skeleton system for assesment
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Now I have enough material from the textbooks. Let me compile a comprehensive skeletal system assessment.
Skeletal System - Assessment Guide
Sources: Gray's Anatomy for Students; Robbins & Kumar Basic Pathology; General Anatomy and Musculoskeletal System (THIEME Atlas); Campbell's Operative Orthopaedics 15th Ed 2026
1. Overview of the Skeletal System
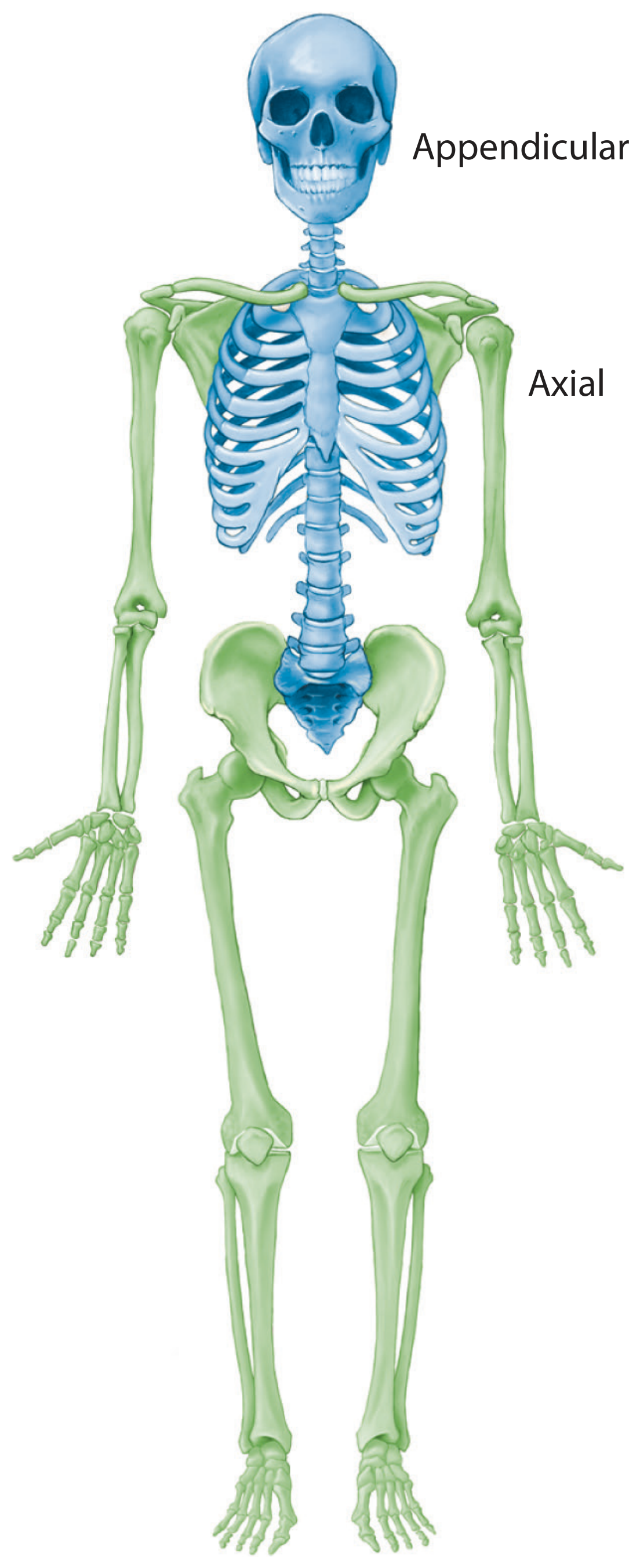
The skeletal system consists of bone and cartilage. The adult human body contains 206 bones. The skeleton is divided into two main subdivisions:
| Division | Components | Bone Count |
|---|---|---|
| Axial skeleton | Skull (cranium), vertebral column, ribs, sternum | 80 bones |
| Appendicular skeleton | Upper & lower limbs + their girdles (pectoral & pelvic) | 126 bones |
- Gray's Anatomy for Students, p. 29
2. Functions of the Skeleton
Bones serve five key functions (mnemonic: SPRLC):
- Support - structural framework for the body
- Protection - protects vital organs (skull → brain; ribs → heart/lungs)
- Reservoir - calcium and phosphorus storage (homeostasis)
- Lever - muscles act on bones to produce movement
- Container - marrow cavity houses blood-forming (hematopoietic) cells
- Gray's Anatomy for Students; Robbins & Kumar Basic Pathology, p. 770
3. Bone Classification by Shape
| Type | Description | Example |
|---|---|---|
| Long bones | Tubular, longer than wide | Humerus, femur, tibia |
| Short bones | Cuboidal | Carpals (wrist), tarsals (ankle) |
| Flat bones | Two compact plates + spongy bone | Skull, sternum, scapula |
| Irregular bones | Variable, complex shapes | Vertebrae, facial bones |
| Sesamoid bones | Round/oval, develop within tendons | Patella |
- Gray's Anatomy for Students, p. 29
4. Bone Tissue Types
Compact (Cortical) Bone
- Dense outer shell of all bones
- Arranged in osteons (Haversian systems)
- High mechanical strength
Spongy (Cancellous/Trabecular) Bone
- Network of trabeculae enclosing marrow cavities
- Found in epiphyses of long bones and interior of flat bones
- Contains red bone marrow (hematopoiesis)
Bone Matrix Composition
- Organic component (osteoid) - 35%: Primarily type I collagen + glycosaminoglycans
- Mineral component - 65%: Hydroxyapatite (gives hardness)
5. Bone Cells
| Cell | Origin | Function |
|---|---|---|
| Osteoblasts | Mesenchymal stem cells (periosteum/medullary space) | Synthesize and assemble bone matrix; regulate mineralization |
| Osteocytes | Derived from osteoblasts (trapped in matrix) | Calcium/phosphate regulation; detect mechanical forces; trigger remodeling |
| Osteoclasts | Circulating monocytes (multinucleate macrophages) | Bone resorption - secrete acid + proteases (MMPs) into resorption pit |
- Robbins & Kumar Basic Pathology, p. 770
6. Bone Development
| Type | Process | Where |
|---|---|---|
| Endochondral ossification | Bone replaces a cartilage template (anlage) | Long bones, vertebrae, pelvis |
| Intramembranous ossification | Bone forms directly from mesenchymal tissue (no cartilage stage) | Flat bones of skull, clavicle |
Growth plate (physis): The cartilage plate trapped between the primary (diaphysis) and secondary (epiphysis) ossification centers. Active during childhood/adolescence; fuses at skeletal maturity.
7. Cartilage Types
| Type | Key Features | Location |
|---|---|---|
| Hyaline | Most common; moderate collagen | Articular surfaces, costal cartilage, trachea |
| Elastic | Collagen + elastic fibers; flexible | External ear (pinna), epiglottis |
| Fibrocartilage | Dense collagen; high tensile strength | Intervertebral discs, pubic symphysis, menisci |
Important: Cartilage is avascular, alymphatic, and aneural - nourished entirely by diffusion. This is why it heals poorly after injury.
- Gray's Anatomy for Students, p. 29
8. Bone Remodeling
Bone is a dynamic tissue undergoing continuous remodeling throughout life via the Basic Multicellular Unit (BMU):
- Activation - osteoclast precursors recruited
- Resorption - osteoclasts remove old bone
- Reversal - transition from resorption to formation
- Formation - osteoblasts deposit new osteoid
- Mineralization - osteoid calcifies
Regulation: Parathyroid hormone (PTH) → ↑ resorption | Calcitonin → ↓ resorption | Vitamin D → ↑ absorption | Estrogen → ↓ resorption
9. Fracture Healing
Fracture healing occurs in two forms:
Indirect (Secondary) Fracture Healing - most common
- Inflammatory phase - fracture hematoma formation
- Granulation stage - organization of hematoma with vessel-rich connective tissue
- Soft callus - fibrocartilaginous callus from periosteum/endosteum cells
- Hard callus - callus mineralization (6-8 weeks post fracture)
- Remodeling - woven bone → lamellar bone (takes months)
Direct (Primary) Fracture Healing
- Requires surgical fixation + fracture gap ≤ 0.5 mm
- No cartilage callus; direct osteon bridging across the fracture
Complication: Pseudarthrosis = failure of bone union after 6 months. Caused by excessive mechanical load or poor vascular supply.
- General Anatomy and Musculoskeletal System, THIEME Atlas, p. 74
10. Key Joints Overview
| Joint Type | Structure | Example | Movement |
|---|---|---|---|
| Fibrous (synarthrosis) | Fibrous tissue only | Skull sutures | None/minimal |
| Cartilaginous (amphiarthrosis) | Cartilage bridge | Intervertebral discs, pubic symphysis | Limited |
| Synovial (diarthrosis) | Joint capsule + synovial fluid | Hip, knee, shoulder | Full range |
Synovial Joint Subtypes:
- Hinge - flexion/extension only (elbow, knee, ankle)
- Ball-and-socket - widest ROM (hip, shoulder)
- Pivot - rotation (atlantoaxial joint, proximal radioulnar)
- Condyloid - biaxial movement (wrist, MCP joints)
- Saddle - biaxial + rotation (1st carpometacarpal - thumb)
- Plane/Gliding - sliding only (acromioclavicular, intertarsal)
11. Clinical Assessment Points
History
- Pain: location, onset, character, radiation, aggravating/relieving factors
- Swelling, deformity, loss of function
- Trauma mechanism (direct vs. indirect force)
- Previous fractures, bone diseases, family history (osteoporosis)
- Medications: steroids (osteoporosis risk), bisphosphonates
Physical Examination Sequence: LOOK - FEEL - MOVE
| Step | What to Assess |
|---|---|
| Look | Deformity, swelling, bruising, skin changes, muscle wasting, posture, gait |
| Feel | Tenderness (point vs. diffuse), warmth, crepitus, bony landmarks |
| Move | Active ROM first → then passive → then against resistance; note pain and limitation |
Neurovascular Assessment (CRITICAL after trauma)
- 5 P's: Pain, Pallor, Pulselessness, Paresthesia, Paralysis (compartment syndrome)
Special Tests
- Straight leg raise (SLR) - lumbar nerve root compression
- FABER test - hip/SI joint pathology
- McMurray's test - meniscal tears (knee)
- Apprehension test - patellar/shoulder instability
- Finkelstein's test - De Quervain's tenosynovitis
12. Common Skeletal Pathologies (Assessment Context)
| Condition | Key Features | Assessment Finding |
|---|---|---|
| Osteoporosis | ↓ bone mass, normal mineralization; postmenopausal/elderly | DEXA scan T-score ≤ -2.5; fragility fractures |
| Osteoarthritis | Cartilage degeneration; wear-and-tear | Joint line tenderness, crepitus, ↓ ROM, bony osteophytes |
| Rheumatoid arthritis | Autoimmune synovitis; symmetric joint inflammation | Swollen, warm, tender joints; morning stiffness >1 hr |
| Osteomyelitis | Bone infection (Staph aureus most common) | Local warmth, swelling, tenderness; fever; ↑ WBC, CRP, ESR |
| Rickets/Osteomalacia | ↓ mineralization (Vit D deficiency) | Bowing of legs in children; bone pain; pseudofractures |
| Paget's disease | Abnormal remodeling; ↑ osteoclast activity | Bony enlargement, deformity, pain; ↑ ALP |
13. Imaging Modalities for Skeletal Assessment
| Modality | Best For |
|---|---|
| X-ray (plain film) | Fractures, alignment, joint space, osteoporosis |
| CT scan | Complex fractures, spinal injury, 3D reconstruction |
| MRI | Soft tissue (ligaments, cartilage, marrow), stress fractures |
| Bone scan (scintigraphy) | Metastases, occult fractures, osteomyelitis |
| DEXA scan | Bone mineral density (osteoporosis) |
| Ultrasound | Soft tissue, tendons, bursae |
Quick Reference: Bone Count by Region
| Region | Bones |
|---|---|
| Skull | 22 (8 cranial + 14 facial) |
| Vertebral column | 26 (7 cervical, 12 thoracic, 5 lumbar, 1 sacrum, 1 coccyx) |
| Thoracic cage | 25 (12 pairs ribs + 1 sternum) |
| Upper limb (each) | 32 (clavicle, scapula, humerus, radius, ulna, 8 carpals, 5 metacarpals, 14 phalanges) |
| Lower limb (each) | 31 (hip, femur, patella, tibia, fibula, 7 tarsals, 5 metatarsals, 14 phalanges) |
This covers the core content needed for a skeletal system assessment - from basic anatomy and physiology through clinical evaluation and common pathologies. Let me know if you want any section expanded (e.g., specific joints, fracture types, bone tumors, or a particular region like the spine or pelvis).
skeleton system
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Finding Sources
Reading File
Loading Image
I now have rich textbook content and diagrams. Here is your full skeletal system study notes overview.
The Skeletal System - Full Study Notes
Sources: Gray's Anatomy for Students; Miller's Review of Orthopaedics 9th Ed; Firestein & Kelley's Textbook of Rheumatology; Robbins & Kumar Basic Pathology; Tintinalli's Emergency Medicine
1. Introduction
The skeletal system consists of bone and cartilage. Together they form the structural framework of the entire body. The adult human skeleton contains 206 bones total:
- 80 bones in the axial skeleton
- 126 bones in the appendicular skeleton
2. Divisions of the Skeleton
Axial Skeleton (80 bones)
| Region | Bones | Count |
|---|---|---|
| Skull | Cranium (8) + Facial bones (14) | 22 |
| Auditory ossicles | Malleus, incus, stapes (×2) | 6 |
| Hyoid | Hyoid bone | 1 |
| Vertebral column | 7C + 12T + 5L + sacrum + coccyx | 26 |
| Thoracic cage | 12 pairs ribs + sternum | 25 |
Appendicular Skeleton (126 bones)
| Region | Bones |
|---|---|
| Upper limb (×2) | Clavicle, scapula, humerus, radius, ulna, 8 carpals, 5 metacarpals, 14 phalanges = 32 each |
| Lower limb (×2) | Hip (os coxa), femur, patella, tibia, fibula, 7 tarsals, 5 metatarsals, 14 phalanges = 31 each |
3. Functions of Bone (mnemonic: SPRLC)
- Support - structural framework of the body
- Protection - protects viscera (skull → brain; ribs → heart/lungs; vertebrae → spinal cord)
- Reservoir - stores calcium (99% of body's Ca²⁺) and phosphorus
- Levers - muscles act on bones to produce movement
- Containers - medullary cavities house bone marrow (hematopoiesis)
4. Classification of Bones by Shape
| Type | Description | Examples |
|---|---|---|
| Long | Tubular; length > width | Femur, humerus, tibia, radius |
| Short | Cuboidal | Carpals, tarsals |
| Flat | Two cortical plates + spongy bone | Skull, sternum, scapula, ribs |
| Irregular | Complex, variable shape | Vertebrae, facial bones, hip |
| Sesamoid | Round/oval; develop within tendons | Patella (largest), sesamoids of thumb |
Clinical note: Accessory and sesamoid bones are normal variants commonly found in wrists, hands, ankles, and feet - do not mistake them for fractures on imaging.
5. Anatomy of a Long Bone
| Region | Description |
|---|---|
| Epiphysis | Expanded ends; covered by articular cartilage; contains spongy bone |
| Physis (growth plate) | Cartilaginous zone between epiphysis and metaphysis; site of longitudinal growth; fuses at skeletal maturity |
| Metaphysis | Flared zone between physis and diaphysis; transition region |
| Diaphysis | Midshaft; mostly compact bone; encloses medullary (marrow) cavity |
| Periosteum | Fibrous membrane covering outer bone surface; inner (cambium) layer is osteogenic |
| Endosteum | Thin membrane lining the medullary cavity; also osteogenic |
| Apophysis | Bony outgrowth serving as muscle/ligament attachment point (e.g., greater trochanter) |
- Tintinalli's Emergency Medicine, p. 946
6. Bone Tissue Types
Compact (Cortical) Bone
- Dense outer shell of all bones
- Organized in osteons (Haversian systems) - concentric lamellae around a central Haversian canal
- Haversian canals carry blood vessels and nerves; connected laterally by Volkmann's canals
- Provides tensile and compressive strength
Spongy (Cancellous/Trabecular) Bone
- Lattice-like trabeculae with interconnecting spaces filled with marrow
- Located in epiphyses of long bones and interior of flat/irregular bones
- Trabecular arrangement follows lines of mechanical stress (Wolff's Law)
- Most bone remodeling occurs here
Bone Marrow
| Type | Composition | Location |
|---|---|---|
| Red marrow | 40% water, 40% fat, 20% protein; hematopoietically active | Axial skeleton, epiphyses in children |
| Yellow marrow | 15% water, 80% fat, 5% protein; inactive | Appendicular skeleton in adults |
Red marrow converts to yellow marrow with age, starting first in the appendicular skeleton and then the axial skeleton.
- Miller's Review of Orthopaedics, 9th Ed
7. Bone Matrix Composition
| Component | % of Dry Weight | Role |
|---|---|---|
| Organic (osteoid) | 35-40% | Type I collagen (tensile strength) + proteoglycans |
| Inorganic (mineral) | 60-65% | Calcium hydroxyapatite [Ca₁₀(PO₄)₆(OH)₂] - provides compressive strength |
Two structural forms of bone matrix:
- Woven bone - disorganized collagen; produced rapidly (fetal development, fracture repair); mechanically inferior; always abnormal in adults unless repairing
- Lamellar bone - parallel collagen fibers; organized, mechanically strong; normal adult bone
8. Bone Cells
| Cell | Origin | Location | Function |
|---|---|---|---|
| Osteoblasts | Mesenchymal stem cells (periosteum/endosteum) | Bone surface | Synthesize osteoid; regulate mineralization |
| Osteocytes | Trapped osteoblasts | Within lacunae in matrix | Mechanosensing; Ca²⁺/PO₄ regulation; initiate remodeling signals via canalicular network |
| Osteoclasts | Monocyte/macrophage lineage (multinucleate) | Bone surface (resorption pit) | Bone resorption via acid + matrix metalloproteinases |
| Bone lining cells | Quiescent osteoblasts | Bone surface | Maintain ionic environment; regulate remodeling |
9. Bone Blood Supply
Long bones receive blood from three systems:
| System | Pressure | Supplies |
|---|---|---|
| Nutrient artery | High pressure | Inner 2/3 of cortex via Haversian system; enters through nutrient foramen → medullary canal |
| Metaphyseal-epiphyseal | Moderate | From periarticular vascular plexus |
| Periosteal | Low pressure | Outer 1/3 of cortex |
-
Arterial flow in mature bone is centrifugal (inside → outside)
-
Venous flow is centripetal (outside → inside)
-
Bones with tenuous blood supply (high avascular necrosis risk): scaphoid, talus, femoral head, odontoid
-
Miller's Review of Orthopaedics, 9th Ed
10. Cartilage
Cartilage is an avascular, alymphatic, aneural connective tissue nourished entirely by diffusion.
| Type | Matrix | Location |
|---|---|---|
| Hyaline | Moderate collagen + chondroitin sulfate | Articular surfaces, costal cartilage, trachea, growth plate |
| Elastic | Collagen + abundant elastic fibers | External ear (pinna), epiglottis, larynx |
| Fibrocartilage | Dense type I collagen; few cells | Intervertebral discs, pubic symphysis, knee menisci, TMJ disc |
Functions of cartilage:
- Supports soft tissues
- Provides smooth gliding surface at joints
- Enables growth of long bones (growth plate)
11. Bone Development (Ossification)
| Type | Process | Bones |
|---|---|---|
| Intramembranous | Bone forms directly from mesenchyme (no cartilage template) | Flat bones of skull, mandible, clavicle |
| Endochondral | Bone replaces a cartilage anlage (model) | All long bones, vertebrae, pelvis, ribs |
Endochondral ossification centers:
- Primary center - appears in diaphysis; present at birth in most bones
- Secondary centers - appear in epiphyses postnatally; important for growth; frequently the site of pediatric physeal fractures
12. Bone Remodeling
Bone is continuously remodeled throughout life. The entire adult skeleton is replaced every 7-10 years.
The remodeling cycle (Basic Multicellular Unit / BMU):
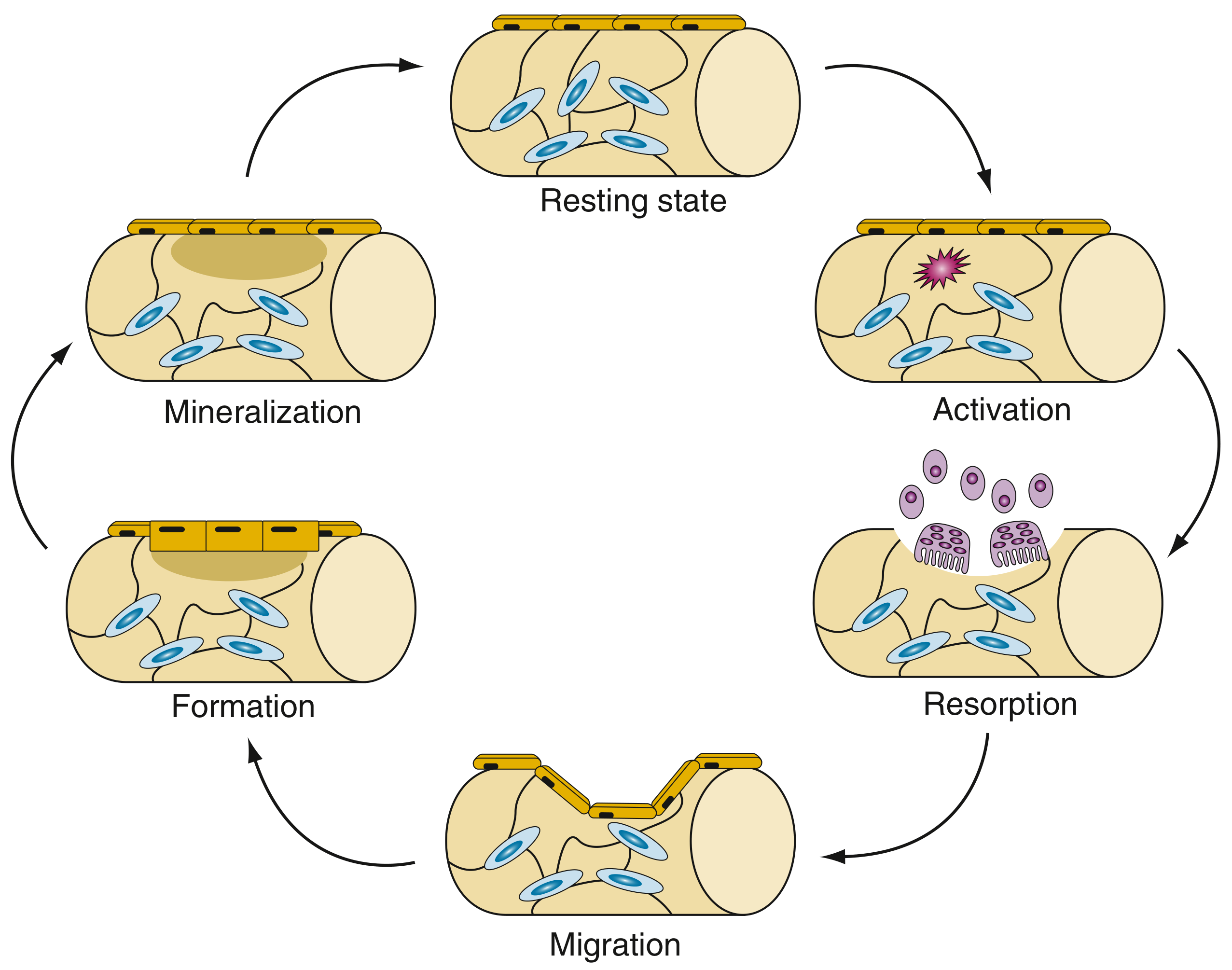
Steps:
- Activation - osteocytes sense micro-damage; sclerostin levels fall; osteoclast precursors recruited
- Resorption - osteoclasts excavate a resorption lacuna
- Migration - mesenchymal stem cells (MSCs) migrate into the lacuna
- Formation - osteoblasts deposit new osteoid
- Mineralization - osteoid calcifies; osteoblasts become osteocytes or lining cells
- Resting state - cycle complete
Full cycle takes 3-6 months. Most remodeling occurs in trabecular bone.
Regulation:
| Factor | Effect |
|---|---|
| PTH (↑) | ↑ resorption (indirect via osteoblast RANKL) |
| Calcitonin | ↓ resorption |
| Vitamin D | ↑ Ca²⁺ absorption; facilitates mineralization |
| Estrogen | ↓ resorption (protective); loss at menopause → osteoporosis |
| Mechanical loading | ↑ bone formation (Wolff's Law) |
- Firestein & Kelley's Textbook of Rheumatology, p. 107
13. Joints (Arthrology)
Joints are classified by degree of movement:
| Class | Type | Structure | Movement | Example |
|---|---|---|---|---|
| Synarthrosis | Fibrous | Fibrous tissue | None | Skull sutures, tooth sockets (gomphosis) |
| Amphiarthrosis | Cartilaginous | Hyaline cartilage (synchondrosis) or fibrocartilage (symphysis) | Limited | Pubic symphysis, intervertebral discs, sternal joints |
| Diarthrosis | Synovial | Joint capsule + synovial membrane + fluid | Full range | Hip, knee, shoulder, elbow |
Synovial Joint Structure
- Articular cartilage - hyaline cartilage on bone ends; no nerve supply
- Joint capsule - fibrous outer layer + inner synovial membrane
- Synovial membrane - secretes synovial fluid (lubricant + nutrient supply to cartilage)
- Ligaments - reinforce capsule; guide/limit movement
- Bursae - fluid-filled sacs that reduce friction near joints
- Menisci/discs - fibrocartilage structures that improve joint congruity (e.g., knee)
Synovial Joint Subtypes
| Type | Movement | Example |
|---|---|---|
| Hinge | Flexion/extension (uniaxial) | Elbow, knee, ankle, interphalangeal |
| Pivot | Rotation only | Atlantoaxial (C1-C2), proximal radioulnar |
| Ball-and-socket | Multiaxial (widest ROM) | Hip, shoulder (glenohumeral) |
| Condyloid/Ellipsoid | Biaxial (flex/ext + abd/add) | Wrist (radiocarpal), MCP joints |
| Saddle | Biaxial + opposition | 1st carpometacarpal (thumb) |
| Plane/Gliding | Sliding/translational | Acromioclavicular, intertarsal, intercarpal |
14. Fracture Healing
Indirect (Secondary) Healing - most common
| Stage | Events | Timing |
|---|---|---|
| Inflammatory | Fracture hematoma; neutrophils, macrophages, T/B cells; debridement of devitalized tissue | Days 1-7 |
| Fibrovascular | Angiogenesis; MSC recruitment; soft tissue bridging | Days 7-14 |
| Soft callus | Fibrocartilaginous callus from periosteum/endosteum cells | Weeks 2-6 |
| Hard callus | Callus mineralization; woven bone | Weeks 6-8 |
| Remodeling | Woven bone → lamellar bone | Months to years |
Direct (Primary) Healing
- Requires surgical fixation + fracture gap ≤ 0.5 mm
- No cartilage callus; osteonal bridging directly crosses the fracture
- Rarely achieved without anatomic reduction and rigid fixation
Key complication: Pseudarthrosis = failure of bone union after 6 months (from excessive movement or poor vascularity)
15. Common Skeletal Conditions (Summary)
| Condition | Pathology | Key Features |
|---|---|---|
| Osteoporosis | ↓ bone mass (normal mineralization) | T-score ≤ -2.5; fragility fractures (vertebra, hip, wrist) |
| Osteomalacia / Rickets | ↓ mineralization (Vit D deficiency) | Bone pain; bowing in children; pseudofractures |
| Osteoarthritis | Articular cartilage degeneration | Joint pain, crepitus, ↓ ROM, osteophytes |
| Rheumatoid Arthritis | Autoimmune synovitis | Symmetric joint swelling, morning stiffness >1 hr |
| Osteomyelitis | Bone infection (Staph aureus #1) | Local pain, warmth, swelling; fever; ↑ ESR/CRP |
| Paget's Disease | Abnormal remodeling (↑ osteoclasts then ↑ osteoblasts) | Bone enlargement, pain, deformity; ↑ ALP |
| Osteonecrosis (AVN) | Infarction of bone | Pain; collapse of femoral head most common |
Quick Summary Table
| Feature | Detail |
|---|---|
| Total adult bones | 206 |
| Axial skeleton | 80 bones (skull, spine, thorax) |
| Appendicular skeleton | 126 bones (limbs + girdles) |
| Bone matrix organic | 35% - type I collagen (flexibility) |
| Bone matrix inorganic | 65% - hydroxyapatite (hardness) |
| Bone remodeling cycle | 3-6 months; skeleton fully renewed every 7-10 years |
| Avascular cartilage types | All 3 (hyaline, elastic, fibrocartilage) |
| Ossification types | Intramembranous (skull) vs. Endochondral (long bones) |
Let me know if you want to go deeper on any specific area - joints, individual regions (spine, upper/lower limb), bone diseases, or fracture types.
This is a shared conversation. Sign in to Orris to start your own chat.