INTRA AORTIC BALLOON PUMP
Reading File
Finding Sources
Searching PubMed
"intra-aortic balloon pump"[MeSH Terms] AND "cardiogenic shock"[MeSH Terms]
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information from multiple authoritative textbooks. Here is the full breakdown:
Intra-Aortic Balloon Pump (IABP)
Overview and History
First described by Harken in 1958 and developed into clinical use in the early 1960s, the IABP is the most commonly used mechanical circulatory support (MCS) device. It operates on the principle of counterpulsation - moving blood volume in a direction "counter" to normal flow to assist the beating heart.
- Fischer's Mastery of Surgery, 8th ed.
- Braunwald's Heart Disease
Device Construction
- A 7- to 8-French double-lumen catheter with a 25-50 mL, 25-cm long sausage-shaped polyurethane balloon at its distal end
- One lumen connects to the pump console to inflate/deflate the balloon
- Helium gas is used exclusively because:
- Its low viscosity allows rapid transfer in and out of the balloon
- If rupture occurs, helium absorbs very rapidly in blood (safety advantage)
- The pump console controls timing via ECG or pressure triggers
Placement
- Inserted percutaneously via the femoral artery (most common) using fluoroscopic or ultrasound guidance
- Optimal position: descending aorta, just distal to the left subclavian artery, proximal to the renal arteries
- Operative placement in the ascending aorta or via the axillary artery is an alternative
Mechanism of Action - Counterpulsation
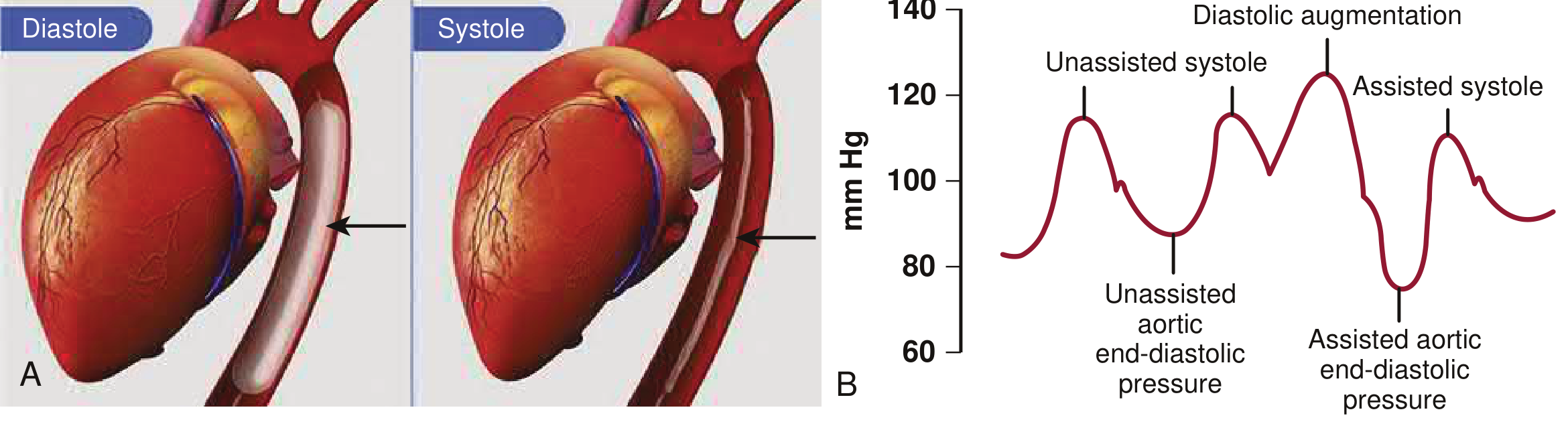
Inflation (Diastole):
- Triggered at aortic valve closure - corresponds to the dicrotic notch on arterial waveform or mid-T wave on ECG
- Balloon inflates, displacing blood from the descending aorta
- Elevates aortic diastolic pressure (diastolic augmentation)
- Increases coronary artery perfusion pressure
- Augments cerebral perfusion
Deflation (Pre-systole/End-diastole):
- Triggered at the R wave on ECG
- Rapid deflation creates a void in the aorta
- Reduces LV afterload (lower systemic vascular resistance)
- Lowers LV end-diastolic pressure
- Facilitates LV ejection, decreasing myocardial oxygen consumption (MVO2)
Net hemodynamic effects:
| Effect | Direction |
|---|---|
| Diastolic blood pressure | ↑ (augmented) |
| Systolic blood pressure | ↓ |
| Afterload | ↓ |
| Coronary perfusion | ↑ |
| Myocardial O2 consumption | ↓ |
| Cardiac output | Modestly ↑ |
| LV end-diastolic pressure | ↓ |
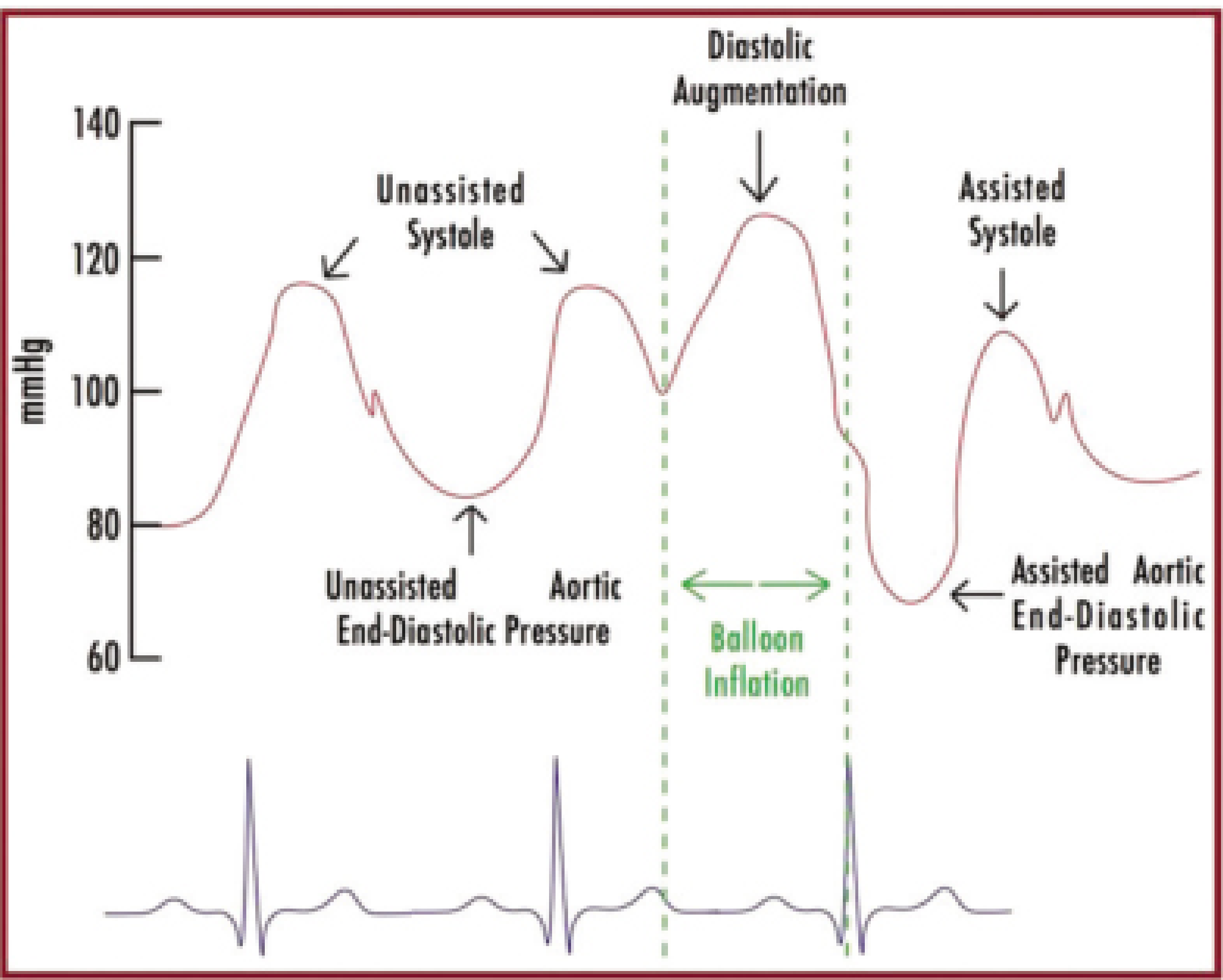
Timing and Trigger Modes
ECG triggering (most common):
- Inflation: mid-T wave (aortic valve closure)
- Deflation: peak R wave (onset of systole)
Pressure triggering:
- Inflation: dicrotic notch of aortic pressure tracing
- Deflation: just before systolic upstroke
Timing errors and consequences:
- Early inflation - increases afterload (inflates before aortic valve closes)
- Late inflation - reduces diastolic augmentation benefit
- Early deflation - reduces coronary perfusion benefit
- Late deflation - increases afterload (balloon still inflated when LV starts ejecting)
Counterpulsation ratios (assist frequency):
- 1:1 - full support (inflates with every beat)
- 1:2 - inflates every other beat (used during weaning)
- 1:3 - minimal support (used during weaning)
Indications
| Indication | Notes |
|---|---|
| Cardiogenic shock (AMI-related) | Most common indication |
| Acute CHF exacerbation with hypotension | LV failure support |
| High-risk PCI (prophylactic) | Hemodynamic support during procedure |
| Mechanical complications of MI (papillary muscle rupture, VSD) | Bridge to surgery |
| Post-CABG ventricular failure | Assist weaning from CPB |
| Refractory unstable angina | Bridge to revascularization |
| Bridge to definitive therapy (LVAD, transplant) |
Prerequisite: Patient must have some residual LV function and electrical stability, because any increase in cardiac output depends on the heart's own work.
Contraindications
Absolute:
- Severe aortic regurgitation (inflation worsens AR by increasing diastolic pressure back into LV)
- Aortic dissection (risk of propagation)
Relative:
- Aortic aneurysm
- Significant coagulopathy
- Severe peripheral arterial disease (especially at insertion site)
IABP vs. Other MCS Devices
| Device | Support Level | Cardiac Output Augmentation | Rhythm Dependency |
|---|---|---|---|
| IABP | Partial | ~0.5 L/min | Rhythm-dependent |
| Impella (CP) | Moderate-full | 2.5-5 L/min | Independent |
| VA-ECMO | Full | 4-6 L/min | Independent |
The IABP is a partial support device - it does not independently generate cardiac output. In contrast, Impella provides direct LV unloading and is independent of cardiac rhythm, providing greater hemodynamic support.
Clinical Evidence - IABP-SHOCK II Trial
The landmark IABP-SHOCK II trial (randomized, prospective, multicenter) evaluated IABP vs. best medical therapy in AMI complicated by cardiogenic shock, with all patients expected to undergo early revascularization:
- At 30 days: 39.7% mortality in IABP group vs. 41.3% in control (RR 0.96; 95% CI 0.79-1.17; p = 0.69) - no significant difference
- No significant difference in secondary endpoints or time to hemodynamic stabilization
- Outside of patients receiving reperfusion, long-term benefits of IABP are not clearly established
This has significantly changed practice - IABP use is declining as Impella and ECMO provide more robust hemodynamic support and greater reductions in LVEDP.
Complications
From the Benchmark Registry (AMI patients):
- Major complications: 2.6%
- All complications: 8.1%
Specific complications:
- Limb ischemia (major vascular complication - most common)
- Bleeding at insertion site
- Thrombotic complications (IV heparin given for prevention)
- Stroke
- Balloon rupture (helium gas embolism - rare but catastrophic)
- Infection
- Death
Weaning the IABP
- Gradually decrease counterpulsation ratio: 1:1 → 1:2 → 1:3
- Monitor hemodynamics at each step
- Remove when patient tolerates minimal support without hemodynamic deterioration
Key Points Summary
- Mechanism: Diastolic inflation augments coronary perfusion; systolic deflation reduces afterload
- Gas: Helium only (low viscosity, rapid absorption if rupture)
- Position: Descending aorta, distal to left subclavian, proximal to renal arteries
- Timing: ECG-triggered (R wave for deflation, T wave for inflation)
- Absolute contraindications: Aortic regurgitation and aortic dissection
- IABP-SHOCK II: No mortality benefit in cardiogenic shock complicating AMI
- Partial support only: Requires residual cardiac function to be effective
- Declining use: Impella and VA-ECMO now preferred for higher-acuity cardiogenic shock
Sources: Fischer's Mastery of Surgery 8th ed. | Braunwald's Heart Disease | Harrison's Principles of Internal Medicine 22e | Tintinalli's Emergency Medicine | Barash Clinical Anesthesia 9e | Morgan & Mikhail Clinical Anesthesiology 7e
Anaesthetic management of a patient posted for turp
Reading File
Finding Sources
Searching PubMed
"transurethral resection of the prostate"[MeSH Terms] AND "anesthesia"[MeSH Terms]
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive, high-quality data from Miller's Anesthesia 10e, Morgan & Mikhail 7e, and Barash 9e. Here is the complete, structured answer:
Anaesthetic Management of a Patient Posted for TURP
1. Preoperative Assessment
TURP patients are typically elderly men (>60 years) with benign prostatic hyperplasia (BPH) and a high burden of comorbidities. The preoperative work-up must be thorough.
History and Examination
- Cardiovascular: Assess for IHD, hypertension, heart failure, valvular disease - cardiac events are the leading cause of perioperative morbidity
- Respiratory: COPD, chronic bronchitis (common in elderly male smokers)
- Renal: Obstructive uropathy may cause chronic renal impairment; check baseline creatinine and eGFR
- Medications: Note anticoagulants, antiplatelets, alpha-blockers (tamsulosin), diuretics
- Coagulation: Previous catheterizations may have caused prostatic inflammation; assess for coagulopathy
- Exercise tolerance: Functional capacity estimate
Investigations
| Investigation | Rationale |
|---|---|
| FBC/Hb | Baseline; blood type and screen adequate for most; cross-match for large glands |
| U&E, creatinine | Renal function (obstructive uropathy) |
| Blood glucose | Elderly patients frequently diabetic |
| Coagulation screen | Especially if on anticoagulants |
| ECG | Cardiac baseline in elderly |
| CXR | If cardiorespiratory disease suspected |
| Urinalysis/MSU | Prostate is often bacterially colonized |
Anticoagulation Decision
- Patients on anticoagulant therapy require careful consideration before spinal anaesthesia
- Decision made jointly with the surgeon, weighing risk of stopping anticoagulation vs. benefit of regional technique
- May require bridging with short-acting anticoagulants (heparin)
- TURP itself carries significant postoperative bleeding risk, mandating normal coagulation perioperatively
2. Choice of Anaesthetic Technique
Spinal anaesthesia is the technique of choice for conventional monopolar TURP (M-TURP).
Why Spinal is Preferred
- Early detection of TURP syndrome: Patient remains awake - restlessness, confusion, and agitation are early warning signs of hyponatremia that would be masked under general anaesthesia
- Early detection of bladder/capsule perforation: Awake patient complains of new lower abdominal/back pain
- Lower mortality: A large ACS-NSQIP analysis (2010-2016, 28,486 TURP patients) showed neuraxial anaesthesia associated with lower 30-day mortality vs. general anaesthesia
- Reduced VTE risk: Regional anaesthesia reduces postoperative venous thrombosis
- Technically feasible: Adequate muscle relaxation of pelvic floor and perineum for surgeon
Spinal Anaesthesia - Key Points
- Target level: T10 - interrupts sensory transmission from prostate and bladder neck; also eliminates uncomfortable sensation of bladder distension
- Avoid levels above T10: Higher levels mask symptoms of bladder perforation (shoulder/abdominal pain, nausea/vomiting)
- Spinal preferred over epidural for TURP because:
- Technically easier in elderly patients
- Epidural may incompletely block sacral nerves (S2-S4) innervating prostate, bladder neck, and penis
- Spinal provides more reliable sacral coverage
When General Anaesthesia is Used
- Patient refusal of regional technique
- Technical difficulty performing neuraxial block
- Coagulopathy or anticoagulation
- Concerns about sacral nerve coverage
- Unpredictable operative duration (consider GA or CSE)
Caution: Under general anaesthesia, acute hyponatremia from TURP syndrome may delay or prevent emergence from anaesthesia. Restlessness in a sedated/GA patient must never be automatically attributed to inadequate anaesthesia and treated with more sedation/anaesthetic agents - this can be fatal.
3. Irrigating Fluids - Understanding the Problem
| Solution | Osmolality | Risk |
|---|---|---|
| Glycine 1.5% | 230 mOsm/L | Hyperglycinaemia, hyperammonaemia, transient blindness |
| Sorbitol 2.7% + Mannitol 0.54% | 195 mOsm/L | Hyperglycaemia (sorbitol), volume overload (mannitol) |
| Distilled water | 0 mOsm/L | Massive haemolysis - largely abandoned |
| Normal saline | 308 mOsm/L | No hyponatraemia risk - used in bipolar TURP |
- Electrolyte solutions cannot be used with monopolar TURP (they disperse electrocautery current)
- Bipolar TURP uses saline - eliminates hyponatraemia risk but volume overload still possible
- Bag/bottle height determines intravesical pressure and rate of fluid absorption - keep height low
4. Positioning
TURP is performed in lithotomy position with slight Trendelenburg tilt.
Physiological consequences:
- Decreased pulmonary compliance
- Cephalad shift of diaphragm
- Reduced lung volumes (RV, FRC, TV, VC)
- Increased cardiac preload
- Risk of lower limb compartment syndrome with prolonged positioning
Nerve injury risks: Common peroneal, sciatic, and femoral nerves - ensure careful padding
5. Intraoperative Monitoring
| Monitor | Purpose |
|---|---|
| ECG | Arrhythmias (from hyponatraemia/volume overload) |
| SpO2 | Desaturation (pulmonary oedema) |
| NIBP | Ongoing haemodynamic status |
| Temperature | Hypothermia monitoring |
| Urine output | Fluid balance |
| Mental status | Best monitor for TURP syndrome in awake patient |
| Fluid balance | Compare irrigant instilled vs. drained |
Fluid absorption monitoring thresholds (to detect TURP syndrome early):
- Halt surgery and assess Na⁺ if >750-1000 mL absorbed
- Terminate surgery if >1000-1500 mL absorbed (females) or >2000 mL (males)
- With saline irrigant (bipolar): terminate after >2500 mL absorbed
6. TURP Syndrome - The Central Complication
Definition
A constellation of signs and symptoms from systemic absorption of ≥2L of hypotonic irrigating fluid - causing:
- Circulatory fluid overload
- Dilutional hyponatraemia and hypo-osmolality
- Solute toxicity (glycine, sorbitol, mannitol)
Incidence: <1% to 10-15% depending on technique; onset from 15 minutes to 24 hours post-procedure.
Risk Factors
- Large prostate gland, prolonged resection (>1 hour)
- High intravesical irrigation pressure
- Open venous sinuses
- Hypotonic irrigants
- Low bag height vs. long resection time
Clinical Features
| System | Features |
|---|---|
| CNS | Headache, restlessness, confusion, agitation, visual disturbances (glycine), seizures, coma |
| CVS | Hypertension (early, from volume overload), then hypotension, arrhythmias, bradycardia |
| Respiratory | Dyspnoea, pulmonary oedema, cyanosis |
| Haematological | Haemolysis (with very hypotonic fluids) |
| Metabolic | Hyponatraemia, hypo-osmolality, hyperammonaemia (glycine), hyperglycaemia (sorbitol) |
Treatment
| Serum [Na⁺] | Management |
|---|---|
| >120 mEq/L + mild symptoms | Fluid restriction + IV furosemide (loop diuretic) |
| <120 mEq/L + severe symptoms (seizures, coma) | Hypertonic saline (3% NaCl) - correct slowly to avoid central pontine myelinolysis |
| Seizures | IV midazolam 2-4 mg; MgSO4 (counteracts glycine-mediated NMDA excitotoxicity) |
| Volume overload | Furosemide; consider haemodialysis if osmolality normal/near-normal |
| Respiratory | Supplemental O₂; ETT intubation if mental status doesn't improve |
Critical rule: Correct serum Na⁺ by no more than 10-12 mEq/L per 24 hours to avoid central pontine myelinolysis.
Novel prevention: A single oral dose of tolvaptan 15 mg (vasopressin V2 receptor antagonist, aquaretic) 2 hours before surgery may prevent hyponatraemia in expected long procedures.
7. Blood Loss Management
- Average blood loss: 3-5 mL/min of resection time (~200-300 mL total)
- Difficult to assess due to dilution with irrigating fluid
- Blood type and screen adequate for most; cross-match for large glands or anaemic patients
- ~2.5% patients require intraoperative transfusion
- Transfusion threshold guided by clinical signs of hypovolaemia + serial Hb for prolonged procedures
- Post-TURP haemorrhage: caused by release of prostatic tissue plasminogen activators causing fibrinolysis
- Treatment: ε-aminocaproic acid 4-5 g IV loading dose, then 1 g/h infusion; or tranexamic acid
8. Other Intraoperative Complications
| Complication | Notes |
|---|---|
| Hypothermia | Temperature falls ~1°C/hour of surgery; shivering in 16% with room-temp irrigation; prevent with warmed irrigation fluid |
| Bladder/capsule perforation | 2% incidence; awake patient reports lower abdominal/back pain; suspect with sudden hypotension/hypertension + vagal bradycardia |
| Septicaemia | Prostate often colonised; venous sinus opening allows bacteraemia; give prophylactic antibiotics (gentamicin, levofloxacin, or cefazolin) preoperatively |
| DIC | Release of thromboplastins from prostate tissue; treat with haematologist input, clotting factors, platelets |
| Primary fibrinolysis | Prostatic plasminogen activators; treat with ε-aminocaproic acid / tranexamic acid |
9. Postoperative Management
- Analgesia: Simple analgesics (paracetamol, NSAIDs if renal function permits); bladder spasm from catheter may require antispasmodics (oxybutynin)
- Monitoring for delayed TURP syndrome: Symptoms can appear hours after surgery
- Haematuria: Continuous bladder irrigation; haemorrhage in <1% requires surgical revision
- Fluid balance: Monitor for continued absorption of residual irrigation fluid
- Anticoagulation resumption: Discuss timing with surgeon given bleeding risk
- Temperature: Actively warm the patient if hypothermic
- DVT prophylaxis: Early mobilisation; consider LMWH given reduced VTE risk was a benefit of regional anaesthesia
10. Bipolar vs. Monopolar TURP - Anaesthetic Implications
| Feature | Monopolar (M-TURP) | Bipolar (B-TURP) |
|---|---|---|
| Irrigant | Hypotonic (glycine/sorbitol) | Normal saline |
| TURP syndrome risk | Yes (hyponatraemia) | No hyponatraemia, but volume overload still possible |
| Electrocautery | External return pad required | Self-contained circuit |
| Use of spinal | Still recommended to detect volume overload | Still beneficial |
Summary - Key Teaching Points
- Spinal to T10 is the anaesthetic of choice - allows early detection of TURP syndrome
- Never dismiss restlessness under sedation/GA as inadequate anaesthesia without excluding hyponatraemia
- Irrigating fluid monitoring is mandatory - track input vs. output throughout
- Treat TURP syndrome: mild - furosemide; severe - hypertonic saline (slow correction)
- Prophylactic antibiotics essential (prostate colonization + open venous sinuses)
- Warmed irrigation fluids prevent hypothermia
- Elderly patient with cardiac/renal comorbidity requires careful preop assessment
- Bipolar TURP with saline irrigant has reduced but not eliminated fluid-related complications
Sources: Miller's Anesthesia 10e | Morgan & Mikhail's Clinical Anesthesiology 7e | Barash Clinical Anesthesia 9e | Campbell-Walsh-Wein Urology | Hinman's Atlas of Urologic Surgery
This is a shared conversation. Sign in to Orris to start your own chat.