Grading of nuclear cataract Lid anatomy Peribulbar block (anaesthesia) Lens induced glaucoma
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching the Web
nuclear cataract grading LOCS III Emery-Little classification ophthalmology
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information for all four topics. Here is the full structured answer:
1. Grading of Nuclear Cataract
Nuclear cataract (nuclear sclerosis) involves progressive hardening and discolouration of the lens nucleus, ranging from clear/yellow to amber, brown, and finally black (brunescent/nigra cataract). Several grading systems are in clinical use.
Emery-Little Classification (most common clinical grading)
| Grade | Description | Nucleus appearance |
|---|---|---|
| I | Soft/clear | Transparent or faintly yellow; minimal density |
| II | Slightly hard | Yellow; mild nuclear sclerosis |
| III | Moderately hard | Deep yellow to amber; moderate sclerosis |
| IV | Hard | Brownish (brunescent); dense sclerosis |
| V | Very hard | Black (nuclear nigra); extremely dense |
- Higher grades require greater phacoemulsification energy and carry more risk of corneal endothelial damage.
LOCS III (Lens Opacities Classification System III)
The most widely used research/clinical trial grading system. Uses photographic slit-lamp standards.
Nuclear opacity is graded on two parameters in parallel:
| Parameter | Range | Meaning |
|---|---|---|
| NO (Nuclear Opalescence/opacity) | NO1 - NO6 | Degree of haziness/opacification |
| NC (Nuclear Color) | NC1 - NC6 | Degree of yellowing/browning |
- NO1/NC1 = trace - faint yellow
- NO2/NC2 = mild yellow
- NO3/NC3 = ocher (orange-yellow)
- NO4/NC4 = amber/orange
- NO5/NC5 = brown
- NO6/NC6 = black (brunescent nigra)
NO and NC usually coincide but do not have to. Grades are not always whole numbers; a lens may be recorded as NO3-NO4. The system also grades cortical (C1-C5) and posterior subcapsular opacities (P1-P5).
Oxford System
Uses a grading wheel with reference standards; less commonly used now.
Clinical slit-lamp grading (practical):
- Nuclear color is assessed with broad oblique slit beam and retroillumination.
- Darker color = harder nucleus = more surgical energy required.
- Brunescent (grade IV-V) cataracts have a high risk of posterior capsule rupture and endothelial cell loss.
2. Lid Anatomy
The eyelid is divided into anterior lamella, middle lamella, and posterior lamella (some authors use a two-layer anterior/posterior division).
Layers from anterior to posterior (Upper Eyelid)
- Skin - the thinnest skin in the body; no subcutaneous fat.
- Orbicularis oculi muscle (striated, facial nerve CN VII) - very vascular; subcutaneous fat is absent, so local anaesthetic should be placed just under the skin to avoid haematoma.
- Orbital septum - a fibrous diaphragm arising from the arcus marginalis along the superior orbital margin; fuses with the levator aponeurosis just above the tarsal plate.
- Preaponeurotic fat pad - lies immediately posterior to the orbital septum; key surgical landmark to identify the levator aponeurosis beneath it. Contains two compartments: medial (pale/white fat) and central/main fat pad.
- Levator aponeurosis - fibrous extension of the levator palpebrae superioris muscle; inserts into anterior surface of tarsus and skin at the level of the skin crease (creating the crease).
- Müller's muscle (superior tarsal muscle) - smooth muscle, sympathetically innervated (CN III for levator, but Müller's is adrenergic); arises from undersurface of levator muscle, inserts into upper border of tarsus; contributes ~2 mm to lid elevation.
- Tarsal plate - dense fibrous tissue providing structural rigidity; upper tarsus is 8-10 mm high, lower tarsus is 4-5 mm. Contains meibomian glands (modified sebaceous glands).
- Palpebral conjunctiva - tightly adherent to posterior tarsal surface.
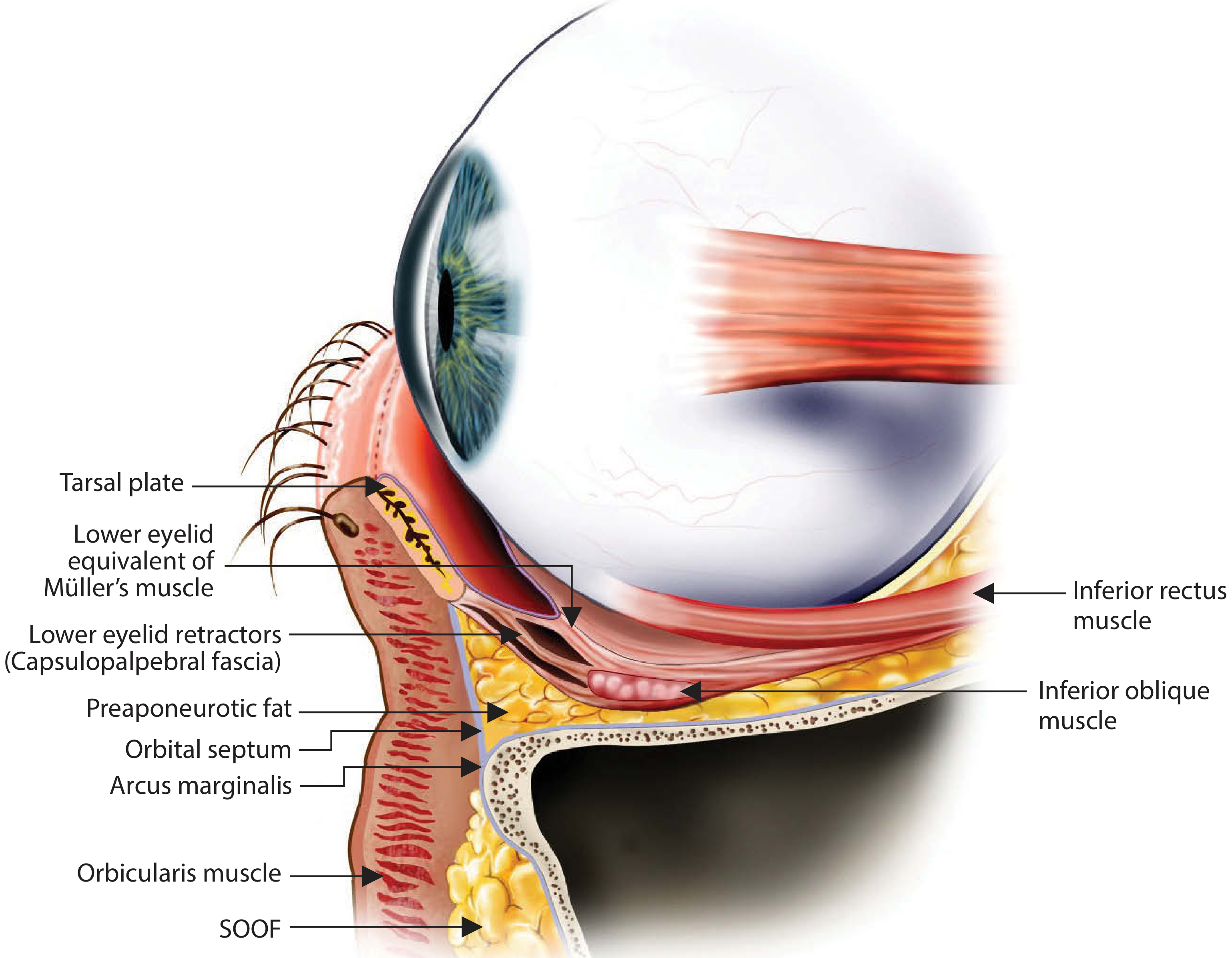
Lower Eyelid Layers (anterior to posterior)
- Skin
- Orbicularis oculi
- Orbital septum (arising from arcus marginalis inferiorly)
- Preaponeurotic fat (3 compartments: medial, central, lateral)
- Capsulopalpebral fascia (lower eyelid retractor - equivalent to levator aponeurosis)
- Lower eyelid equivalent of Müller's muscle
- Inferior tarsal plate (4-5 mm)
- Palpebral conjunctiva
Skin crease
- Males: ~5-6 mm above lash line; Females: ~7-8 mm above lash line.
- In East Asian eyelids, the orbital septum fuses lower on the levator aponeurosis, allowing preaponeurotic fat to descend and prevent a high skin crease.
Key landmarks
- Medial canthus: contains the lacrimal puncta, canaliculi, lacrimal sac; medial canthal tendon (anterior and posterior limbs).
- Lateral canthus: lateral canthal tendon attaches to Whitnall's tubercle on inner surface of the lateral orbital rim.
- Whitnall's ligament (superior transverse ligament): acts as a pulley for the levator.
- Lockwood's ligament (suspensory ligament of globe): suspends the globe from below.
- Inferior oblique muscle: passes between the medial and central fat compartments of the lower lid.
- Arcuate expansion: fascial extension of inferior oblique separating central and lateral fat compartments.
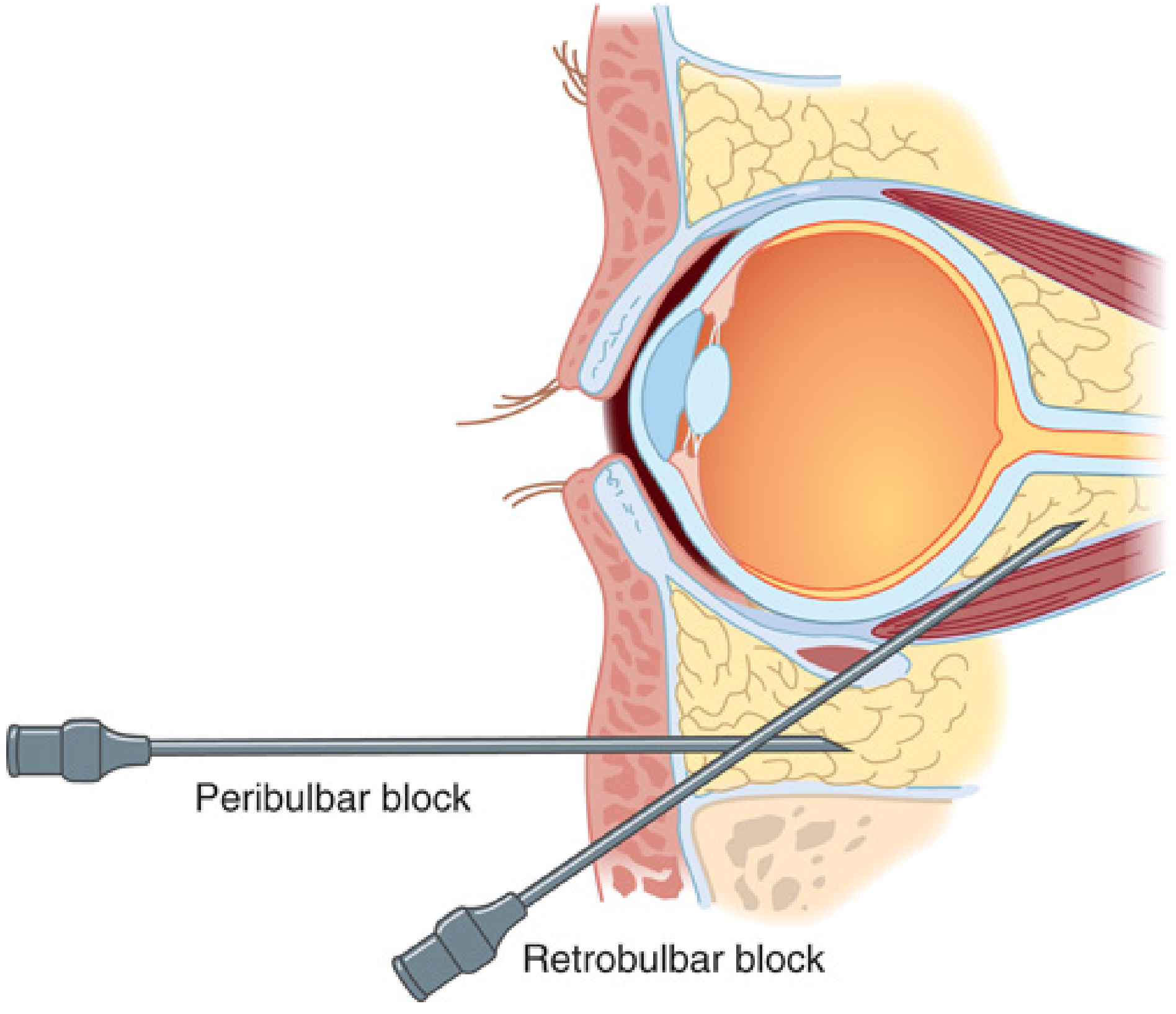
3. Peribulbar Block (Anaesthesia)
Background
Peribulbar (extraconal) block was first described in 1986 as an alternative to the retrobulbar block. The needle is placed outside the muscle cone, unlike retrobulbar block (intraconal injection). This greatly reduces the risk of optic nerve injury and retrobulbar haemorrhage.
Advantages over retrobulbar block
- No intraconal needle placement - lower risk of globe perforation, optic nerve damage, and retrobulbar haemorrhage
- Less pain on injection
- Safer in anticoagulated patients (relatively)
- No brainstem anaesthesia risk
Disadvantages
- Slower onset (5-15 min vs 3-5 min for retrobulbar)
- Greater volume of anaesthetic needed (5-10 mL vs 2-5 mL)
- More likely to cause chemosis and ecchymosis
- Akinesia may be incomplete - a second injection is often needed
Technique
Patient position: Supine, looking directly ahead (primary gaze). Topical anaesthetic drops applied to conjunctiva first.
Inferotemporal injection (first injection)
- Needle: 23-25 gauge, 25 mm; bevel up
- Entry point: Junction of the middle and lateral thirds of the lower lid margin, just above the inferior orbital rim
- Direction: Directed vertically backwards, parallel to the orbital floor (no angulation medially until past the equator of the globe)
- After passing the equator: redirect needle slightly medially (20°) and cephalad (10°)
- Depth: Less than 25 mm (avoid going beyond this to prevent intraconal placement)
- Volume: 5 mL of local anaesthetic injected
Superonasal injection (second injection, if needed)
- Entry: Through conjunctiva, medial to the caruncle, on the nasal side
- Direction: Straight back, parallel to the medial orbital wall, pointing slightly cephalad (20°)
- Volume: 5 mL
- Provides additional akinesia of the superior rectus and medial rectus
Local anaesthetic solution
- Commonly: Lignocaine 2% + bupivacaine 0.5% (1:1 mixture) ± hyaluronidase (to enhance spread and density of block; rare allergic reactions possible)
- Typical total volume: 5-10 mL per block
Ocular compression
- After injection, apply gentle ocular compression (Honan balloon or digital pressure) for 5-10 min to spread anaesthetic and soften the globe.
Facial nerve block (adjunct)
- Often added for akinesia of orbicularis oculi (to prevent lid squeeze, which raises IOP)
- Options:
- Modified Van Lint block: 1 cm lateral to orbital rim at superolateral and inferolateral margins; 2-4 mL
- Atkinson block: Inferior margin of zygomatic bone; needle 30° from vertical
- O'Brien block: At mandibular condyle (proximal trunk)
Complications
| Complication | Notes |
|---|---|
| Chemosis | Common; local spread of LA |
| Ecchymosis | More frequent than retrobulbar |
| Globe perforation | Less than retrobulbar; higher risk in axial length >25 mm |
| Retrobulbar haemorrhage | Rare; venous - usually self-limiting; arterial - may require surgery |
| Brainstem anaesthesia | Rare but can cause apnoea, cardiac arrest (usually with retrobulbar, rare with peribulbar) |
| Oculocardiac reflex | Bradycardia from globe pressure - atropine IV |
Sources: Miller's Anesthesia 10e, p.9731; Morgan & Mikhail's Clinical Anesthesiology 7e, p.1458
4. Lens-Induced Glaucoma
Lens-induced glaucoma encompasses a group of secondary glaucomas where the crystalline lens itself causes elevated intraocular pressure. There are three main types based on mechanism:
4.1 Phacolytic Glaucoma (Lens Protein Glaucoma)
Mechanism: Leakage of high-molecular-weight lens proteins through an intact capsule of a hypermature (Morgagnian) cataract - these proteins clog the trabecular meshwork and macrophages laden with lens material obstruct aqueous outflow. Open-angle mechanism.
Symptoms: Acute unilateral pain, redness, photophobia, decreased vision (sudden worsening on background of longstanding poor vision from mature cataract).
Signs (Critical):
- Markedly raised IOP
- Iridescent particles and white material in anterior chamber
- Hypermature (Morgagnian) or mature cataract with intact capsule
- Large white cells in AC (macrophages bloated with lens material)
- Pseudohypopyon possible
- Open angle on gonioscopy (clumps of macrophages in inferior angle)
Diagnosis: AC paracentesis - microscopy shows macrophages engulfing lens material.
Treatment:
- Medical (immediate IOP lowering): Topical β-blocker, α2-agonist, topical/systemic CAI (acetazolamide 500 mg), topical steroid (prednisolone acetate 1% q1h), cycloplegic, mannitol if needed
- Definitive: Cataract extraction (urgent, within 24-48 hrs if IOP uncontrolled). Glaucoma surgery usually not needed.
4.2 Lens Particle Glaucoma
Mechanism: Lens material liberated by trauma or surgery (lens capsule disrupted) directly obstructs the trabecular meshwork. Open-angle mechanism.
Symptoms: Pain, blurred vision, red eye - history of recent trauma or intraocular surgery.
Signs (Critical):
- White, fluffy pieces of lens cortex in the anterior chamber
- Raised IOP
- AC cell and flare, open angle on gonioscopy
Key distinction from phacolytic: Lens capsule is ruptured/disrupted (vs. intact in phacolytic).
Treatment: Medical IOP lowering; surgical removal of residual lens material if IOP not controlled medically.
4.3 Phacomorphic Glaucoma
Mechanism: A swollen (intumescent) cataractous lens physically pushes the iris forward, causing pupillary block and angle closure. Closed-angle mechanism.
Causes: Rapidly enlarging (intumescent) cataract or subluxated/dislocated lens.
Signs: Acute angle closure presentation - raised IOP, shallow anterior chamber (one side only, as it is unilateral), mid-dilated pupil, corneal oedema, congestion. Fellow eye has a deeper angle.
Treatment:
- Acute: IV mannitol, acetazolamide, topical IOP-lowering agents, pilocarpine to constrict pupil
- Laser iridotomy to break pupillary block
- Definitive: Cataract extraction (resolves the underlying cause)
4.4 Phacoantigenic Glaucoma (Phacoanaphylaxis)
Mechanism: Rare. Chronic granulomatous uveitis after prior sensitisation to lens material (following trauma or surgery). TM blockage by inflammatory cells and lens particles. Open-angle mechanism.
Signs: Granulomatous AC inflammation, latent period after lens material liberation. Rare glaucomatous optic neuropathy at presentation.
Treatment: Topical steroids + antiglaucoma medications; surgical lens removal if uncontrolled.
Summary Table: Lens-Induced Glaucoma
| Type | Mechanism | Capsule | Angle | Key feature |
|---|---|---|---|---|
| Phacolytic | Protein leakage | Intact | Open | Hypermature cataract; large cells in AC |
| Lens particle | Cortex obstruction | Disrupted | Open | White cortical fluffs post-trauma/surgery |
| Phacomorphic | Pupillary block (angle closure) | Intact | Closed | Swollen lens; shallow AC |
| Phacoantigenic | Immune-mediated TM block | Disrupted | Open | Granulomatous uveitis; prior sensitisation |
Sources: The Wills Eye Manual 9e, §9.12.1-9.12.3; Kanski's Clinical Ophthalmology 10e
This is a shared conversation. Sign in to Orris to start your own chat.