephalus | Lateral ventricles > 10 mm (ventriculomegaly) |
| Gastroschisis | Bowel loops floating freely outside abdomen (no membrane) |
| Omphalocele | Abdominal contents in membrane-covered sac at cord insertion |
| Diaphragmatic hernia | Stomach/bowel in thorax, mediastinal shift |
| Renal agenesis | Absent kidneys, oligohydramnios (Potter sequence) |
| IUGR | AC < 5th percentile, EFW < 10th percentile, abnormal Doppler |
| Placenta previa | Placenta covers cervical os |
| Vasa previa | Fetal vessels crossing internal os (color Doppler) |
| Hydrops fetalis | Skin edema + 2 or more: ascites, pleural/pericardial effusion, placental edema |
| Down syndrome markers | Increased NT, short femur, echogenic bowel, choroid plexus cysts, absent nasal bone, short humerus |
FETAL WEIGHT ESTIMATION (EFW)
- EFW < 10th percentile for gestational age = Small for Gestational Age (SGA) / suspect IUGR
- EFW > 90th percentile = Large for Gestational Age (LGA) / suspect macrosomia
- Symmetric IUGR: All measurements proportionally small (chromosomal, early insult)
- Asymmetric IUGR: AC most affected, HC spared (placental insufficiency, late onset) - AC is the most sensitive measurement
CERVICAL LENGTH - Preterm Labor Screening
- Measured by transvaginal scan (TVS) - more accurate than transabdominal
- Normal: > 25 mm at 16-24 weeks
- < 25 mm at 16-24 weeks = increased risk of preterm birth
- < 15 mm = high risk
- Funneling of internal os (beaking) is an additional sign of incompetence
TIPS FOR GOOD IMAGE ACQUISITION
| Tip | Rationale |
|---|---|
| Full bladder for TAS in early pregnancy | Acts as acoustic window |
| Empty bladder for TVS | Better visualization |
| Use curvilinear probe for abdomen | Best depth/FOV for obstetric scanning |
| Harmonic imaging | Reduces noise, improves margins |
| Patient in left lateral tilt (>20 wks) | Reduces aortocaval compression |
| Increase depth for late third trimester | Fetal head may be deep in pelvis |
Abortion all about with images
spontaneous abortion types classification threatened incomplete complete missed ultrasound clinical features management
types of abortion ultrasound images threatened inevitable incomplete complete missed septic molar pregnancy
missed abortion anembryonic pregnancy blighted ovum ultrasound images incomplete abortion retained POC septic molar pregnancy snowstorm
hydatidiform mole molar pregnancy snowstorm ultrasound image complete partial mole USG beta hCG
An error occurred (ValidationException) when calling the ConverseStream operation: The model returned the following errors: messages.3.content.26.image.source.base64.data: At least one of the image dimensions exceed max allowed size for many-image requests: 2000 pixels
We encountered an error while processing your request. Please try again or reach out to us for help.