Modified lynch algorithm
Reading File
Finding Sources
Searching the Web
modified Lynch algorithm colorectal surgery large bowel obstruction
Searching PubMed
"Lynch algorithm" colorectal obstruction
Finding Sources
Searching the Web
modified Lynch algorithm ophthalmology eyelid reconstruction lacrimal surgery
Reading File
Reading File
Searching the Web
"modified Lynch algorithm" OR "Lynch Howarth" frontal sinus surgery approach
Reading Article
PMID: 3669838
Reading File
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC3214493
Loading Image
I now have everything needed for a thorough answer. Here is a comprehensive response:
Modified Lynch Procedure / Lynch Incision
The term "modified Lynch" appears in two related but distinct ENT/head & neck surgical contexts: (1) the Modified Lynch Procedure for frontal sinus disease (the most classically described "algorithm"), and (2) the Modified Lynch (Howarth) incision, a facial access incision used in rhinology, orbital, and skull-base surgery.
1. Modified Lynch Procedure for Chronic Frontal Sinus Disease
Historical Background
The original Lynch operation (1921) was an external frontoethmoidectomy for frontal sinusitis that involved radical removal of sinus mucosa and creation of a naso-frontal communication, with high failure and stenosis rates.
The Modified Lynch Procedure (Neel-Lake modification), described by Neel, McDonald, and Facer in The Laryngoscope (1987, PMID 3669838), revised this approach substantially.
Key Differences from the Original Lynch Operation
| Feature | Original Lynch | Modified Lynch (Neel-Lake) |
|---|---|---|
| Mucosal removal | All mucosa stripped | Normal mucosa preserved |
| Turbinate | Middle turbinate removed | Middle turbinate preserved |
| Bone removal | Extensive | Limited to anterior frontal floor, lacrimal bone, anterior ethmoid cells |
| Stenting | Not standardized | Soft, non-reactive Silastic sheeting used |
| Approach | External only | Begins with intranasal anterior ethmoidectomy |
| Agger nasi | Not addressed | Removed by curetting forward between frontal process of maxilla and septum |
Operative Steps
- Intranasal anterior ethmoidectomy - the operation begins endoscopically/intranasally
- Agger nasi cell removal - curetted forward between the frontal process of the maxilla and the nasal septum
- Limited bone removal - restricted to:
- Anterior floor of the frontal sinus
- Portion of the lacrimal bone
- Bone overlying the anterior ethmoid cells
- Preservation of normal-appearing mucosa - of the frontal-ethmoid complex and frontal process of the superior maxilla
- Silastic stenting - thin, soft, non-reactive Silastic sheeting is placed to stent the naso-frontal passageway
- Reepithelialization - remaining normal mucosa accelerates healing of the naso-frontal duct
Rationale
The key insight of the modification is that complete mucosa removal is unnecessary for a good result. Retained normal mucosa actually hastens reepithelialization of the naso-frontal duct. Silastic stenting maintains patency while the duct heals.
Outcomes
- Original follow-up: 7% failure rate
- At 13.5-year mean follow-up: failure rate rose to 20% (3 of 15 ducts)
- This is the longest reported follow-up for any such series in the literature
Indications
- Chronic frontal sinusitis refractory to medical therapy
- Cases where endoscopic approaches are not feasible (far lateral disease, narrow nasofrontal recess)
- Frontal sinus mucoceles (alongside the Lynch-Howarth incision)
2. Modified Lynch (Lynch-Howarth) Incision
This is the external facial incision used to access the medial orbital wall, ethmoid sinuses, frontal sinus, and anterior skull base.
Incision Description
The incision runs along the superomedial orbit:
- Begins under the medial end of the eyebrow (placed along the lower eyebrow border, or in a skin crease - the latter gives better cosmesis)
- Extends approximately 0.5 cm medial to the medial canthus
- Can extend cephalad to the medial eyebrow for access to the frontal sinus
- Can extend inferiorly to be incorporated into a lateral rhinotomy for more extensive access
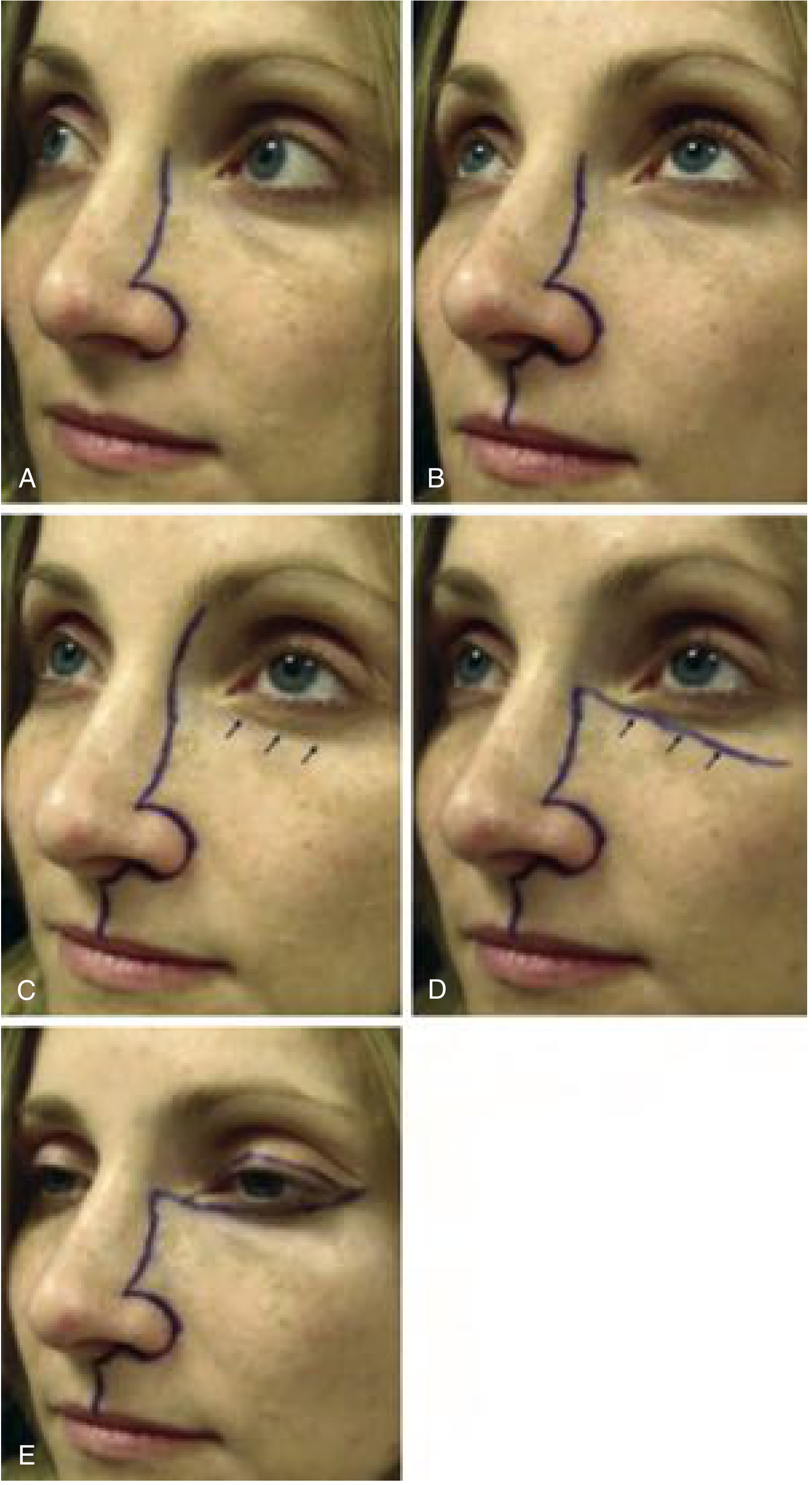
Modified facial incisions showing the Lynch extension used for nasal cavity/paranasal sinus access (from Cummings Otolaryngology)
Surgical Uses
| Application | Structures Accessed |
|---|---|
| Anterior ethmoid artery ligation | Between periorbita and skull base after removing lamina papyracea |
| Subperiosteal abscess drainage | Medial orbital wall (especially in children when endoscopic field is poor) |
| Frontal sinus surgery | When lateral frontal sinus disease is inaccessible endoscopically |
| Paranasal sinus mucoceles | Drainage and obliteration of frontal/ethmoidal mucoceles |
| Medial maxillectomy | Component of extended access for nasal/sinus tumors |
Extensions
- Lynch + lateral rhinotomy - for large sinonasal tumors involving the medial orbit and nasal cavity
- Lynch + Weber-Ferguson - adds upper lip split for inferior access (palate, infrastructure of maxilla)
- Lynch + subciliary (Dieffenbach) - adds lower eyelid crease incision for orbital floor access
Cosmetic Considerations
Placing the incision inside the eyebrow can produce a thick, visible scar. A skin-crease incision or one placed along the lower eyebrow border generally gives superior cosmetic results and can often be concealed at the hair-skin junction.
Anterior Ethmoid Artery Ligation via Modified Lynch Incision
A particularly important application highlighted in Scott-Brown's Otorhinolaryngology:
"The anterior ethmoid artery is more difficult to access endoscopically as it is only found within a mesentery that can be ligated in a small portion of cases. An external approach using a modified Lynch incision is often the preferred method of ligation." - Scott-Brown's Otorhinolaryngology Head & Neck Surgery
After the incision, removal of the lamina papyracea allows identification of the anterior and posterior ethmoid arteries between the periorbita and skull base, which can then be clipped or ligated. This is relevant in refractory posterior epistaxis when the anterior ethmoid artery contribution must be controlled.
Sources:
- Neel HB, McDonald TJ, Facer GW. Modified Lynch procedure for chronic frontal sinus diseases. Laryngoscope. 1987. [PMID 3669838]
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery (Vol 1), BOX 87.10-87.11
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery (Vol 2), Treatment of orbital complications
- Cummings Otolaryngology Head and Neck Surgery, Open Approaches (p. 1746)
Modified lynch algorithm for skin rash
Reading File
Finding Sources
Searching the Web
modified Lynch algorithm skin rash dermatology diagnosis
Searching PubMed
"Lynch" algorithm rash skin diagnosis
Reading Web Page
https://www.drhem.com/education/wp-content/uploads/2016/03/D…
Finding Sources
Searching PubMed
dermatologic emergency rash diagnosis algorithm morphology
Finding Sources
Reading Web Page
https://www.annemergmed.com/article/S0196-0644(20)31169-0/fu…
I have enough information from the PDF extraction to build a thorough, accurate answer. Here it is:
Modified Lynch Algorithm for Skin Rash
Overview
The Modified Lynch Algorithm is a systematic, morphology-based decision tree used primarily in emergency medicine to diagnose unknown rashes and identify life-threatening dermatologic conditions. It was originally developed by Peter Lynch (Lynch PJ, Edminster SC, 1984 - "Dermatology for the nondermatologist: a problem-oriented system", Ann Emerg Med) and has since been adapted and modified by emergency clinicians for rapid bedside use.
Its primary purpose is to help non-dermatologists (emergency physicians, hospitalists, internists) efficiently narrow the differential diagnosis of an unknown rash, with a focus on not missing life-threatening causes.
How the Algorithm Works
The algorithm uses a series of branching yes/no questions based purely on lesion morphology (what the rash looks like, not what caused it). The first and most critical branch point is:
Is the rash fluid-filled (vesicular/bullous) or solid?
From there, solid rashes are further subdivided by whether erythema is present, and then by the specific morphological subtype.
The Six Primary Rash Categories
The unknown rash is classified into one of six major morphological groups:
| Category | Description | Key Life-Threatening Diagnoses |
|---|---|---|
| 1. Maculopapular | Solid, non-fluid lesions with erythema; flat macules or raised papules <0.5 cm | Meningococcemia (early), Rocky Mountain spotted fever (early), drug hypersensitivity, viral exanthems, secondary syphilis, DRESS |
| 2. Petechial / Purpuric | Solid, non-blanching lesions with erythema; hemorrhagic spots | Meningococcemia, Rocky Mountain spotted fever, vasculitis, TTP, endocarditis |
| 3. Diffuse Erythematous | Widespread confluent redness, often blanching | Streptococcal/staphylococcal toxic shock syndrome, scarlet fever, Kawasaki disease, drug hypersensitivity, erythroderma |
| 4. Vesiculo-Bullous | Fluid-filled with clear content; vesicles (<0.5 cm) or bullae (>0.5 cm) | Stevens-Johnson syndrome (SJS), toxic epidermal necrolysis (TEN), erythema multiforme major, pemphigus vulgaris, varicella-zoster, herpes simplex, necrotizing fasciitis (late) |
| 5. Pustular | Fluid-filled with turbid/purulent content | Bacterial folliculitis, disseminated gonococcemia |
| 6. Non-Erythematous | Solid lesions without background erythema | Secondary syphilis, anthrax (ulcerated lesions) |
The Algorithm Flowchart (Step-by-Step Logic)
UNKNOWN RASH
│
▼
Is it FLUID-FILLED?
│
┌─YES──────────────────────────────────────┐
│ │
▼ ▼
Is fluid CLEAR? Is fluid CLOUDY/PURULENT?
│ │
▼ ▼
VESICULO-BULLOUS PUSTULAR
(SJS, TEN, varicella, (folliculitis, gonorrhea)
pemphigus, necrotizing
fasciitis late)
│
└─NO (Solid)──────────────────────────────►
│
Is there ERYTHEMA (background redness)?
│
┌─────────┴──────────┐
│ │
YES NO
│ │
▼ ▼
Is it PETECHIAL/PURPURIC? NON-ERYTHEMATOUS
│ (secondary syphilis,
┌───┴───┐ anthrax)
YES NO
│ │
▼ ▼
PETECHIAL/ Is it DIFFUSE
PURPURIC ERYTHEMA?
(meningococcemia, │
RMSF, TTP, ┌──┴──┐
vasculitis, YES NO
endocarditis) │ │
▼ ▼
DIFFUSE MACULOPAPULAR
ERYTHEMA (drug reaction,
(TSS, scarlet viral exanthem,
fever, Kawasaki, RMSF early,
erythroderma) meningococcemia early)
Worked Example
A 52-year-old man on ticlopidine and methyldopa presents with a petechial rash and underlying erythema:
- Fluid-filled? No → solid
- Erythema present? Yes
- Petechial/purpuric? Yes
- Differential: Vasculitis, TTP, meningococcemia, Rocky Mountain spotted fever, endocarditis
- History refines it: Ticlopidine use → TTP rises to top of list
- Confirmatory test: Platelet count in the ED → diagnostic and potentially life-saving
Key Life-Threatening Diagnoses Not to Miss
| Diagnosis | Category | Red Flag Features |
|---|---|---|
| Meningococcemia | Petechial/maculopapular (early → petechial) | Fever, non-blanching purpura, rapid progression, meningism |
| Rocky Mountain Spotted Fever | Petechial | Tick exposure, fever, starts on wrists/ankles spreading centrally |
| Toxic Epidermal Necrolysis (TEN) | Vesiculo-bullous | >30% BSA skin detachment, Nikolsky sign, mucous membrane involvement, drug trigger |
| Stevens-Johnson Syndrome (SJS) | Vesiculo-bullous | <10% BSA, mucous membrane involvement, drug trigger |
| Toxic Shock Syndrome | Diffuse erythematous | Fever, hypotension, diffuse sunburn-like rash, desquamation of palms/soles |
| Necrotizing Fasciitis | Variable (late: bullous) | Disproportionate pain, skin necrosis, crepitus, rapid spread |
| TTP | Petechial/purpuric | Thrombocytopenia, microangiopathic hemolytic anemia, neurologic symptoms |
| Kawasaki Disease | Diffuse erythematous | Pediatric, prolonged fever, strawberry tongue, conjunctivitis |
| DRESS | Maculopapular | Drug trigger (weeks prior), eosinophilia, organ involvement, facial edema |
Why Morphology-First?
The Lynch approach is explicitly morphology-first because:
- It is observable at the bedside without tests
- It avoids premature closure (jumping to a diagnosis before categorizing the lesion)
- It forces systematic thinking through the most dangerous possibilities in each category
- It is teachable and reproducible for trainees and non-dermatologists
Limitations
- Rashes evolve over time - a petechial RMSF rash begins as maculopapular
- Some diagnoses (e.g., erythema multiforme) can span multiple categories
- The algorithm focuses on emergency/life-threatening rashes and does not cover the full scope of dermatology
- Clinical context (fever, travel, medications, exposures, immune status) is still required to finalize diagnosis
Source: Lynch PJ, Edminster SC. Dermatology for the nondermatologist: a problem-oriented system. Ann Emerg Med. 1984 - as described in Emergency Medicine Practice (2002) and the JETem emergency dermatology curriculum.
This is a shared conversation. Sign in to Orris to start your own chat.