Gastritis complete pathology answer for mbbs
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Give a short note answer on gastritis pathology
I have all the information needed from the previous research. Here is a complete short note on Gastritis for MBBS pathology:
Gastritis - Short Note (Pathology)
Definition
Gastritis is mucosal inflammation of the stomach. When inflammatory cells are absent or rare, the term gastropathy is used instead.
Classification
| Type | Duration | Key Feature |
|---|---|---|
| Acute gastritis | Short-lived | Neutrophilic infiltrate |
| Chronic gastritis | Persistent | Lymphocytes, plasma cells, atrophy |
ACUTE GASTRITIS
Etiology
- NSAIDs (inhibit COX-1/COX-2 → reduced prostaglandins → ↓ mucus, bicarbonate, blood flow)
- Alcohol, bile reflux, chemotherapy, radiation
- Severe physiologic stress (burns → Curling ulcer; raised ICP → Cushing ulcer; sepsis/shock → stress ulcers)
- Uremia, ingestion of caustic substances
Morphology
- Mucosal edema and vascular congestion
- Neutrophilic infiltrate in lamina propria and within gland lumina
- Superficial erosions with fibrin-containing exudate
- Hemorrhage → acute erosive hemorrhagic gastritis (dark hemorrhagic puncta in hyperemic mucosa)
- Lesions are typically superficial - do not penetrate the muscularis mucosae
Clinical Features
- Epigastric pain, nausea, vomiting
- Upper GI bleed in severe cases
- Heals within days to weeks after removing the offending agent
CHRONIC GASTRITIS
Etiology (in order of frequency)
- H. pylori infection (most common)
- Autoimmune (anti-parietal cell antibodies)
- NSAIDs (chronic use)
- Radiation, bile reflux, Crohn disease, amyloidosis, GVHD
H. PYLORI GASTRITIS
About the Organism
- Gram-negative, spiral-shaped, flagellated bacillus
- Discovered by Robin Warren and Barry Marshall (Nobel Prize 2005)
- Most common chronic bacterial infection - >50% of the world's population infected
- Route: fecal-oral transmission; infection typically acquired in childhood
Virulence Factors (4 key features)
| Factor | Role |
|---|---|
| Flagella | Movement through viscous mucus |
| Urease | Generates ammonia from urea → elevates local pH → protects from acid |
| Adhesins | Enhances binding to foveolar cells |
| CagA toxin | Stimulates IL-8 release → chemotaxis of neutrophils → mucosal damage |
Pathogenesis
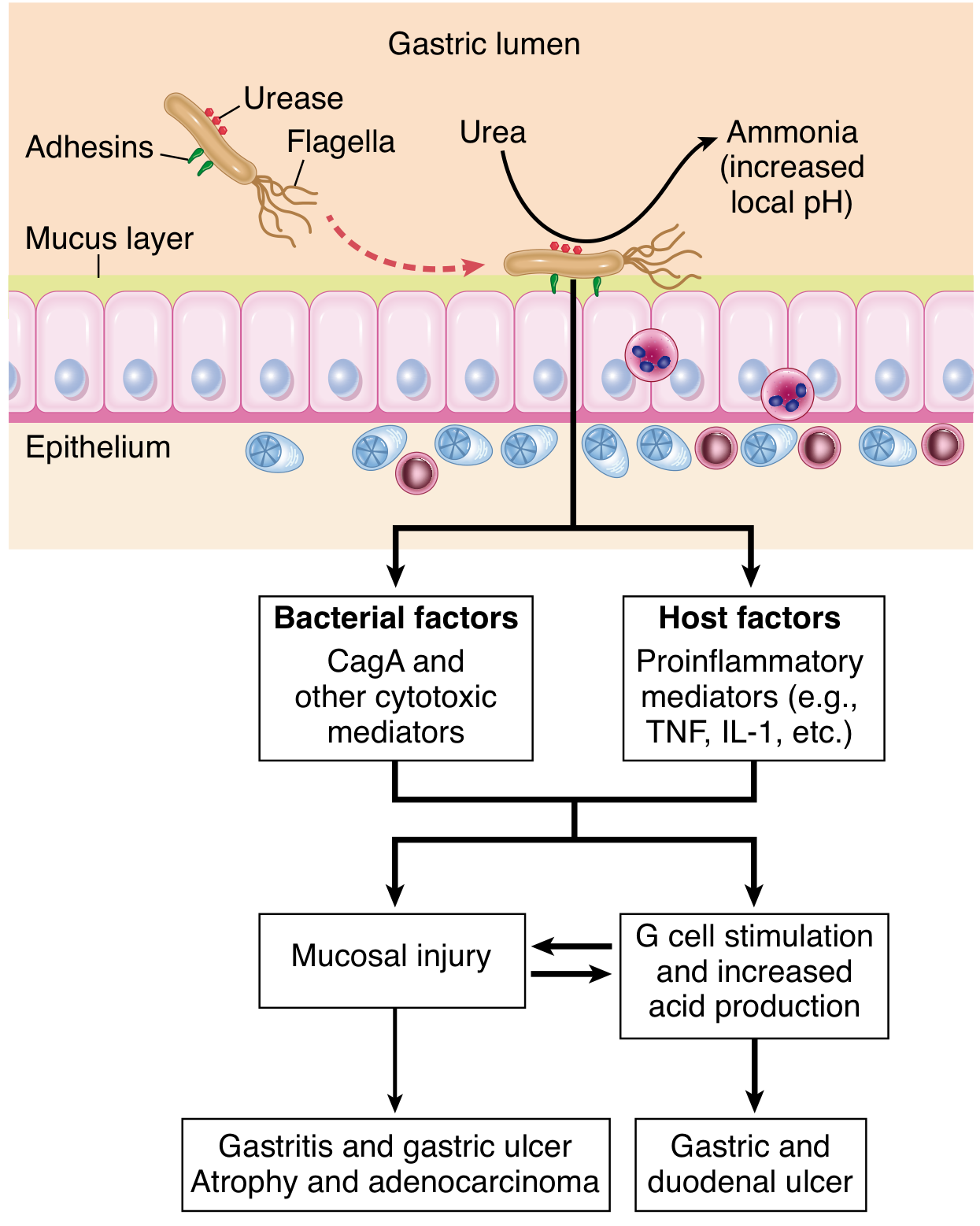
- Colonizes antrum → stimulates G cells → ↑ gastrin → ↑ acid → risk of peptic ulcer disease
- Long-standing infection spreads to body/fundus → atrophic gastritis + intestinal metaplasia → risk of gastric adenocarcinoma
- Induces MALT → risk of MALToma (B-cell lymphoma)
Morphology
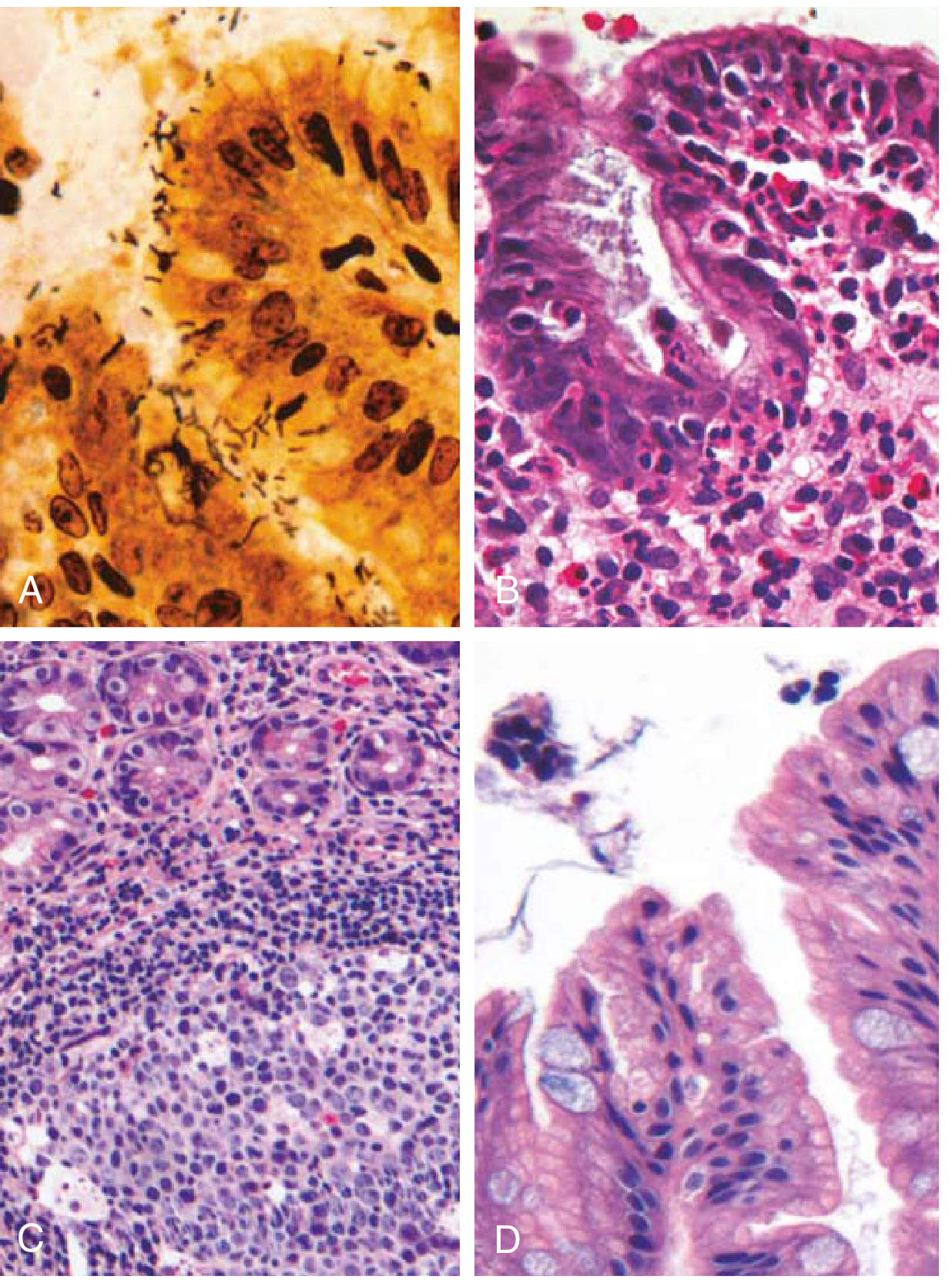
- Organisms lie within mucus overlying foveolar cells (antrum preferred)
- Stains: H&E, Giemsa, Warthin-Starry silver stain, immunohistochemistry
- Neutrophils in lamina propria and within gland lumina ("pit abscesses")
- Plasma cells in clusters/sheets + lymphocytes + macrophages in superficial lamina propria
- Lymphoid aggregates with germinal centers (MALT induction)
- Thickened rugal folds in intense inflammation
- Intestinal metaplasia: goblet cells + columnar absorptive cells
Diagnosis
- Urea breath test (non-invasive, based on urease activity)
- Stool antigen test
- Serology (anti-H. pylori antibodies)
- Rapid urease test (CLO test) on biopsy
- H&E/Giemsa on biopsy
AUTOIMMUNE GASTRITIS (Type A)
Key Features
- Accounts for <10% of chronic gastritis cases
- Affects body and fundus (antrum spared)
- Median age: 60 years; slight female predominance
Pathogenesis
- CD4+ T cells and autoantibodies directed against parietal cell components, especially H⁺/K⁺-ATPase (proton pump)
- Loss of parietal cells → ↓ acid (achlorhydria) + ↓ intrinsic factor
- ↓ acid → hypergastrinemia → antral G-cell hyperplasia
- ↓ intrinsic factor → ↓ ileal B12 absorption → pernicious anemia (megaloblastic)
Characteristic Laboratory Findings
- Anti-parietal cell antibodies (against H⁺/K⁺-ATPase) - up to 80% of patients
- Anti-intrinsic factor antibodies
- ↓ serum pepsinogen I
- Achlorhydria + markedly elevated gastrin
- B12 deficiency
Morphology
- Diffuse atrophy of oxyntic mucosa (body + fundus)
- Rugal folds lost (thinned mucosa)
- Inflammatory infiltrate: lymphocytes, macrophages, plasma cells - centered on glands (deeper than H. pylori)
- Neutrophils are NOT prominent (unlike H. pylori)
- Extensive parietal cell and chief cell loss
- Intestinal metaplasia with goblet cells (risk of adenocarcinoma)
- Enterochromaffin-like (ECL) cell hyperplasia → may progress to gastric carcinoid tumors
Associations
Hashimoto thyroiditis, Type 1 DM, Addison disease, Graves disease
COMPARISON TABLE: H. pylori vs Autoimmune Gastritis
| Feature | H. pylori | Autoimmune |
|---|---|---|
| Location | Antrum | Body & Fundus |
| Inflammatory cells | Neutrophils, subepithelial plasma cells | Lymphocytes, macrophages |
| Acid production | Increased / slightly decreased | Decreased (achlorhydria) |
| Gastrin | Normal to markedly increased | Markedly increased |
| Serology | Anti-H. pylori antibodies | Anti-parietal cell, anti-IF antibodies |
| Other lesions | Hyperplastic/inflammatory polyps | Neuroendocrine (ECL) hyperplasia |
| Sequelae | PUD, adenocarcinoma, MALToma | Atrophy, pernicious anemia, adenocarcinoma, carcinoid |
COMPLICATIONS OF CHRONIC GASTRITIS
1. Intestinal Metaplasia
- Goblet cells replace gastric epithelium
- Strongly associated with gastric adenocarcinoma risk
- May regress after H. pylori eradication
2. Dysplasia
- Epithelial nuclear enlargement, hyperchromasia, loss of polarity
- Precursor to gastric carcinoma
- Dysplastic cells remain cytologically immature at the surface (unlike reactive cells which mature)
3. MALToma
- H. pylori-induced MALT can transform into B-cell lymphoma
- May regress with H. pylori eradication
4. Pernicious Anemia
- Autoimmune gastritis → loss of intrinsic factor → B12 deficiency → megaloblastic anemia
5. Gastric Carcinoid Tumors
- From ECL cell hyperplasia driven by hypergastrinemia in autoimmune gastritis
SPECIAL FORMS OF GASTRITIS
| Form | Key Points |
|---|---|
| Ménétrier disease | Excessive TGF-α → diffuse foveolar hyperplasia, giant rugal folds, protein-losing enteropathy; ↑ risk of adenocarcinoma |
| Phlegmonous (suppurative) gastritis | Bacterial infection of submucosa/muscularis; gram-negative bacilli, streptococci; rare, life-threatening |
| Emphysematous gastritis | Gas-producing organisms (Clostridium perfringens); gas in gastric wall on CT; fatal without treatment |
| Eosinophilic gastritis | Eosinophilic infiltrate; associated with allergy/parasites |
| Lymphocytic gastritis | >25 intraepithelial lymphocytes/100 epithelial cells; associated with celiac disease, H. pylori |
| Granulomatous gastritis | Crohn disease, sarcoidosis, TB, syphilis |
SYDNEY SYSTEM (Classification)
The updated Sydney System classifies chronic gastritis based on:
- Topography (antrum, corpus, pangastritis)
- Morphology (atrophy, metaplasia, activity)
- Etiology (H. pylori, autoimmune, chemical, etc.)
HIGH-YIELD EXAM POINTS
- Most common cause of chronic gastritis = H. pylori
- Most common cause in H. pylori-negative patients = autoimmune
- H. pylori stain = Giemsa or Warthin-Starry silver stain
- Pernicious anemia = Type A (autoimmune) gastritis
- MALT lymphoma → associated with H. pylori; can regress with eradication
- Intestinal metaplasia = risk factor for gastric adenocarcinoma in all forms of chronic gastritis
- Anti-parietal cell antibody target = H⁺/K⁺-ATPase
- Curling ulcer = burns; Cushing ulcer = raised ICP
Sources: Robbins, Cotran & Kumar - Pathologic Basis of Disease | Robbins & Kumar - Basic Pathology | Sleisenger & Fordtran's Gastrointestinal and Liver Disease
Gastritis classification as well as complete parhology in crisp and short answer for 8marks
Based on my comprehensive research from the previous session, here is a crisp, exam-ready 8-mark answer:
GASTRITIS
Definition
Gastritis = mucosal inflammation of the stomach. (Absent/rare inflammatory cells = gastropathy)
CLASSIFICATION
A. Based on Duration
| Type | Cells | Key Feature |
|---|---|---|
| Acute | Neutrophils | Erosions, hemorrhage |
| Chronic | Lymphocytes, plasma cells | Atrophy, metaplasia |
B. Etiological / Clinical (Most Exam-Relevant)
Type A (Autoimmune) - Body & Fundus
Type B (Bacterial/H. pylori) - Antrum
Type C (Chemical/Reactive) - NSAIDs, bile reflux
C. Sydney System (Updated)
Classifies based on:
- Topography - Antrum / Corpus / Pangastritis
- Morphology - Grade of atrophy, metaplasia, activity
- Etiology - H. pylori / Autoimmune / Chemical
D. Morphological Types
- Superficial gastritis
- Atrophic gastritis (multifocal / autoimmune)
- Hypertrophic gastropathy (Ménétrier disease)
ACUTE GASTRITIS
Etiology
- NSAIDs (↓ prostaglandins → ↓ mucus/bicarb/blood flow)
- Alcohol, chemotherapy, radiation
- Stress: Burns → Curling ulcer | ↑ICP → Cushing ulcer | Sepsis/shock → Stress ulcer
- Uremia, caustic ingestion
Morphology
- Mucosal edema + vascular congestion
- Neutrophils in lamina propria + within gland lumina
- Superficial erosions + fibrin exudate
- Hemorrhage → Acute erosive hemorrhagic gastritis
- Lesions superficial (do not penetrate muscularis mucosae)
Clinical Features
- Epigastric pain, nausea, vomiting
- Hematemesis in severe cases
- Heals in days-weeks after removing cause
CHRONIC GASTRITIS
Two Main Types:
1. H. PYLORI GASTRITIS (Type B)
Organism: Gram-negative, spiral/curved, flagellated bacillus
4 Virulence Factors:
| Factor | Function |
|---|---|
| Flagella | Motility in mucus |
| Urease | NH₃ from urea → buffers acid |
| Adhesins | Binds foveolar cells |
| CagA toxin | ↑IL-8 → neutrophil chemotaxis → mucosal damage |
Pathogenesis:
Antrum colonization → G cell stimulation → ↑Gastrin → ↑Acid → PUD
Long-standing → spreads to body → Atrophy + Intestinal metaplasia → Adenocarcinoma
MALT induction → MALToma
Morphology:
- Organisms in mucus overlying foveolar cells
- Stain: Giemsa / Warthin-Starry silver stain / IHC
- Neutrophils in lamina propria + pit abscesses
- Plasma cells in sheets (superficial lamina propria)
- Lymphoid aggregates with germinal centers (MALT)
- Intestinal metaplasia (goblet cells)
Diagnosis:
- Urea breath test, Stool antigen test, Serology
- Biopsy: Rapid urease (CLO) test, culture, PCR
2. AUTOIMMUNE GASTRITIS (Type A)
Site: Body & Fundus (antrum spared)
Pathogenesis:
CD4+ T cells + Autoantibodies (against H⁺/K⁺-ATPase) → Parietal cell destruction
→ ↓ Acid (achlorhydria) → ↑ Gastrin → G-cell hyperplasia
→ ↓ Intrinsic factor → ↓ B12 absorption → Pernicious anemia
Labs:
- Anti-parietal cell antibodies (anti-H⁺/K⁺-ATPase) - 80%
- Anti-intrinsic factor antibodies
- ↓ Pepsinogen I, Achlorhydria, ↑↑ Gastrin
Morphology:
- Diffuse atrophy of oxyntic mucosa - rugal folds lost
- Infiltrate: lymphocytes, macrophages, plasma cells - centered on glands (deep)
- NO prominent neutrophils
- Extensive parietal + chief cell loss
- Intestinal metaplasia
- ECL cell hyperplasia → Gastric carcinoid tumor
Associations: Hashimoto thyroiditis, Type 1 DM, Addison disease, Graves disease
COMPARISON TABLE (High-Yield)
| Feature | H. pylori (Type B) | Autoimmune (Type A) |
|---|---|---|
| Site | Antrum | Body & Fundus |
| Cells | Neutrophils + plasma cells | Lymphocytes, macrophages |
| Acid | ↑ (antral) / ↓ (atrophy) | ↓ (achlorhydria) |
| Gastrin | Normal - ↑ | ↑↑↑ (markedly) |
| Antibodies | Anti-H. pylori | Anti-parietal cell, anti-IF |
| Complications | PUD, Adenocarcinoma, MALToma | Pernicious anemia, Adenocarcinoma, Carcinoid |
COMPLICATIONS OF CHRONIC GASTRITIS
- Intestinal metaplasia → Precursor to gastric adenocarcinoma
- Dysplasia → Direct precancer (cells immature at surface)
- MALToma → H. pylori-driven B-cell lymphoma (may regress with eradication)
- Pernicious anemia → Autoimmune (B12 deficiency, megaloblastic)
- Gastric carcinoid → ECL hyperplasia from hypergastrinemia
HIGH-YIELD EXAM POINTS ★
- Most common chronic gastritis = H. pylori
- H. pylori stain = Giemsa / Warthin-Starry
- Nobel Prize 2005 = Warren & Marshall (H. pylori)
- Anti-parietal cell Ab target = H⁺/K⁺-ATPase
- Pernicious anemia → Type A (autoimmune) gastritis
- MALT lymphoma → H. pylori (can regress with eradication)
- Curling = Burns | Cushing = ↑ICP
- Intestinal metaplasia = risk for adenocarcinoma in ALL types of chronic gastritis
Sources: Robbins, Cotran & Kumar - Pathologic Basis of Disease | Robbins & Kumar - Basic Pathology
This is a shared conversation. Sign in to Orris to start your own chat.