Dlco full details for md exam answer 15 marks with concept behind it
Reading File
Finding Sources
Finding Sources
Searching the Web
DLCO diffusing capacity lung CO test physiology clinical significance MD exam
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Loading Image
Finding Sources
Reading File
I now have comprehensive information to write a thorough 15-mark MD exam answer. Let me compose it:
DLCO (Diffusing Capacity of the Lung for Carbon Monoxide) — Complete 15-Mark Answer
1. DEFINITION
DLCO (also called Transfer Factor, TLCO) is a measure of the functional capacity of the lungs to transfer gas across the alveolar-capillary membrane into the pulmonary capillary blood. It quantifies the rate of CO uptake per unit of alveolar partial pressure gradient and is expressed as:
DLCO = mL CO/min/mmHg (at STPD — Standard Temperature and Pressure, Dry)
Normal resting value using the single-breath method ≈ 25 mL CO/min/mmHg (range ~20–30 in adults).
2. WHY CARBON MONOXIDE IS USED (The Concept)
Oxygen cannot be used to measure diffusing capacity directly because the PO₂ in pulmonary capillary blood changes continuously as blood flows through the capillary, making calculations unreliable.
Carbon monoxide (CO) is ideal because:
| Property | Significance |
|---|---|
| Affinity for Hb is 210× that of O₂ | CO binds haemoglobin so avidly that capillary PCO ≈ 0 |
| Capillary PCO ≈ zero | Entire alveolar–capillary gradient drives transfer; flow-limited component is negligible |
| Transfer is diffusion-limited, not perfusion-limited | Allows pure measurement of membrane + Hb-binding capacity |
| Minimal endogenous CO in blood | Background interference negligible |
The governing principle follows Fick's Law of Diffusion:
Rate of gas transfer ∝ (Surface Area × Pressure gradient × Solubility) / (MW^½ × Membrane Thickness)
3. COMPONENTS OF DLCO — THE ROUGHTON-FORSTER EQUATION
DLCO is the sum of two resistances in series:
$$\frac{1}{D_{LCO}} = \frac{1}{D_M} + \frac{1}{\theta \cdot V_c}$$
| Component | Meaning |
|---|---|
| D_M | Membrane diffusing capacity (alveolar-capillary membrane conductance) |
| θ (theta) | Rate of CO binding to Hb per unit Vc per unit PCO (reaction rate constant) |
| V_c | Pulmonary capillary blood volume |
Both membrane and blood components contribute. In emphysema, D_M falls; in anaemia, θ·Vc falls.
4. TEST TECHNIQUE — SINGLE-BREATH METHOD (Krogh Method, most widely used)
Step-by-step:
- Patient exhales completely to Residual Volume (RV)
- Rapidly inhales to Total Lung Capacity (TLC) from a gas mixture containing:
- 0.3% CO (tracer dose)
- ~10% Helium (inert, insoluble — for alveolar volume calculation)
- 21% O₂, balance N₂
- Breath-hold for 10 seconds — CO diffuses across alveolar-capillary membrane and binds Hb
- Rapid exhalation; first 750–1000 mL discarded (dead space washout)
- Alveolar gas sample collected and analyzed for CO and He concentrations
Calculation:
$$DLCO = \frac{60 \times V_A}{t_{bh} \times (P_B - 47)} \times \ln\left(\frac{FA_{CO_{initial}}}{FA_{CO_{final}}}\right)$$
Alveolar Volume (V_A) is calculated from helium dilution:
$$V_A = V_I \times \frac{F_{I_{He}}}{F_{A_{He}}}$$
KCO (Transfer Coefficient / Krogh Factor):
$$KCO = \frac{DLCO}{V_A}$$
KCO reflects diffusing capacity per unit lung volume and helps distinguish causes of a low DLCO.
5. OTHER METHODS OF MEASUREMENT
| Method | Principle | Use |
|---|---|---|
| Single-breath (SB) | 10-sec breath-hold | Standard clinical method |
| Steady-state | Continuous breathing of dilute CO; measures equilibrium | Used during exercise |
| Rebreathing | Rapid rebreathing of CO from bag | Requires rapid gas analyzers |
6. NORMAL VALUES AND INTERPRETATION
| Value | Significance |
|---|---|
| ≥75% of predicted | Normal |
| 60–75% | Mildly reduced |
| 40–60% | Moderately reduced — ↑ risk of postoperative pulmonary complications |
| <40% | Severely reduced — high risk; may indicate need for O₂ therapy; threshold for disability assessment |
Normal DLCO requires: normal alveolar-capillary surface, normal capillary blood volume (Vc), normal Hb, relatively homogeneous V/Q.
7. FACTORS AFFECTING DLCO
A. Physiological Variables (not disease)
| Factor | Effect on DLCO | Mechanism |
|---|---|---|
| Exercise | ↑ 2–3× normal | Capillary recruitment ↑ Vc |
| Supine position | ↑ | Increased pulmonary capillary filling |
| High altitude | ↑ | Hypoxia → alveolar capillary recruitment |
| Anaemia | ↓ | Reduced θ·Vc (less Hb to bind CO) |
| Polycythaemia | ↑ | More Hb available |
| Elevated alveolar PCO | ↑ | CO back-pressure effect (more Hb sites available) |
| Smoking (COHb) | ↓ (if not corrected) | CO back-pressure reduces gradient |
| Age | ↓ with age | Loss of alveolar surface |
| Height | ↑ | Larger lung volume |
| Female sex | ↓ than males | Smaller lung surface |
B. Correction for Haemoglobin
DLCO must be corrected for Hb:
$$DLCO_{corrected} = DLCO_{measured} \times \frac{(10.22 + Hb)}{1.7 \times Hb}$$ (for males)
8. CAUSES OF REDUCED DLCO
(A) Parenchymal / Membrane (↓ D_M)
| Condition | Mechanism |
|---|---|
| Emphysema | Loss of alveolar walls → ↓ surface area + ↓ Vc; DLCO disproportionately reduced vs. lung volumes |
| Interstitial Lung Disease (ILD) — IPF, sarcoidosis, asbestosis, berylliosis | Alveolar wall thickening + fibrosis → ↑ diffusion distance |
| Pulmonary oedema | Fluid in alveolar-capillary space ↑ diffusion barrier |
| Pneumonectomy / Lobectomy | Reduced total alveolar surface area |
| Sarcoidosis | Granulomatous thickening |
| Drug toxicity — Amiodarone, Bleomycin, Methotrexate | Alveolar/interstitial damage |
(B) Vascular (↓ Vc)
| Condition | Mechanism |
|---|---|
| Pulmonary arterial hypertension (PAH) | Reduced capillary bed perfusion |
| Pulmonary embolism / CTEPH | Loss of perfused capillary bed |
| Vasculitis | Destruction of pulmonary capillaries |
(C) Blood / Haematological
| Condition | Mechanism |
|---|---|
| Anaemia | ↓ θ·Vc — less Hb to bind CO |
| COHb (smoking, CO poisoning) | Occupied Hb binding sites; ↑ CO back-pressure |
9. CAUSES OF ELEVATED (INCREASED) DLCO
| Condition | Mechanism |
|---|---|
| Alveolar haemorrhage (Goodpasture's, Wegener's) | Blood in alveoli acts as additional Hb reservoir for CO binding → falsely elevated |
| Polycythaemia | ↑ Hb → ↑ θ·Vc |
| Left-to-right cardiac shunts | ↑ Pulmonary blood flow → ↑ Vc |
| Exercise | Capillary recruitment |
| Obesity | Supine-like effect, ↑ capillary volume |
| Early left heart failure | Engorgement of pulmonary capillaries (transiently) |
| Asthma (mild) | Slightly ↑ due to hyperinflation exposing more capillaries |
Alveolar haemorrhage is the classic "elevated DLCO" condition in MD exams. The elevated DLCO in the setting of haemoptysis and renal failure strongly suggests Goodpasture's syndrome.
10. DLCO IN SPECIFIC PATTERNS
PFT Interpretation Algorithm
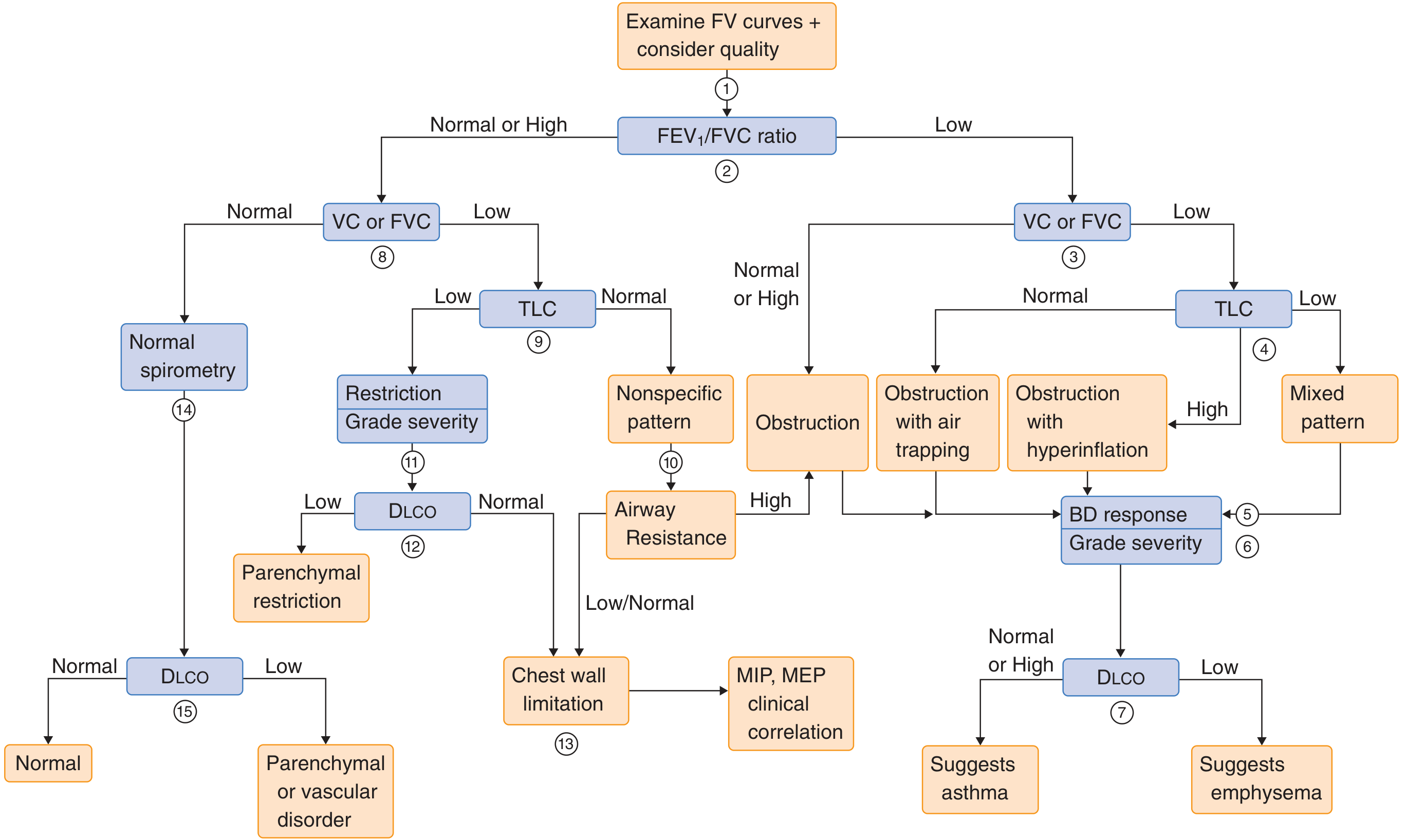
| Pattern | FEV1/FVC | TLC | DLCO | Likely Diagnosis |
|---|---|---|---|---|
| Obstruction + ↓ DLCO | ↓ | ↑ or normal | ↓ | Emphysema |
| Obstruction + normal DLCO | ↓ | Normal/↑ | Normal | Asthma, Chronic Bronchitis |
| Restriction + ↓ DLCO | Normal/↑ | ↓ | ↓ | ILD / Parenchymal restriction |
| Restriction + normal DLCO | Normal/↑ | ↓ | Normal | Chest wall disease, Neuromuscular |
| Normal spirometry + ↓ DLCO | Normal | Normal | ↓ | Early ILD, Pulmonary vascular disease (PAH, PE) |
| Normal spirometry + ↑ DLCO | Normal | Normal | ↑ | Alveolar haemorrhage, Polycythaemia |
11. CLINICAL APPLICATIONS OF DLCO
- Diagnosis of ILD — DLCO is reduced early in pulmonary fibrosis, often before spirometric abnormalities appear
- Distinguishing emphysema from asthma/chronic bronchitis (both obstructive, but DLCO reduced only in emphysema)
- Detecting pulmonary vascular disease — isolated ↓ DLCO with normal spirometry and TLC → PAH or CTEPH
- Pre-surgical risk assessment — PPO (predicted postoperative) DLCO >60% = low risk; <40% = high risk for resection
- Monitoring drug toxicity — Bleomycin, Amiodarone, Methotrexate
- Monitoring disease progression — ILD, connective tissue disease (SLE, RA, scleroderma)
- Predicting exercise-induced desaturation — DLCO <50% predicted
- Disability assessment — DLCO <40% may qualify for disability
12. KCO (TRANSFER COEFFICIENT) — A KEY DIFFERENTIATING TOOL
$$KCO = \frac{DLCO}{VA}$$
| Scenario | DLCO | VA | KCO | Interpretation |
|---|---|---|---|---|
| Emphysema | ↓ | ↓ (air trapping) | ↓↓ | True membrane loss |
| Post-pneumonectomy | ↓ | ↓ | Normal/↑ | Less lung, but remaining lung is normal — compensatory |
| ILD | ↓ | ↓ | ↓ or Normal | Membrane thickening + volume loss |
| Chest wall restriction | ↓ | ↓ | Normal | Volume loss only; membrane OK |
| PAH | ↓ | Normal | ↓ | Vascular disease, membrane OK |
13. CONTRAINDICATIONS TO DLCO TEST
- Absolute: Carbon monoxide toxicity, dangerous oxyhemoglobin desaturation without O₂ supplementation
- Relative: Recent MI, recent eye surgery, inability to perform respiratory maneuvers
SUMMARY TABLE
| Parameter | Value |
|---|---|
| Test gas | 0.3% CO + ~10% He + 21% O₂ |
| Breath-hold | 10 seconds |
| Normal DLCO | ~25 mL CO/min/mmHg |
| Units | mL/min/mmHg (STPD) |
| Normal % predicted | 75–140% |
| CO affinity vs O₂ | 210× greater |
| DLCO/VA = | KCO (Transfer Coefficient) |
| Classic ↑ DLCO | Alveolar haemorrhage, Polycythaemia |
| Classic ↓ DLCO | Emphysema, ILD, PAH |
Sources: Miller's Anesthesia 10e; Barash's Clinical Anesthesia 9e; Goldman-Cecil Medicine; Fishman's Pulmonary Diseases and Disorders
Tell me from this dlco full details for md exam answer 15 marks
Reading File
Running Command
Running Command
Running Command
Running Command
Running Command
Running Command
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.