I am gastro resident Give IPCL pattern of esophagus with images
Reading File
Finding Sources
Searching the Web
IPCL pattern classification esophagus NBI endoscopy Inoue classification images
Reading File
Loading Image
Loading Image
Loading Image
Reading Web Page
https://www.e-ce.org/journal/view.php?doi=10.5946%2Fce.2021.…
Loading Image
Loading Image
Loading Image
Excellent - I now have all the images and information needed. Here is the comprehensive IPCL pattern guide:
IPCL (Intraepithelial Papillary Capillary Loop) Pattern Classification - Esophagus
What is IPCL?
The IPCL is a capillary that arises from the fourth branch of the arborescent subepithelial vessels, forms single loops within the epithelial papillae, and is visible under magnifying NBI endoscopy (ME-NBI). In normal squamous epithelium, IPCLs are regular, small, and uniform. With progressive neoplastic transformation, they undergo stepwise morphological changes in four parameters:
D - T - C - V: Dilation | Tortuosity | Change in Caliber | Variation in shape
Classification Systems
Two main classifications are in use:
| Inoue (Original 2001) | JES Classification (2017) | |
|---|---|---|
| Basis | 5 types (I-VN) | 2 types (A and B) |
| Clinical use | Japan, academic | Current international standard |
Inoue IPCL Classification (Original)
Below is the full Inoue classification showing endoscopic images, schematics, pathological correlation, and treatment implication:
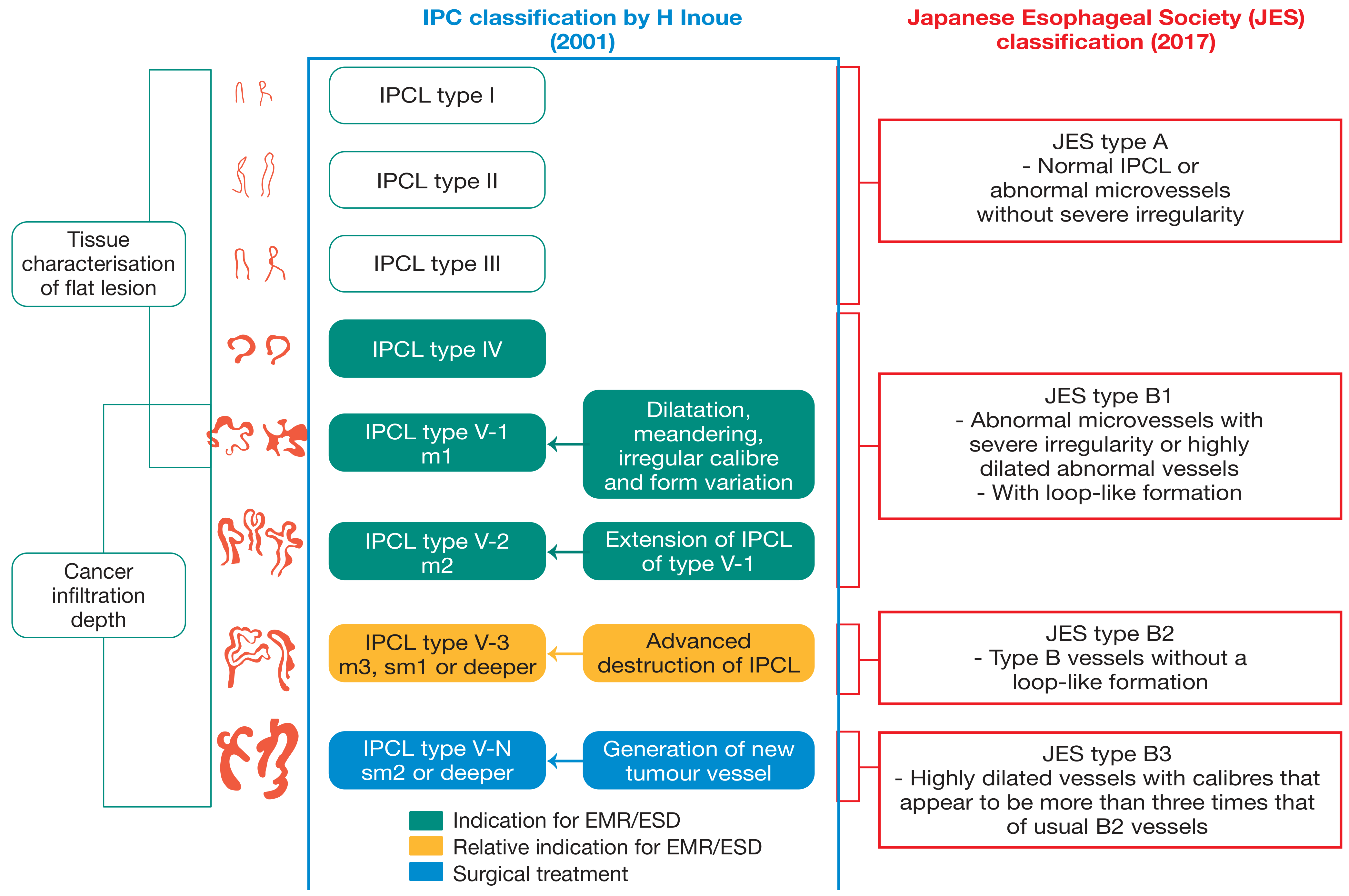
From Bailey & Love's Short Practice of Surgery, 28th Ed., Fig. 66.45 - IPCL classification showing depth of invasion and treatment indication
Type-by-Type Breakdown (Inoue)
| Type | Morphology | Histology / Depth | Treatment |
|---|---|---|---|
| Type I | Normal regular loops; small, uniform, hairpin shape | Normal squamous epithelium | None |
| Type II | Elongation + mild dilation | Esophagitis / reactive change | None / treat inflammation |
| Type III | Increased elongation, mild caliber change | Inflammation / Low-grade intraepithelial neoplasia (LGIN) | Observe / endoscopic treatment |
| Type IV | Increased caliber + elongation toward epithelial surface | Borderline HGIN / definite carcinoma | Endoscopic treatment |
| Type V-1 | 4 features: dilation + tortuosity + irregular caliber + non-uniformity (loop intact) | Carcinoma in situ (M1, EP) | EMR/ESD |
| Type V-2 | V-1 features + elongation in vertical plane | M2 (lamina propria invasion, LPM) | EMR/ESD |
| Type V-3 | Horizontal spread + loss of loop arrangement (destruction of IPCL) | M3/SM1 (muscularis mucosa/superficial submucosa) | ESD (relative indication); surgery if SM suspected |
| Type VN | Vessel diameter ~3x Type V-3; new tumor vessel formation | SM2 or deeper (deep submucosal) | Surgery |
JES Classification (Japan Esophageal Society, 2017) - Current Standard
The JES classification simplifies Inoue into a more clinically actionable 2-tier system:
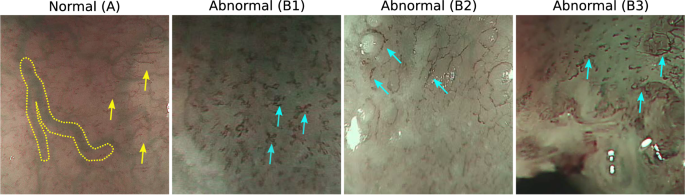
JES Classification: Type A (normal), B1 (loop present), B2 (loop lost), B3 (highly dilated)
JES Type A - Normal/Benign
- Normal IPCL OR abnormal microvessels without severe irregularity (3 or fewer morphological factors)
- Vessel caliber: 7-10 µm
- Corresponds to: Normal epithelium, inflammation, LGIN
- No invasion
JES Type B - Abnormal (subdivided)
Morphological factors for "severe irregularity" = ALL 4 of: tortuosity + dilation + irregular caliber + various shapes
| Subtype | Description | Caliber | Depth | Histology |
|---|---|---|---|---|
| B1 | Abnormal microvessels with severe irregularity + loop-like formation preserved | ~20 µm | T1a (EP or LPM) = M1/M2 | HGIN, invasive SCC |
| B2 | Type B vessels + loss of loop-like formation | Variable | T1a (MM) or T1b (SM1) = M3/SM1 | Invasive SCC |
| B3 | Highly dilated vessels; caliber >3x that of B2 | >60 µm | T1b (SM2) or deeper | Invasive SCC |
Clinical Endoscopic Images
Below are actual endoscopic images showing early squamous cell cancer detected with NBI:
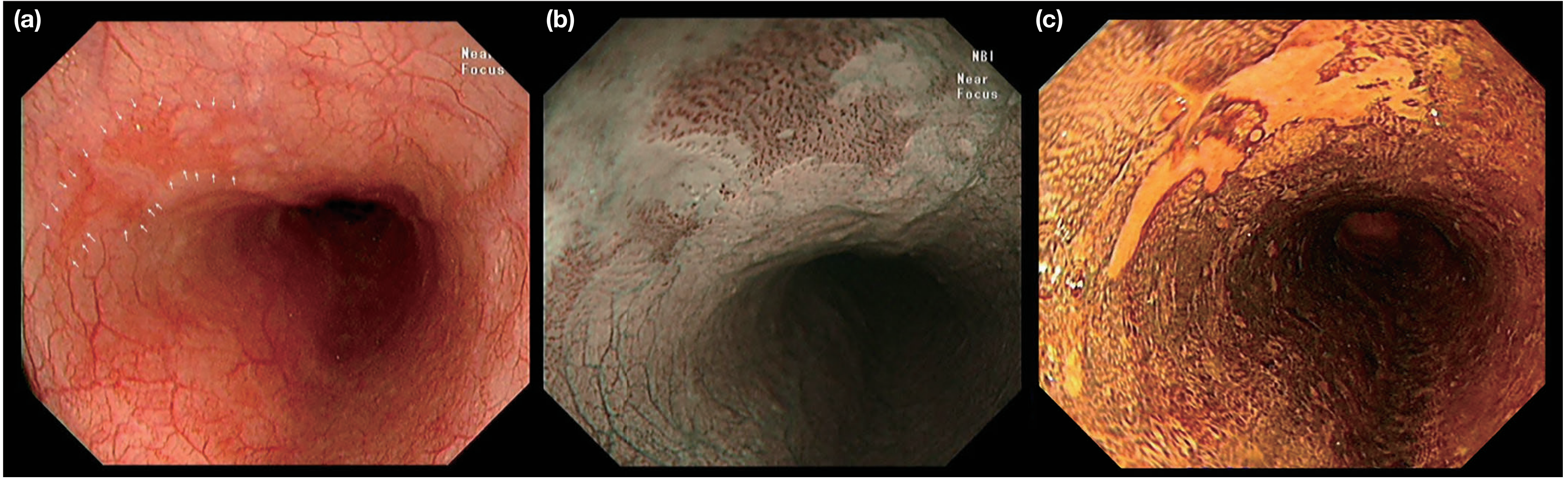
Fig. 66.44 from Bailey & Love's - (a) White light: suspicious lesion with white arrows; (b) NBI near-focus: abnormal IPCLs visible; (c) Lugol's chromoendoscopy: lesion unstained (iodine-negative)
Inoue + JES Correlation (Summary Diagram)
The comprehensive figure below shows both Inoue (original) and JES classifications side by side with endoscopic images, schematics, pathology, and treatment indication:

(A) Inoue classification; (B) Arima classification; (C) JES classification with vessel calibers. Note: shaded oval = "formation of area" (loss of individual loop structure)
Key Points for Clinical Practice
1. When to use ME-NBI:
- Any reddish or discolored flat lesion on white light
- Lugol's iodine-negative (LCL) areas
- Screening in high-risk patients (alcohol + smoking)
2. Treatment decision algorithm:
Type A / IPCL I-III → Observe or treat inflammation
IPCL IV / JES B1 → EMR or ESD (curative)
JES B2 / IPCL V-3 → ESD (if <2 cm) or surgery
JES B3 / IPCL V-N → Surgery ± neoadjuvant therapy
3. Four morphological factors to assess in every lesion (DTCV):
- D - Dilation
- T - Tortuosity
- C - Caliber irregularity
- V - Variation in shape (non-uniformity)
3 or fewer factors = JES Type A (benign/low-grade)
All 4 factors = JES Type B (neoplastic) - then subclassify B1/B2/B3 by loop status and caliber
4. NBI technical note:
- NBI uses 415 nm (blue) and 540 nm (green) wavelengths
- These are absorbed preferentially by hemoglobin, enhancing visualization of superficial capillaries
- Magnification (x80-115) is required for accurate IPCL assessment
Sources: Bailey & Love's Short Practice of Surgery 28th Ed. p.1158; Current Status of Image-Enhanced Endoscopy (2021); NBI classification review - QIMS
This is a shared conversation. Sign in to Orris to start your own chat.