Urticaria uriens
Reading File
Finding Sources
Searching the Web
urticaria uriens clinical features pathophysiology treatment
Searching PubMed
urticaria uriens
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from Fitzpatrick's to write a thorough answer. Let me compose it.
Urticaria Uriens
Urticaria uriens is the classical Latin designation for ordinary urticaria - literally "stinging/burning urticaria," named after the burning sensation of the stinging nettle (Urtica dioica). The term is interchangeable with common urticaria, and in modern classification corresponds to what is now called spontaneous urticaria (acute or chronic). It is the prototypical form of the condition characterized by pruritic wheals with or without angioedema.
Etymology and Classification
The word "urticaria" derives from Urtica, the stinging nettle, and uriens (Latin: burning/stinging) emphasizes the characteristic burning-pruritic quality of the eruption. In current international guidelines (EAACI 2018), urticaria is classified by:
- Duration: Acute (<6 weeks) vs. Chronic (≥6 weeks)
- Mechanism: Spontaneous (no identifiable trigger) vs. Inducible (triggered by physical stimuli)
Urticaria uriens corresponds to the spontaneous subtype - wheals appearing without a consistent exogenous stimulus.
Clinical Features
Wheals in urticaria uriens have three defining characteristics:
- Central swelling of variable size (mm to several cm), surrounded by a reflex erythematous flare
- Intense pruritus or burning sensation (the "uriens" quality)
- Transient nature - individual lesions resolve within 1-24 hours without scarring, though new ones may continuously appear
Morphology is polymorphic - lesions can be round, annular ("flower-like"), arcuate, or polycyclic. Up to 50% of patients with spontaneous urticaria also develop angioedema - a deeper swelling in the dermis or submucosa, most often affecting eyelids, lips, tongue, and genitalia. Angioedema episodes typically last longer (hours to a few days).
The sensation is described as prickling, stinging, or burning, not just itching. Histamine is the primary mediator of pruritus, and H1-receptor antagonists generally suppress this sensation alongside the wheals themselves.
- Dermatology 2-Volume Set 5e
- Fitzpatrick's Dermatology, Vol. 1-2, Ch. 41
Pathophysiology
The fundamental event is mast cell degranulation in the dermis, releasing:
- Histamine (primary mediator) - causes vasodilation, increased vascular permeability via H1 and H2 receptor activation, and pruritus
- Arachidonic acid metabolites - prostaglandins (PGD2), leukotrienes (LTC4)
- Platelet-activating factor (PAF)
- Proinflammatory cytokines (including IL-31, which correlates with itch intensity)
Three main mechanisms activate mast cells:
1. Type I (IgE-mediated) hypersensitivity - antigen cross-links FcεRI-bound IgE on mast cells, activating signaling cascades (SYK → LAT → PLCγ → PKC) leading to degranulation. Accounts for <10% of urticaria cases (food, drugs, insect venom).
2. Autoimmune mechanism (autoallergic) - approximately 35-40% of CSU patients have IgG autoantibodies against:
- FcεRI (the high-affinity IgE receptor), or
- IgE itself These autoantibodies directly cross-link and activate mast cells, independent of antigen exposure. The autologous serum skin test (ASST) screens for this.
3. Non-IgE, non-autoimmune mechanisms - direct mast cell degranulation by drugs (NSAIDs, opioids, contrast media, vancomycin), infections, or unknown causes.
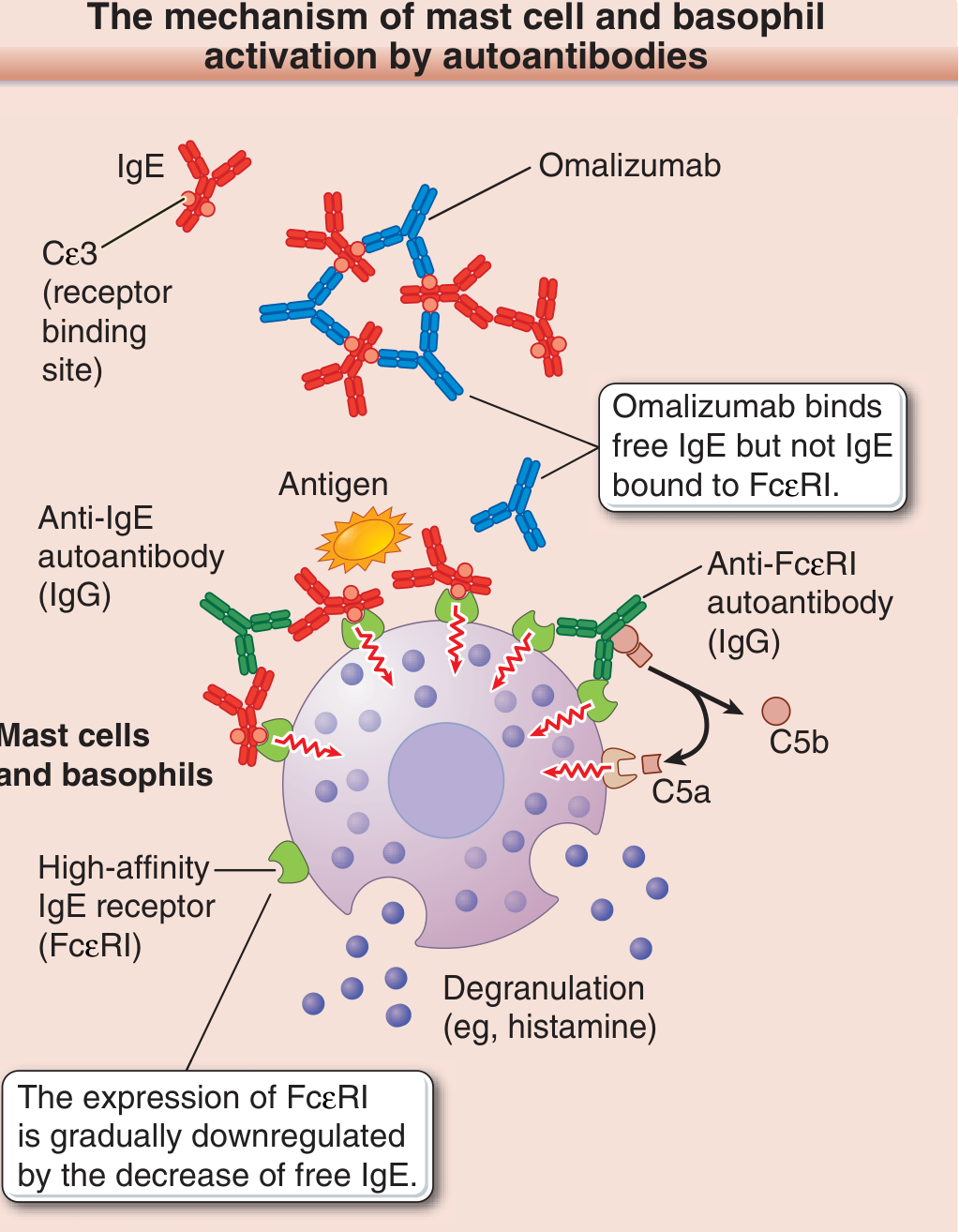
Figure: Mechanism of mast cell/basophil activation in autoimmune urticaria and omalizumab's mechanism of action - Fitzpatrick's Dermatology
Histopathology
- Dermal edema (the wheal itself)
- Perivascular infiltration of lymphocytes and eosinophils
- Mild to moderate dilation of small blood vessels and lymphatics
- No epidermal change (unlike eczema)
- Neutrophilic urticaria shows a predominantly neutrophilic infiltrate and is associated with autoinflammatory syndromes
- Urticarial vasculitis requires evidence of endothelial damage, fibrin deposition, and leukocytoclasis to distinguish it from ordinary urticaria
Causes and Triggers
| Category | Examples |
|---|---|
| Infections | Viral (especially in children), bacterial (H. pylori), parasitic |
| Foods | Nuts, seafood, eggs, milk (IgE-mediated); salicylates, food additives (pseudoallergens) |
| Drugs | β-lactam antibiotics, NSAIDs (COX-1 inhibitors), ACE inhibitors (angioedema), opioids, contrast media |
| Physical stimuli | Pressure, heat, cold, vibration, water, exercise |
| Autoimmune diseases | Thyroid autoimmunity, SLE, rheumatoid arthritis, Sjögren syndrome, celiac disease |
| Malignancy | Lymphoma, leukemia, carcinomas (especially in chronic urticaria) |
NSAIDs and aspirin deserve special mention: they can both induce and aggravate wheals by inhibiting COX-1, shifting arachidonic acid toward leukotriene synthesis. COX-2 selective NSAIDs are generally safer.
Diagnosis
Diagnosis is clinical - based on the characteristic morphology of evanescent wheals with pruritus. Key features:
- Each wheal lasts <24 hours (vs. urticarial vasculitis which persists >24 hours and leaves bruising)
- Complete blanching on pressure (positive diascopy)
- No epidermal change (scaling, vesicles) on the lesions
Workup for CSU (when acute cause not found):
- Minimum: CBC with differential, ESR/CRP
- Extended (based on history): H. pylori testing, thyroid function and antibodies (TPO-IgE), ASST, allergen-specific IgE, skin biopsy if vasculitis suspected, tryptase (for mastocytosis)
No extensive screening is recommended without a clinical indication.
Differential Diagnosis
| Condition | Key distinguishing feature |
|---|---|
| Urticarial vasculitis | Wheals >24 h, residual bruising, systemic symptoms, biopsy shows vasculitis |
| Erythema multiforme | Target lesions, fixed >24 h, mucous membrane involvement |
| Insect bites | Fixed, clustered, central punctum |
| Maculopapular mastocytosis | Darier's sign, orange-brown pigmented lesions |
| Schnitzler syndrome | Recurrent urticaria + monoclonal gammopathy + fever |
| CAPS (cryopyrin-associated) | Urticaria-like rash + fever + neutrophilic infiltrate |
| Drug eruption | Fixed timing to drug exposure, may not blanch |
| Angioedema HAE | Without wheals, bradykinin-mediated, antihistamine-resistant |
Prognosis
- Acute urticaria resolves in most patients within days to weeks; ~7% persist >1 year
- Chronic spontaneous urticaria (CSU): remission rates of ~37% at 1 year, ~51% at 2 years, ~66% at 5 years
- Factors associated with prolonged course: severe initial disease, presence of angioedema, coexisting physical urticaria, positive ASST (autoreactivity)
Management
The treatment algorithm follows a stepwise approach (EAACI 2018 guidelines):
Step 1 - First-line:
- 2nd-generation non-sedating H1-antihistamines (cetirizine, fexofenadine, loratadine, desloratadine, bilastine, rupatadine) - taken continuously, not on-demand, for CSU
- First-generation antihistamines are no longer recommended as first-line (sedation carry-over, paradoxical excitation risk in children)
- Trigger avoidance where identifiable
Step 2 - Second-line (antihistamine failure):
- Up-dosing H1-antihistamines up to 4x the standard dose - evidence shows improved pruritus control (though not always wheal reduction)
Step 3 - Third-line:
- Omalizumab 300 mg/month SC (anti-IgE monoclonal antibody) - now the preferred step 3 by EAACI guidelines
- Mechanism: binds free circulating IgE at the Cε3 domain, preventing FcεRI binding; secondarily downregulates FcεRI expression on mast cells/basophils
- Clinical effect can appear within 1 week despite FcεRI downregulation taking 2+ months
- Approved for CSU refractory to antihistamines; effective across virtually all mast cell-mediated subtypes
- Antileukotrienes (montelukast) may be added per BSACI/American guidelines as an alternative step 3
Step 4 - Fourth-line:
- Cyclosporine (immunosuppressive) for refractory autoimmune CSU
- Short courses of systemic corticosteroids for severe acute flares only; continuous use (>10 days) not recommended
Special note on bradykinin-mediated angioedema (HAE):
Antihistamines, corticosteroids, and adrenaline are ineffective. Treatment requires C1-INH concentrate, icatibant (bradykinin B2 receptor antagonist), or tranexamic acid for prophylaxis.
Sources: Fitzpatrick's Dermatology (9th ed.), Chapter 41 | Dermatology 2-Volume Set 5e
This is a shared conversation. Sign in to Orris to start your own chat.