Does the serosanguineous exudate gets infected and, uh, lead to pus formation if it is immediately not treated or if it, uh, does really disturbs the collagen sheet?
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
I now have all the information needed for a thorough, well-sourced answer. Here it is:
Serosanguineous Exudate, Infection, and Collagen Disruption
What is serosanguineous exudate, really?
Serosanguineous exudate is a mixture of serum (clear plasma) and blood (red cells) that leaks from wound capillaries in the early inflammatory phase. It is normal and expected - even sterile wounds produce it. The fluid contains growth factors, fibrin, and immune cells that prepare the wound bed for healing. By itself, it is not pathological.
Can it become infected and lead to pus?
Yes - and here is the exact mechanism:
During the inflammatory phase, polymorphonuclear leukocytes (neutrophils) and mononuclear cells flood the wound. Their job is to phagocytose dead tissue, foreign material, and bacteria - essentially a biological debridement. When they die, they release their intracellular contents into the wound fluid.
"In excessive amounts, the contents form the purulence that is characteristic of infected wounds. Some exudate is expected even in the absence of bacterial invasion, but infection with accumulation of pus interferes with epithelialization and fibroplasia, and impairs wound healing."
- Roberts and Hedges' Clinical Procedures in Emergency Medicine
So the sequence is:
- Serosanguineous exudate is present (normal)
- Bacteria colonize the wound (from skin flora, environment, or contamination)
- Massive neutrophil recruitment occurs in response
- Dying neutrophils dump proteolytic enzymes, reactive oxygen species, and DNA into the wound fluid
- This liquefied material - dead neutrophils + bacteria + tissue debris - is pus (purulent exudate)
The critical threshold is around 10^5 organisms per gram of tissue - above this, wound healing is typically impaired and frank infection is established.
Does it need to be "immediately treated" to prevent infection?
Not necessarily immediately, but the risk rises with time and depends on several factors:
| Factor | Higher infection risk |
|---|---|
| Wound contamination | Dirt, feces, saliva, foreign bodies |
| Time since injury | >6 hours ("golden period") |
| Tissue devitalization | Crush injuries, ischemic edges |
| Host immunity | Diabetes, immunosuppression, poor vascularity |
| Wound type | Bite wounds, puncture wounds, dirty lacerations |
A clean surgical wound with minimal serosanguineous drainage does not automatically progress to infection. But an untreated contaminated wound, or one with devitalized tissue that bacteria can colonize, creates the perfect environment for bacterial proliferation.
Does infection actually disrupt the collagen sheet?
Yes - this is one of the most important mechanisms of impaired healing. Here is what happens:
-
Fibroplasia is blocked. New collagen synthesis by fibroblasts begins around day 4-5 after injury. Pus and ongoing infection interfere directly with fibroplasia - the fibroblasts cannot lay down organized collagen matrix in an infected, enzyme-rich environment.
-
Proteolytic degradation. Bacteria (especially Staphylococcus aureus, Pseudomonas, Streptococcus) secrete collagenases and other proteases. Neutrophil-derived matrix metalloproteinases (MMPs) also rise sharply. These enzymes actively digest the existing collagen framework.
-
Prolonged or persistent inflammation. Infected wounds with significant bacterial load or retained foreign material undergo a prolonged inflammatory response and may fail to progress to fibroplasia at all. This is why chronically infected wounds (diabetic foot ulcers, pressure sores) often stall in the inflammatory phase indefinitely.
-
Tensile strength never develops. Under normal conditions, tensile strength rises rapidly from day 5-17. In an infected wound, because collagen deposition is disrupted, the wound edges remain weak - leading to dehiscence (wound breakdown), abscess formation, or chronic non-healing.
The wound healing timeline (for reference):
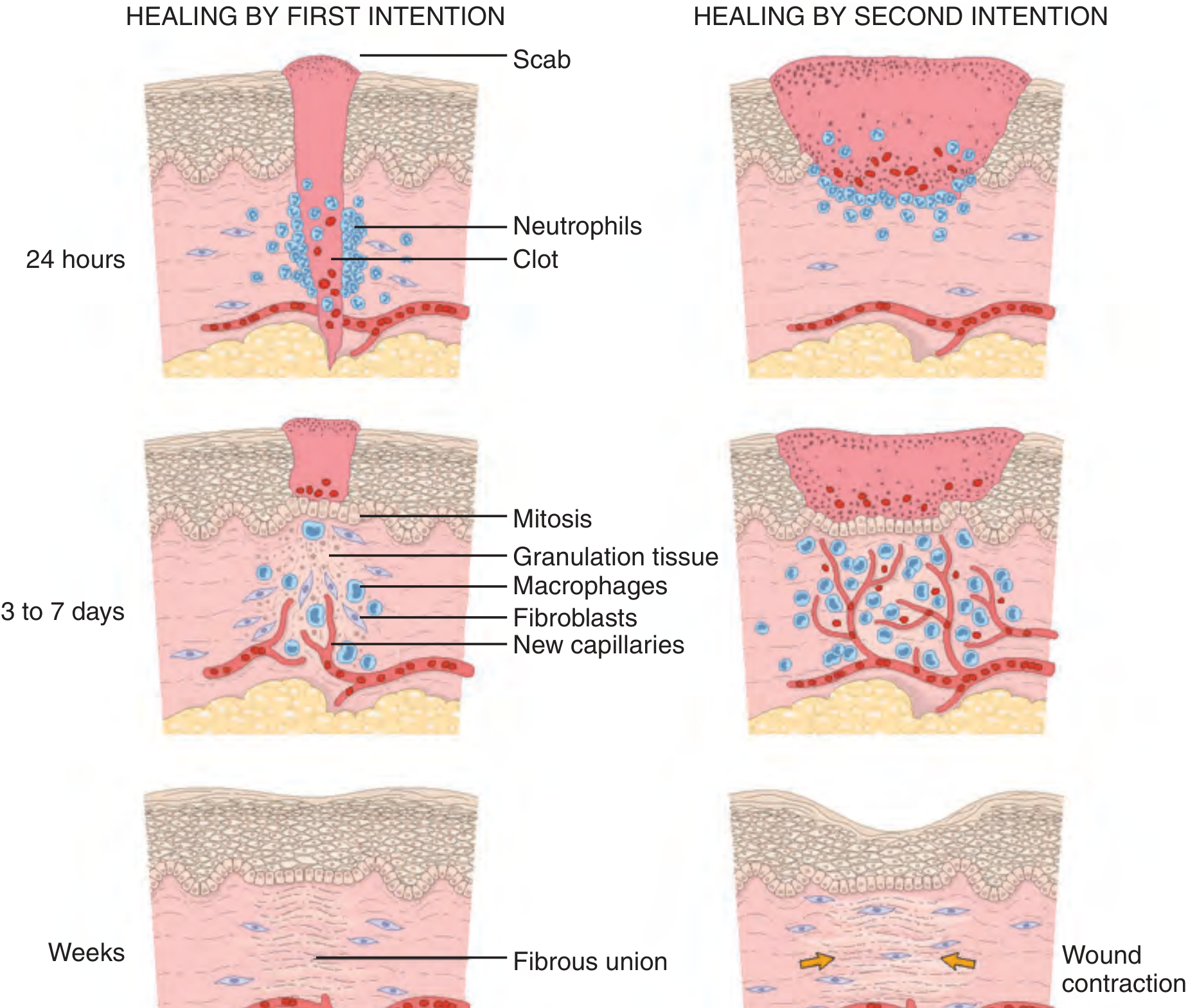
Roberts and Hedges' Clinical Procedures in Emergency Medicine - Steps in wound healing: healing by first intention (left) vs. second intention (right). Note the massive granulation tissue and wound contraction when infection/tissue loss forces secondary healing.
Summary
- Serosanguineous exudate is normal - it does NOT automatically become infected.
- Infection occurs when bacterial load overwhelms the wound's immune defenses.
- Once infected, pus forms from dying neutrophils releasing their contents.
- Pus and bacterial proteases directly disrupt collagen synthesis (fibroplasia) AND degrade already-formed collagen.
- This prevents tensile strength development and can lead to wound dehiscence, abscess formation, or chronic non-healing.
- Treatment (debridement, irrigation, appropriate antibiotics when indicated) is aimed at reducing bacterial burden to below the threshold where healing can resume.
Source: Roberts and Hedges' Clinical Procedures in Emergency Medicine, Background: Wound Healing, p. 739
This is a shared conversation. Sign in to Orris to start your own chat.