A 70 year old male patient with history of stage 4 Pancreatic cancer is consulting with intractable pain abdomen . Write about: 1. Principles of chronic pain management 2. Pharmacological management of chronic pain 3. Ascending and descending pathways of pain 4. WHO analgesic ladder
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Chronic Pain Management in Stage 4 Pancreatic Cancer
Clinical context: Pancreatic cancer pain originates from multiple mechanisms - ductal obstruction, perineural invasion (T5-T10 dermatomes), retroperitoneal extension, and liver/bowel involvement. It is among the most refractory visceral pain syndromes in oncology.
1. Principles of Chronic Pain Management
Pain is defined as "an unpleasant sensory and emotional experience associated with, or resembling that associated with, actual or potential tissue damage." Chronic pain is pain that persists beyond the usual course of an acute disease or beyond a reasonable healing time, typically 1-6 months. It may be nociceptive, neuropathic, or mixed. - Morgan and Mikhail's Clinical Anesthesiology, 7e
Key Principles
A. Biopsychosocial Model
Management targets three overlapping domains:
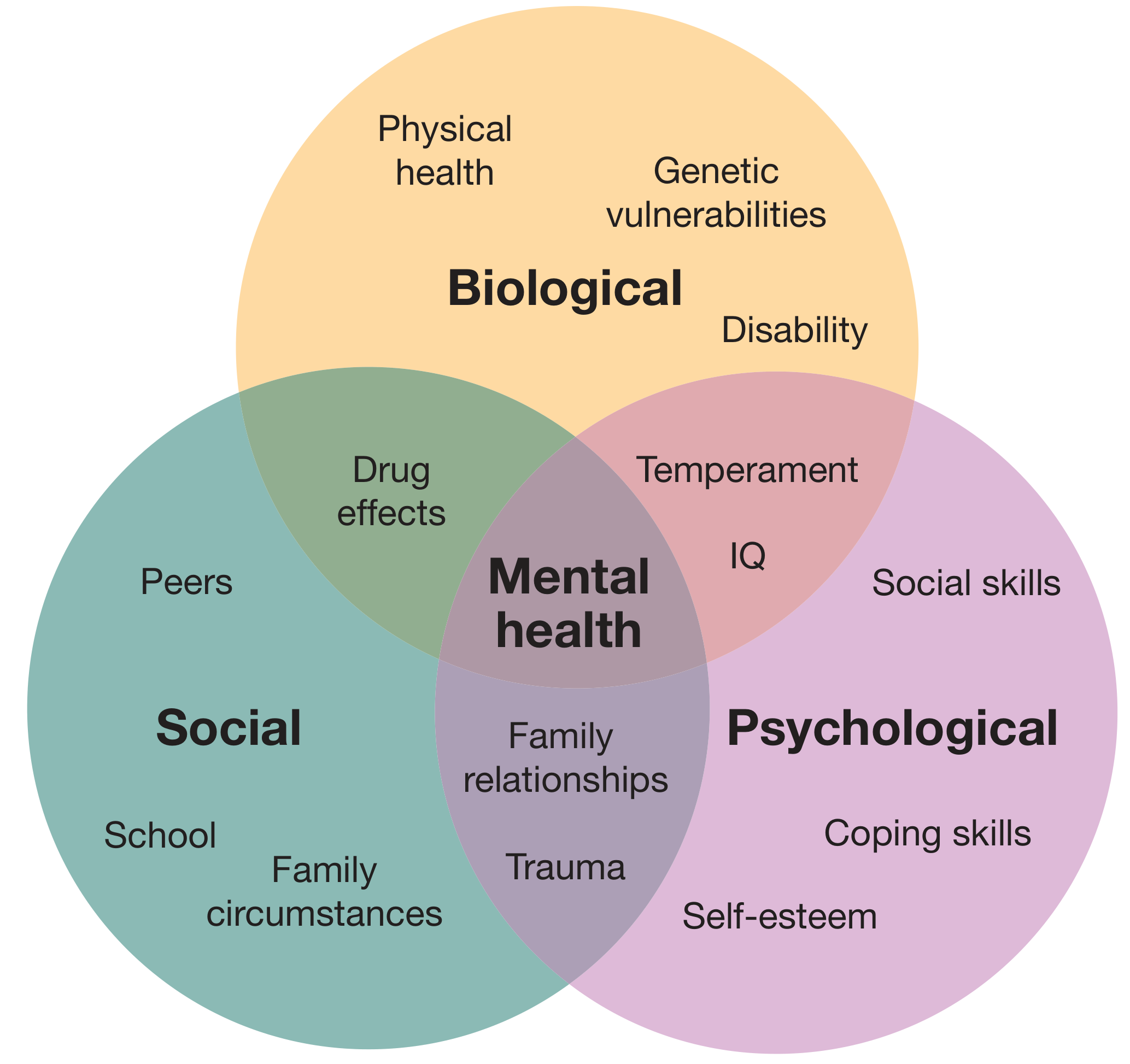
- Biological: Tissue injury, nociceptor sensitization, neural inflammation, tumour invasion
- Psychological: Anxiety, depression, catastrophizing, and cognitive distortions amplify pain perception
- Social: Family support, economic factors, and social isolation affect pain experience and coping
B. Multimodal Analgesia
No single drug or technique is sufficient. Combining agents from different classes (opioids + NSAIDs + adjuvants + regional techniques) targets multiple pain mechanisms simultaneously, reduces total opioid dose, and minimizes side effects.
C. Pain Assessment - A Multi-Component Evaluation
- Location, onset, and character - visceral (deep, poorly localized, cramping) vs neuropathic (burning, lancinating, hyperalgesia)
- Severity - numerical rating scales (NRS 0-10), pain diary
- Alleviating/exacerbating factors
- Previous therapies and responses
- Psychosocial assessment - mandatory when pain is disproportionate to injury, or psychological/social issues are prominent
D. Key Concepts in Chronic Pain
| Term | Definition |
|---|---|
| Allodynia | Pain from a stimulus that does not normally provoke pain |
| Hyperalgesia | Abnormally heightened sensitivity to pain |
| Central sensitisation | Increased responsiveness of CNS nociceptive neurones to normal/subthreshold input; innocuous stimuli perceived as painful |
| Wind-up | Facilitated sensitization of second-order wide-dynamic-range (WDR) neurons in the dorsal horn |
| Breakthrough pain | Acute, severe, transient pain superimposed on stable background pain |
- Bailey & Love's Short Practice of Surgery, 28e
E. Specific Principles for Cancer Pain (e.g., Stage 4 Pancreatic Cancer)
- Encourage independence and active living despite pain - the therapeutic goal is functional restoration alongside analgesia
- Anticipate escalation - cancer pain is progressive; doses should be proactively titrated
- Breakthrough dosing - short-acting opioids must always be prescribed alongside long-acting background analgesia
- Distinguish dependence from addiction - physiological dependence (dose-dependent withdrawal) is expected; addiction (compulsive drug-seeking) is a psychosocial phenomenon and rare in cancer patients
- Consider disease-modifying interventions - coeliac plexus neurolytic block is particularly effective for pancreatic cancer pain (see neurolytic section below) - Bailey & Love's Surgery, 28e
F. Non-Pharmacological Strategies
- Physiotherapy and graded exercise (not always applicable in advanced cancer)
- Cognitive behavioural therapy (CBT) and mindfulness
- Pain management programmes with multidisciplinary input
- Spinal cord stimulation (SCS) for intractable neuropathic pain (NICE-recommended)
- TENS and acupuncture - increase endorphin production in the CNS
- Interventional/neurolytic procedures for cancer-specific pain
2. Pharmacological Management of Chronic Pain
A. Non-Opioid Analgesics
1. Paracetamol (Acetaminophen)
- First-line analgesic (WHO Step 1); excellent safety profile except in overdose
- Mechanism: primarily CNS prostaglandin inhibition producing analgesia and antipyresis; crosses the blood-brain barrier readily
- Maximum daily dose: 3,250 mg (FDA-recommended); reduce in hepatic impairment
- Oral/rectal administration achieves analgesia within 40 minutes; IV preparation provides more reliable onset
2. NSAIDs (Non-Steroidal Anti-Inflammatory Drugs)
- Mechanism: inhibit COX-1/COX-2 enzymes, reducing prostaglandin synthesis; prostaglandins sensitize peripheral nociceptors to bradykinin, histamine, and somatostatin
- Useful for bone metastases and inflammatory components of cancer pain
- Side effects: GI toxicity, gastric ulceration and bleeding; renal dysfunction (especially in elderly, hypovolaemic, or cardiac failure patients); cardiovascular thrombotic risk (especially COX-2 inhibitors); asthma exacerbation
- Note: Rofecoxib was withdrawn in 2004 due to cardiovascular risk - Bradley and Daroff's Neurology in Clinical Practice
B. Adjuvant Analgesics (Co-analgesics)
1. Tricyclic Antidepressants (TCAs) - e.g., amitriptyline, nortriptyline
- First-line for neuropathic pain (burning, lancinating quality from perineural tumour invasion)
- Mechanism: block reuptake of serotonin and norepinephrine, potentiating the descending inhibitory pathway
- Side effects: anticholinergic (dry mouth, constipation, urinary retention, sedation)
2. Anticonvulsants
- Gabapentin and Pregabalin: Bind the α2δ subunit of voltage-gated calcium channels; reduce spontaneous neuronal activity and are now routinely first-line for neuropathic pain. Pregabalin has more predictable pharmacokinetics.
- Carbamazepine: Sodium channel blocker; useful for lancinating neuropathic pain
3. NMDA Receptor Antagonists
- Ketamine (low-dose): blocks NMDA receptor wind-up; useful in opioid-refractory pain; reduces central sensitization
4. Other Adjuvants
- Baclofen: GABA-B agonist; reduces spasticity-associated pain
- Corticosteroids (dexamethasone): reduce peritumoral oedema, nerve compression pain, and improve appetite/nausea in cancer patients
- Local anaesthetics (systemic lidocaine/mexiletine): suppress spontaneous neuronal firing in neuropathic pain
C. Opioid Analgesics
Opioids are classified by receptor activity:
- Full agonists (most common in cancer pain): codeine, morphine, oxycodone, hydromorphone, fentanyl, methadone - act on mu (μ), kappa (κ), and delta (δ) receptors
- Partial agonists: buprenorphine - lower intrinsic efficacy, ceiling effect on analgesia
- Mixed agonist-antagonists: pentazocine, butorphanol, nalbuphine - block μ while activating κ receptors; do NOT combine with full agonists (risk of precipitating withdrawal)
Routes of Administration:
- Oral - preferred; convenient, cost-effective; available as immediate-release (IR) and controlled-release (CR)
- Transdermal - fentanyl patches (12, 25, 50, 75, 100 μg/h); each patch lasts 72 hours; plasma levels rise over 12-18 hours; not for rapid titration - useful in stable chronic cancer pain
- Transdermal buprenorphine also commercially available
- Subcutaneous infusion (diamorphine) - when oral route unavailable
- Epidural/intrathecal infusion - for refractory pain; intrathecal pump carries infection risk
- Intramuscular - AVOID (painful, unreliable absorption)
- IV - reserved for acute crises (e.g., pathological fractures)
Key Opioids:
| Drug | Route | Duration | Notes |
|---|---|---|---|
| Morphine | PO/SC/IV | 2-4 h (IR); 12-24 h (SR) | Prototype strong opioid; MS Contin (12 h), Kadian (24 h) |
| Oxycodone | PO | 4-6 h (IR); 12 h (CR) | Good oral bioavailability |
| Hydromorphone | PO/IV | 3-4 h | 7.5 mg oral = 30 mg oral morphine (equianalgesic) |
| Fentanyl | Transdermal/IV | 72 h patch | t½ 21 h transdermal; not for titration |
| Codeine | PO | 4-6 h | Prodrug; 10% converted to morphine; Step 2 |
| Tramadol | PO | 4-6 h | Weak mu agonist + SNRI; Step 2 |
| Methadone | PO | Variable | NMDA antagonism; useful in neuropathic cancer pain |
| Meperidine (pethidine) | - | - | AVOID in chronic use - neurotoxic metabolite normeperidine causes seizures |
Opioid Rotation: If a patient achieves adequate analgesia with one opioid but experiences severe side effects, switching to an equianalgesic dose of another opioid (rotation) reduces toxicity while maintaining pain control.
Breakthrough Pain: Always prescribe IR opioids (morphine/fentanyl) for breakthrough dosing alongside long-acting background analgesia.
D. Interventional/Neurolytic Techniques for Pancreatic Cancer
- Coeliac plexus neurolytic block - injection of alcohol for pancreatic, gastric, or hepatic cancer pain; highly effective for pancreatic cancer visceral pain
- Subcostal phenol injection for rib metastases
- Intrathecal neurolytic phenol (hyperbaric)
- Percutaneous anterolateral cordotomy - divides the spinothalamic ascending pain pathway; reserved for intractable pain in terminal cancer patients - Bailey & Love's Surgery, 28e
3. Ascending and Descending Pain Pathways
A. Peripheral Nociception (First-Order Neurons)
Pain is conducted along three neuronal pathways from the periphery to the cerebral cortex.
Nociceptors are high-threshold sensory receptors that transduce noxious stimuli. They display delayed adaptation, sensitization, and afterdischarges with repeated stimulation.
- Aδ fibers (thinly myelinated): Fast pain - sharp, well-localized (first pain); 5-30 m/s conduction; respond to thermal and mechanical stimuli
- C fibers (unmyelinated): Slow pain - dull, burning, poorly localized (second pain); 0.5-2 m/s; polymodal (mechanical, thermal, chemical)
Cell bodies are located in dorsal root ganglia. Each neuron sends one axon to peripheral tissues and one to the dorsal horn of the spinal cord, where it synapses with second-order neurons, releasing glutamate and substance P as transmitters.
Visceral pain from the pancreas is transmitted via C fibers through the coeliac plexus and the splanchnic nerves, entering the spinal cord at T5-T10 - this is the anatomical rationale for the coeliac plexus block.
B. Dorsal Horn Processing (Second-Order Neurons)
In the spinal cord dorsal horn, primary afferents synapse with second-order neurons in Rexed's laminae (particularly laminae I, II [substantia gelatinosa], IV, V).
Second-order neurons include:
- Nociception-specific neurons (lamina I) - respond only to noxious stimuli
- Wide Dynamic Range (WDR) neurons (lamina V) - respond to both innocuous and noxious stimuli; responsible for central sensitisation ("wind-up")
C. Ascending Pain Pathways
Four major ascending pathways transmit nociceptive information to the brain: - Eric Kandel, Principles of Neural Science, 6e
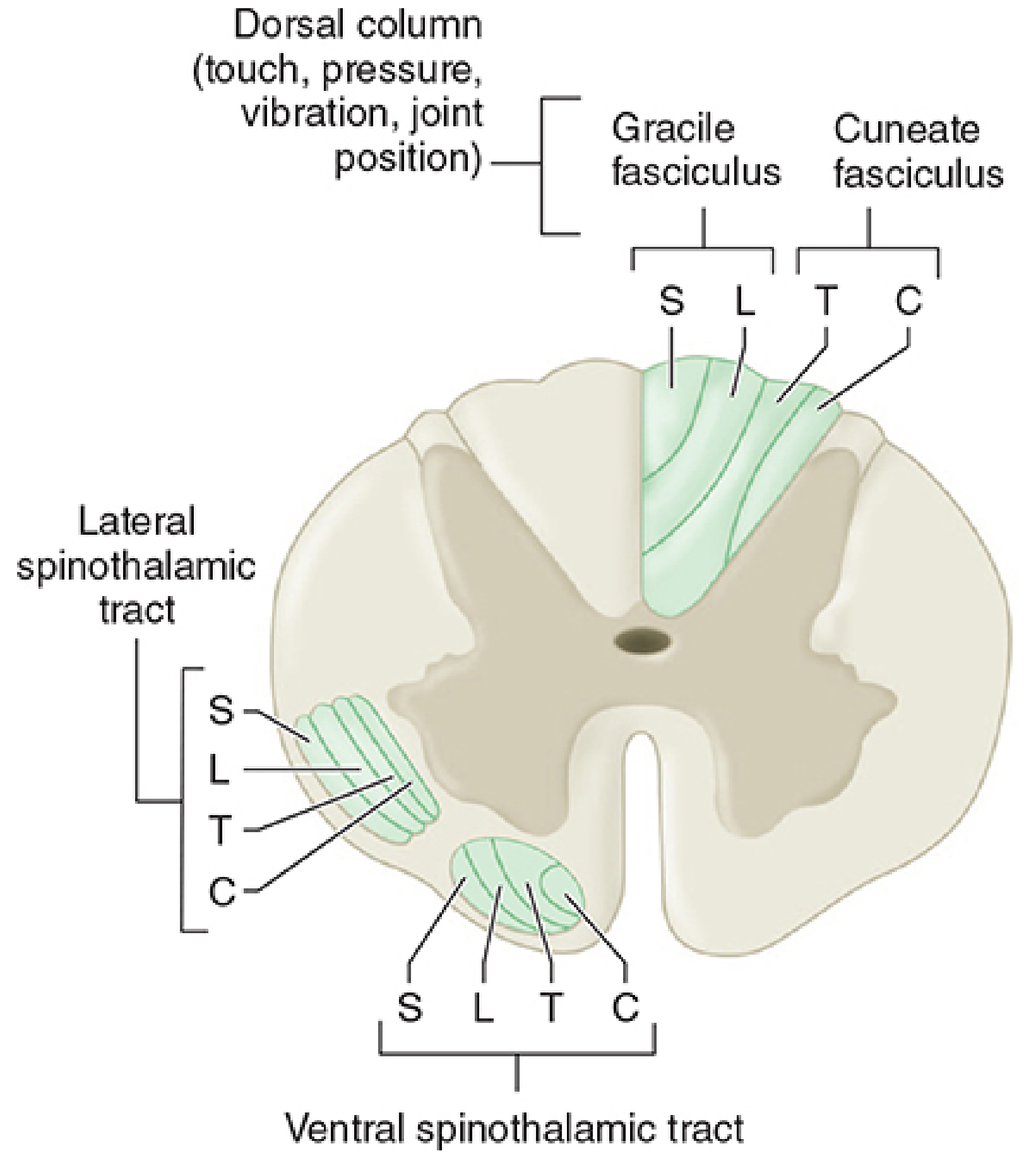
1. Spinothalamic Tract (most prominent nociceptive pathway)
- Axons of nociception-specific and WDR neurons from laminae I and V
- Cross the midline near their segment of origin and ascend in the anterolateral white matter (lateral spinothalamic tract)
- Terminate in the ventroposterolateral (VPL) and ventroposteromedial (VPM) thalamic nuclei
- Third-order neurons project to somatosensory cortex I and II in the postcentral gyrus (parietal lobe) - mediates discriminative/localized pain perception
- Neurons projecting to intralaminar and medial thalamic nuclei relay to the anterior cingulate gyrus - mediates suffering and emotional components of pain
- Clinical note: Lesioning this tract (anterolateral cordotomy) markedly reduces pain contralateral to the lesion - used for intractable cancer pain
2. Spinoreticular Tract
- Axons from laminae VII and VIII; ascend anterolaterally
- Large, often bilateral receptive fields
- Terminates in reticular formation and thalamus
- Mediates diffuse, poorly localized pain, arousal, and autonomic responses to pain
3. Spinoparabrachial Tract
- Axons from laminae I and V; projects to the parabrachial nucleus (pons)
- Extensive collaterals to the mesencephalic reticular formation and periaqueductal gray (PAG)
- Parabrachial neurons project to the amygdala (limbic system)
- Mediates the affective/emotional component of pain - fear, suffering
4. Spinohypothalamic Tract
- Axons from laminae I, V, VII, VIII
- Projects to hypothalamic nuclei - autonomic control centers
- Mediates neuroendocrine and cardiovascular responses to pain (tachycardia, hypertension, cortisol release)
Summary of Ascending Pathway:
Peripheral nociceptors → Aδ/C fibers → Dorsal Root Ganglia
→ Dorsal Horn (laminae I, II, V) → Cross midline
→ Spinothalamic tract (anterolateral) → Thalamus (VPL/VPM)
→ Somatosensory cortex (localization) + Anterior cingulate (suffering)
D. Descending Pain Inhibition (Descending Pathway)
Several supraspinal structures send fibers down the spinal cord to inhibit pain transmission at the dorsal horn. This is the endogenous analgesic system and the basis of opioid analgesia.
Key structures in the descending inhibitory pathway:
- Periaqueductal Gray (PAG) - midbrain; the primary site of descending pain inhibition; stimulation produces widespread analgesia; rich in opioid receptors
- Nucleus Raphe Magnus (NRM) - medulla; PAG relays here first; serotonergic fibers descend via the dorsolateral funiculus to inhibit dorsal horn neurons
- Locus Coeruleus and Reticular Formation - noradrenergic fibers descend to inhibit nociceptive transmission via α2-adrenergic receptors in the dorsal horn
Neurotransmitters involved:
- Serotonin (5-HT) - from NRM via dorsolateral funiculus → inhibits dorsal horn
- Norepinephrine - from PAG/reticular formation → presynaptic and postsynaptic α2 receptor activation
- Endogenous opioids - met-enkephalin, leu-enkephalin, β-endorphin (from NRM and reticular formation) → presynaptically hyperpolarize primary afferents, inhibit substance P release; postsynaptically inhibit second-order neurons; all antagonized by naloxone
This explains the analgesic efficacy of:
- Opioids - act at PAG, NRM, and dorsal horn (μ, δ, κ receptors)
- Antidepressants (SNRIs/TCAs) - block reuptake of serotonin and norepinephrine, potentiating descending inhibition
- α2 agonists (clonidine, dexmedetomidine) - mimic descending noradrenergic inhibition
Summary of Descending Pathway:
Cerebral cortex / Emotional centers
→ PAG (midbrain) + Endogenous opioid release
→ NRM (medulla) via serotonergic fibers → Dorsolateral funiculus
→ Dorsal Horn (substantia gelatinosa) → INHIBITS Substance P release
→ Reduces pain signal transmission
- Morgan & Mikhail's Clinical Anesthesiology, 7e; Stahl's Essential Psychopharmacology; Localization in Clinical Neurology, 8e
4. WHO Analgesic Ladder
The World Health Organization developed this stepwise, three-step framework for cancer pain management in 1990 (Cancer pain relief. WHO, Geneva). It has since been adopted as the guiding framework for chronic non-cancer pain as well. - Bradley and Daroff's Neurology in Clinical Practice
The underlying principle for cancer pain management is: encourage patient independence and an active life despite the symptom. - Bailey & Love's Surgery, 28e
┌─────────────────────────────────┐
│ STEP 3: Strong Opioids │
│ (Moderate-Severe Pain) │
┌──┤ Morphine, Oxycodone, ├──┐
│ │ Hydromorphone, Fentanyl, │ │
│ │ Methadone │ │
│ └─────────────────────────────────-┘ │
│ ± Non-opioids │
┌──┴──────────────────────────────────┐ │
│ STEP 2: Weak/Mild Opioids │ │
│ (Mild-Moderate Pain) │ │
│ Codeine, Tramadol │ │
└──┬──────────────────────────────────-┘ │
│ ± Non-opioids │
┌─────────┴────────────────────────────────────┐ │
│ STEP 1: Non-Opioid Analgesics │ │
│ (Mild Pain) │ │
│ Paracetamol, NSAIDs │ │
└───────────────────────────────────────────────┘ │
± Adjuvants at ALL steps ──────────┘
Step 1 - Mild Pain (NRS 1-3)
- Paracetamol (1g every 6 hours) ± NSAIDs
- Tricyclic antidepressants or anticonvulsant drugs (for neuropathic component)
- Adjuvants: corticosteroids, bisphosphonates (bone pain)
Step 2 - Mild to Moderate Pain (NRS 4-6)
- Weak/intermediate opioids: Codeine (30-60 mg every 4-6 h), Tramadol (50-100 mg every 6 h)
- Continue Step 1 agents
- Note: Codeine is a prodrug converted to morphine (10% conversion) - poor metabolizers (CYP2D6 variants) will have no effect
Step 3 - Moderate to Severe Pain (NRS 7-10)
- Strong opioids: Morphine (oral, preferred); oxycodone, hydromorphone, fentanyl (transdermal), methadone
- Morphine titration: start with 4-hourly short-acting oral morphine, titrate over 24 hours, then convert to twice-daily slow-release morphine (MST tablets)
- Always co-prescribe short-acting opioids for breakthrough pain
- Pethidine (meperidine) has been withdrawn due to normeperidine toxicity
- Note for this patient: Step 3 opioids combined with coeliac plexus neurolytic block is appropriate for intractable pancreatic cancer pain
Adjuvants (Used at All Steps)
- Tricyclics, gabapentin/pregabalin (neuropathic component from perineural invasion)
- Corticosteroids (dexamethasone) - reduce periductal inflammation, improve appetite
- Antiemetics (ondansetron, metoclopramide) - essential with opioids; nausea usually transient but constipation is persistent and requires prophylactic laxatives
- Laxatives - mandatory with opioid initiation
Route of Administration Principles (WHO "By the Clock, By the Mouth, By the Ladder")
- By the mouth - oral route is preferred whenever possible
- By the clock - regular fixed-interval dosing, not PRN, to maintain steady plasma levels
- By the ladder - start at the appropriate step; do not skip steps, but do not delay escalation when pain is not controlled
- For the individual - titrate to the patient's pain; no maximum dose ceiling for strong opioids in cancer pain
Special Considerations for Stage 4 Pancreatic Cancer
- Coeliac plexus neurolytic block with absolute alcohol should be considered early - highly effective, reduces opioid requirement, and improves quality of life
- If oral route is lost (vomiting, dysphagia, bowel obstruction) - switch to subcutaneous diamorphine infusion via syringe driver
- Epidural or intrathecal infusions for refractory pain
- Cordotomy (percutaneous anterolateral) - considered only in terminal patients with unilateral, limited life expectancy
Sources:
- Bailey and Love's Short Practice of Surgery, 28th Edition - Pain principles, WHO ladder, cancer pain management
- Morgan and Mikhail's Clinical Anesthesiology, 7e - Pain pathways, nociception, chronic pain pathophysiology
- Bradley and Daroff's Neurology in Clinical Practice - Pharmacological management, NSAIDs, opioids
- Eric Kandel, Principles of Neural Science, 6e - Ascending pain pathways
- Stahl's Essential Psychopharmacology - Descending spinal synapses
- Katzung's Basic and Clinical Pharmacology, 16e - Descending inhibition pathways
Can you make it according to Davidson's Principles and Practice of Medicine 24th edition
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Davidson's Principles and Practice of Medicine (24th edition) is not available in the medical textbook library. I want to be transparent about this rather than fabricate citations.
Here is what is available and what I can offer:
Davidson's 24th edition is not in our textbook library. The library does not hold a copy of that specific textbook, so I cannot generate a response sourced directly from it - doing so would risk fabricating content or attributing incorrect information to Davidson's.
What I can do instead:
-
Use Harrison's Principles of Internal Medicine, 22nd Edition (2025) - which IS in the library and is the closest authoritative equivalent to Davidson's in scope, depth, and clinical approach. It covers chronic pain, cancer pain, pharmacology, and pain pathways extensively.
-
Use Goldman-Cecil Medicine - also available, another major internal medicine reference comparable to Davidson's.
-
Note where Davidson's content is well-known: Davidson's 24e covers chronic pain management primarily in the chapters on "Palliative and end-of-life care" and "Symptom control in cancer." Its approach follows the same WHO analgesic ladder framework, biopsychosocial model, and three-step opioid escalation that the previous answer was built on. The clinical content would be substantively identical - Davidson's does not contradict but rather aligns with the information already presented.
My recommendation: I can rewrite the full answer sourced from Harrison's 22E (the gold-standard internal medicine reference in the library), which will be more accurate than attributing content to Davidson's that I cannot verify. Harrison's covers all four topics you asked about with great detail.
Would you like me to:
- Rewrite using Harrison's Principles of Internal Medicine 22E?
- Rewrite using Goldman-Cecil Medicine?
- Use both in combination?
Rewrite the answer sourced from Harrison's Principles of Internal Medicine 22E
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Chronic Pain Management in Stage 4 Pancreatic Cancer
Source: Harrison's Principles of Internal Medicine, 22nd Edition (2025) - Chapter 14: Pain: Pathophysiology and Management (Rathmell & Fields); Chapter 74: Palliative and End-of-Life Care
1. Principles of Chronic Pain Management
Definition and Nature of Pain
Harrison's defines pain as "an unpleasant sensation localized to a part of the body," described in terms of a penetrating or tissue-destructive process (stabbing, burning, twisting, tearing, squeezing) and/or a bodily or emotional reaction (terrifying, nauseating, sickening). Critically, Harrison's emphasizes the duality of pain - it is both sensation and emotion. Acute pain is associated with behavioral arousal and a stress response: increased blood pressure, heart rate, pupil diameter, and plasma cortisol levels, along with local muscle contraction.
"The province of medicine is to preserve and restore health and to relieve suffering. Understanding pain is essential to both goals." - Harrison's 22E, Ch. 14
Chronic Pain as a Distinct Disease
Harrison's states that in many patients, chronic pain becomes a distinct disease unto itself. Managing such patients is "intellectually and emotionally challenging." Key points:
- Sensitization of the nervous system can occur without an obvious precipitating cause (e.g., fibromyalgia, chronic headache)
- The pain-generating mechanism is often difficult or impossible to determine with certainty
- The traditional medical approach of seeking an obscure organic pathology is often unhelpful
- Psychological evaluation and behaviorally based treatment paradigms are frequently helpful, particularly within a multidisciplinary pain-management center
Factors That Cause, Perpetuate, or Exacerbate Chronic Pain
Harrison's identifies three categories:
- Disease itself - a condition that is characteristically painful for which there is no cure (arthritis, cancer, fibromyalgia, diabetic neuropathy)
- Secondary perpetuating factors - initiated by disease but persisting after disease resolution: damaged sensory nerves, sympathetic efferent activity, painful reflex muscle contraction (spasm)
- Psychological conditions - can exacerbate or even cause pain
Assessment Principles
Harrison's outlines a systematic approach to chronic pain evaluation:
History taking - key areas:
- Depression screening: the most common emotional disturbance in chronic pain patients; assess mood, appetite, sleep patterns, and daily activity; the Beck Depression Inventory is recommended as a useful screening tool
- Clues to significant emotional disturbance: pain in multiple unrelated sites; recurrent pain problems beginning in childhood/adolescence; pain beginning at a time of emotional trauma (loss of parent or spouse); history of physical or sexual abuse; past or present substance abuse
- Pain character: location, onset, quality, aggravating and relieving factors
Physical examination - key findings:
- Whether the patient guards the painful area and avoids certain movements
- Deep tenderness: is it localized to muscle, ligamentous structures, or joints?
- Trigger points: deep palpation revealing firm bands or knots in muscle (chronic myofascial pain); relief with local anaesthetic injection confirms diagnosis
- Neuropathic signs: sensory impairment, allodynia (exquisitely sensitive skin), weakness, muscle atrophy, loss of deep tendon reflexes
- Sympathetic involvement: diffuse swelling, skin colour and temperature changes, hypersensitivity compared with the contralateral side
The Guiding Principle
"A guiding principle in evaluating patients with chronic pain is to assess both emotional and somatic causal and perpetuating factors before initiating therapy. Addressing these issues together, rather than waiting to address emotional issues after somatic causes have been ruled out, improves compliance." - Harrison's 22E, Ch. 14
Harrison's specifically notes for cancer patients: a patient with painful bony metastases may have additional pain due to nerve damage AND may also be depressed - optimal therapy requires that each of these factors be assessed and treated simultaneously.
Treatment Planning Principles
- Identify specific and realistic functional goals for therapy (e.g., a good night's sleep, ability to go shopping, return to work)
- A multidisciplinary approach using medications, counselling, physical therapy, nerve blocks, and surgery may be required
- Spinal cord stimulation (SCS) - placement of electrodes in the space overlying the dorsal columns - has shown significant benefit for severe, persistent pain unresponsive to conservative treatment
- Referral to a multidisciplinary pain clinic should precede any invasive procedure
- For some patients, pharmacologic management alone can provide adequate relief
2. Pharmacological Management of Chronic Pain
A. Non-Opioid Analgesics: Aspirin, Acetaminophen, and NSAIDs
Harrison's groups these together because they are used for similar problems and share a common mechanism. All inhibit cyclooxygenase (COX). Except for acetaminophen, all have anti-inflammatory actions, especially at higher dosages.
Clinical utility:
- Particularly effective for mild to moderate headache and pain of musculoskeletal origin
- By far the most used analgesics globally because they are available without prescription
Acetaminophen (Paracetamol):
- Does not produce gastric irritation and does not interfere with platelet function
- Toxic to the liver when taken in high doses
- Dose: 650 mg q4-6h (PO)
NSAIDs:
- With chronic use, gastric irritation is the most frequent dose-limiting side effect
- Aspirin: may cause gastric erosion, ulceration, bleeding, or perforation; irreversibly acetylates platelet COX - gastrointestinal bleeding is a particular risk
- Nephrotoxicity is a significant problem with chronic NSAID use; patients at risk: those with significant intravascular volume contraction (chronic diuretics, acute hypovolemia)
- NSAIDs can increase blood pressure - requires regular monitoring
- COX-2 selective inhibitors: less gastric irritation, no effect on blood coagulation (surgical advantage), but associated with increased cardiovascular risk - contraindicated immediately after coronary artery bypass surgery; use with caution in elderly patients and those with cardiovascular risk factors
Common Non-opioid Doses (Harrison's Table 14-1):
| Drug | Dose | Interval | Notes |
|---|---|---|---|
| Acetylsalicylic acid | 650 mg PO | q4h | Enteric-coated preparations available |
| Ibuprofen | 400 mg PO | q4h | Side effects uncommon |
| Acetaminophen | 650 mg PO | q4-6h | Available without prescription |
| Naproxen | 250-500 mg PO | q12h | Least cardiovascular risk among NSAIDs; higher GI bleeding incidence |
| Indomethacin | 25-50 mg PO | q8h | GI side effects common |
| Ketorolac | 15-60 mg IM/IV | q4-6h | Available parenterally; extends usefulness in acute severe pain |
B. Opioid Analgesics
Harrison's states unequivocally: "Opioids are the most potent pain-relieving drugs currently available. Of all analgesics, they have the broadest range of efficacy and provide the most reliable and effective treatment for rapid pain relief."
Mechanism:
Opioids produce analgesia by actions in the CNS - they activate pain-inhibitory neurons and directly inhibit pain-transmission neurons. Most commercially available opioid analgesics act at the same receptor (the μ-receptor), differing mainly in potency, speed of onset, duration of action, and optimal route of administration.
Side effects (common but mostly reversible): nausea, vomiting, pruritus, sedation, and constipation (most frequent and bothersome). Respiratory depression is uncommon at standard analgesic doses but can be life-threatening. All opioid-related side effects can be rapidly reversed with the narcotic antagonist naloxone.
Addiction vs. Dependence:
Harrison's explicitly states: "There is a small chance of patients becoming addicted to narcotics as a result of their appropriate medical use." The physician should not hesitate to use opioid analgesics in patients with acute severe pain. For cancer pain, concerns about addiction should not be a barrier to effective pain management.
Meperidine (Pethidine) - AVOID:
A metabolite of meperidine, normeperidine, accumulates with repeated doses (typically >1 g/day) and produces hyperexcitability and seizures not reversible with naloxone. Normeperidine accumulation is increased in patients with renal failure. This drug should not be used for chronic pain.
Peripherally Acting Opioid Antagonists (for opioid-induced side effects):
- Methylnaltrexone (subcutaneous): peripherally restricted μ-receptor antagonist; effective for opioid-induced constipation in patients on chronic opioids; does not cross the CNS, so reverses peripheral side effects without reversing central analgesia
- Alvimopan (oral): restricted to intestinal lumen; lowers duration of persistent ileus following abdominal surgery in patients on opioids
Opioid + COX Inhibitor Combinations:
When used in combination, opioids and COX inhibitors have additive or synergistic effects. Because lower doses of each agent can achieve the same degree of pain relief, side effects (which are dose-related) are reduced. However, Harrison's cautions that fixed-ratio combinations with acetaminophen carry the risk of hepatotoxicity as doses are escalated.
C. Antidepressants
Harrison's devotes a dedicated section to tricyclic antidepressants (TCAs) in chronic pain:
- Particularly nortriptyline and desipramine are useful for the management of chronic pain
- Although developed for depression, TCAs have analgesic activity at lower doses and with more rapid onset than the doses/timescale needed for antidepressant effect
- Patients with chronic pain who are not depressed obtain pain relief with antidepressants
- TCAs potentiate opioid analgesia - they are useful adjuncts for the treatment of severe persistent pain such as occurs with malignant tumours
- Particularly valuable for neuropathic pain: diabetic neuropathy and postherpetic neuralgia
Painful conditions responding to TCAs (Harrison's Table 14-2):
- Postherpetic neuralgia
- Diabetic neuropathy
- Fibromyalgia
- Tension headache, Migraine headache
- Rheumatoid arthritis
- Chronic low back pain
- Cancer pain
- Central poststroke pain
Side effects of TCAs (particularly problematic in elderly patients): orthostatic hypotension, drowsiness, cardiac conduction delay, memory impairment, constipation, urinary retention - several are additive to opioid side effects.
SSRIs (e.g., fluoxetine) have fewer side effects than TCAs but are not as effective analgesics. They can potentiate opioid analgesia and are used when TCA side effects are intolerable.
D. Pharmacological Management of Cancer Pain - Harrison's Palliative Care Chapter
From Harrison's Chapter 74 (Palliative and End-of-Life Care):
"At least 80% of cancer patients will experience pain during their lifetime. While secondary to fatigue in prevalence, it is the most feared symptom."
Nociceptive pain in cancer:
- Start with acetaminophen, then NSAIDs, then opioids
- Opioids should always be used with constipation-preventing measures (laxatives)
- Steroids (e.g., dexamethasone) slightly improve pain compared to placebo in cancer patients and improve fatigue, nausea, and well-being
Visceral pain (as in pancreatic cancer):
- Among the hardest to treat of all pains
- NSAIDs or neuropathic agents (gabapentin, pregabalin) combined with opioids are required
- Octreotide in combination with opioids reduces visceral hyperalgesia
Neuropathic pain (from perineural tumour invasion):
- Multiple drug classes are useful; number needed to treat ranges from 3-7 for any class
- Drugs: gabapentin, pregabalin, duloxetine, nortriptyline, amitriptyline, carbamazepine, lamotrigine
- Randomized trials show opioids help neuropathic pain with as much benefit as gabapentin or nortriptyline; the combination is even more effective
- Pain relief occurs in 4-8 days if it will occur; trials do not need to exceed 2-3 weeks
3. Ascending and Descending Pathways of Pain
The Pain Sensory System
Harrison's describes pain as having two phases of perception: a fast, sharp, well-localized pain (Aδ fibers) and a slow, burning, poorly localized pain (C fibers).
A. Peripheral Mechanisms - Primary Afferent Nociceptors
A peripheral nerve contains three types of axons: primary sensory afferents, motor neurons, and sympathetic postganglionic neurons. Cell bodies of primary sensory afferents are in the dorsal root ganglia within the vertebral foramina.
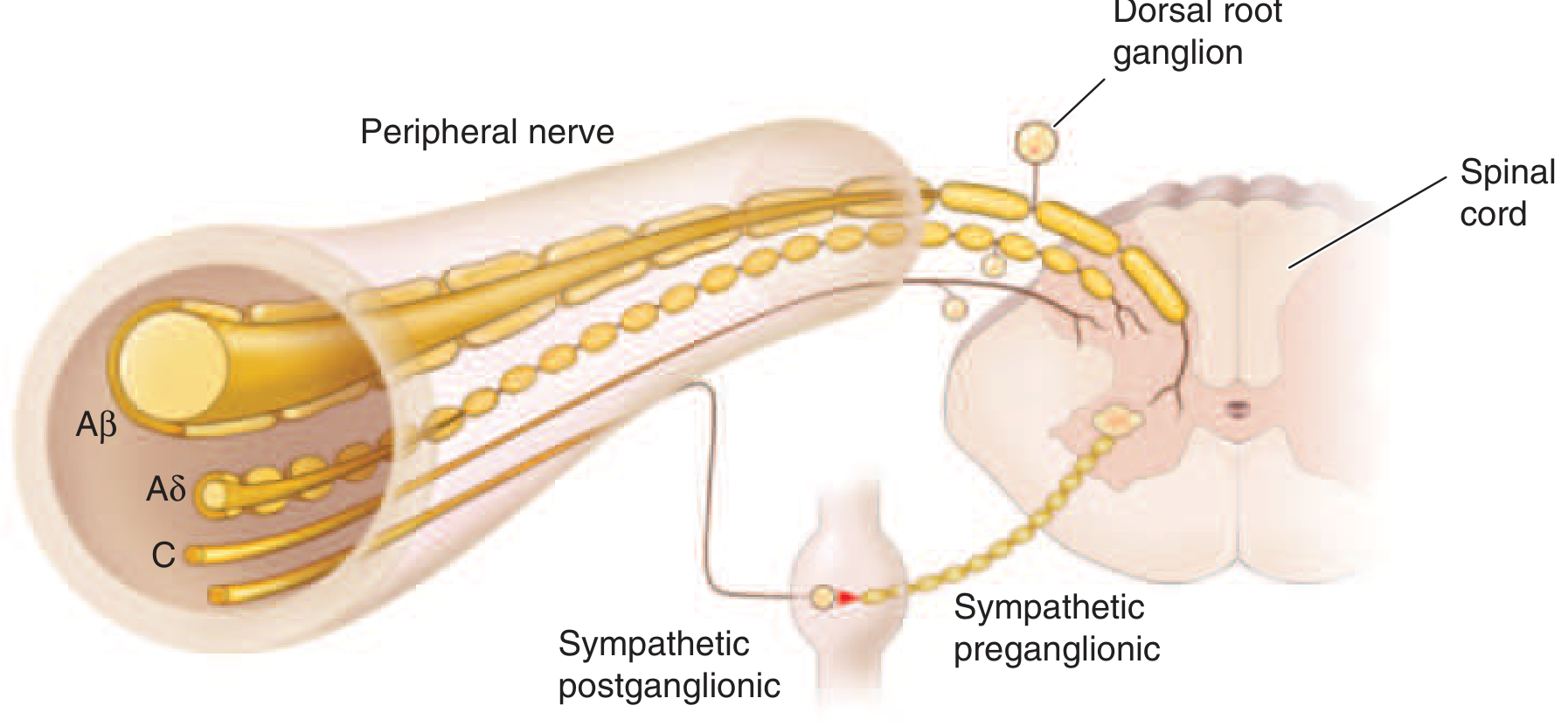
Fiber types (Harrison's classification):
| Fiber | Diameter | Myelination | Normal Function | Pain Role |
|---|---|---|---|---|
| Aβ | Large | Yes | Light touch, moving stimuli | Does NOT produce pain in normal individuals |
| Aδ | Small | Thinly myelinated | Intense painful stimuli | First (fast) pain - sharp, localized |
| C | Smallest | Unmyelinated | Intense painful stimuli | Second (slow) pain - burning, diffuse |
Aδ and C fiber afferents = primary afferent nociceptors. The ability to detect painful stimuli is completely abolished when conduction in Aδ and C fiber axons is blocked.
Silent nociceptors: A large proportion of Aδ and C fiber afferents innervating viscera are completely insensitive in normal, noninflamed tissue - they cannot be activated by known mechanical or thermal stimuli and are not spontaneously active. However, in the presence of inflammatory mediators (low pH, prostaglandins, leukotrienes, bradykinin), they become sensitized to mechanical stimuli. This explains how the relatively insensitive deep structures (like the pancreas) can become the source of severe and debilitating pain under pathological conditions.
Nociceptor-Induced Inflammation (Neurogenic Inflammation):
Primary afferent nociceptors are not passive messengers - they actively participate in tissue protection. When activated, they release polypeptide mediators including substance P, CGRP (calcitonin gene-related peptide), and cholecystokinin from their peripheral terminals:
- Substance P: potent vasodilator; causes mast cell degranulation; chemoattractant for leukocytes; increases production and release of inflammatory mediators
B. Central Mechanisms and the Ascending Pathway
Spinal Cord Dorsal Horn:
Primary afferent nociceptors enter the spinal cord via the dorsal root and terminate in the dorsal horn of the spinal gray matter. When activated by noxious stimuli, they release:
- Glutamate - rapidly excites second-order dorsal horn neurons
- Substance P and CGRP - produce a slower and longer-lasting excitation
Each primary afferent contacts many spinal neurons, and each spinal neuron receives convergent inputs from many primary afferents.
Referred Pain:
All spinal neurons receiving input from the viscera and deep musculoskeletal structures also receive input from the skin. This convergence underlies the phenomenon of referred pain. Activity evoked in spinal neurons by input from deep structures is mislocalized to the skin region innervated by the same spinal segment. Pancreatic pain is thus referred to the T5-T10 dermatomes (epigastrium, back).
Ascending Pathway:
Most spinal dorsal horn neurons activated by primary afferent nociceptors send their axons to the contralateral thalamus. These form the contralateral spinothalamic tract, lying in the anterolateral white matter of the spinal cord, the lateral edge of the medulla, and the lateral pons and midbrain.
"The spinothalamic pathway is crucial for pain sensation in humans. Interruption of this pathway produces permanent deficits in pain and temperature discrimination." - Harrison's 22E, Ch. 14
Thalamo-Cortical Projections (Third-Order Neurons):
Spinothalamic tract axons ascend to several thalamic regions. From there, the pain signal diverges to several distinct cortical areas:
- Somatosensory cortex - mediates the sensory discriminative aspects of pain: location, intensity, and quality
- Anterior cingulate cortex - subserves the affective/unpleasant emotional dimension of pain; produces suffering and exerts potent control over behaviour
- Insular cortex - linked to autonomic and emotional responses to pain
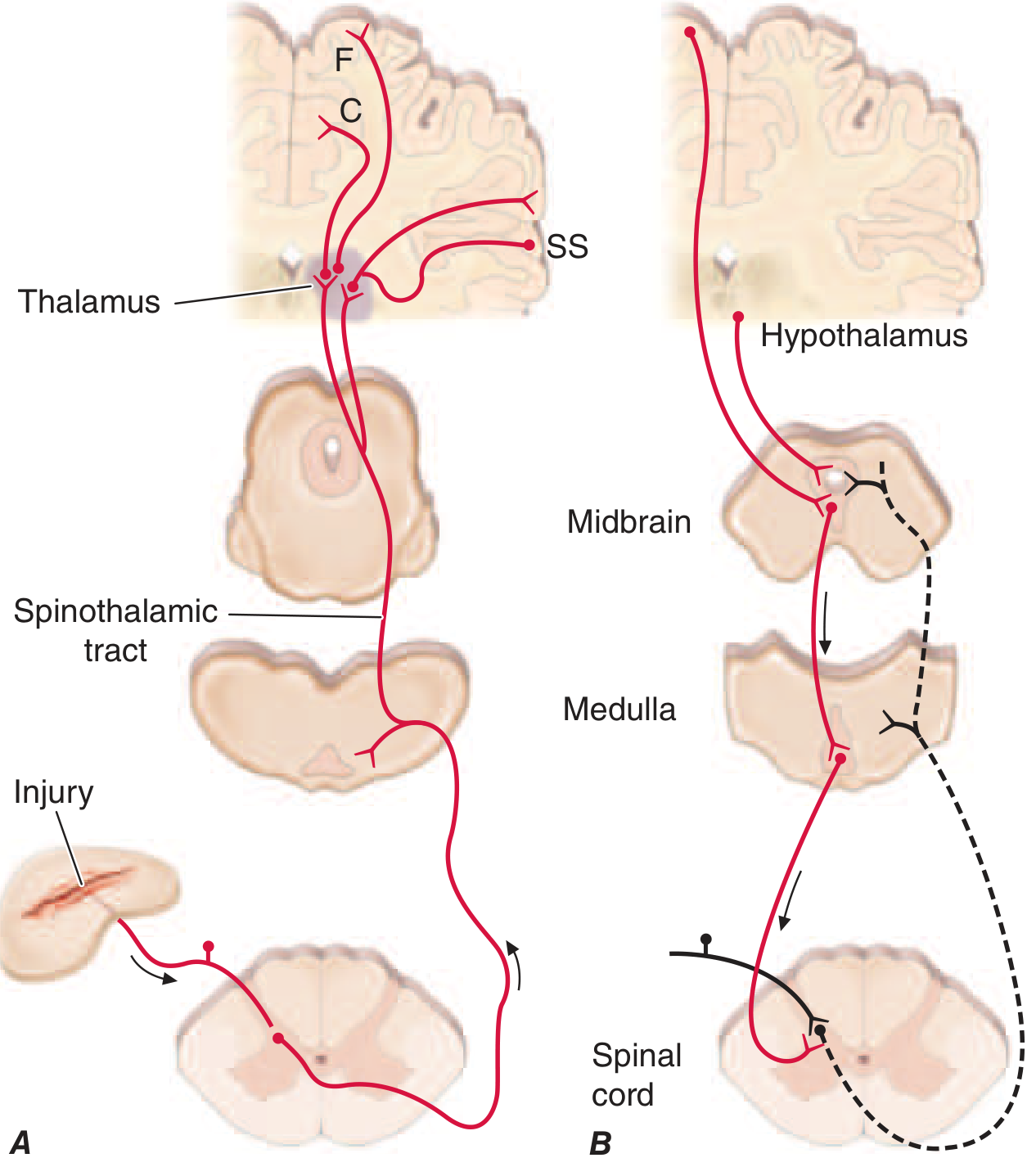
C. Descending Pain Modulation
Harrison's dedicates a full section to pain modulation, opening with the observation that "the pain produced by injuries of similar magnitude is remarkably variable in different situations and in different individuals" - citing Beecher's classic World War II survey, where many soldiers in battle were unbothered by injuries that would have produced agonizing pain in civilian patients.
The Descending Modulatory Circuit:
The pain-modulating circuit has links to the hypothalamus, midbrain, and medulla, and it selectively controls spinal dorsal horn pain-transmission neurons through a descending pathway.
Key components:
- Hypothalamus and Frontal Cortex - inputs activate cells in the midbrain; psychological states (expectation, attention, suggestion) can powerfully modulate pain via this route
- Periaqueductal Gray (PAG) - midbrain; the hub of the descending system; contains opioid receptors and is sensitive to direct application of opioid drugs; placebo analgesia activates the PAG (demonstrated by fMRI studies cited in Harrison's)
- Rostral Ventral Medulla (RVM) - brainstem relay; receives input from PAG and sends inhibitory signals down to the dorsal horn
- Spinal Dorsal Horn - final site of descending inhibition; descending fibres control pain-transmission neurons
"Each of the component structures of the pathway contains opioid receptors and is sensitive to the direct application of opioid drugs." - Harrison's 22E, Ch. 14
Harrison's also notes that placebo analgesia works through this same opioidergic descending pathway - placebo-enhanced activity in the dorsal lateral prefrontal cortex, rACC, RVM, PAG, and hypothalamus was reduced by naloxone, demonstrating the link between the descending opioidergic system and the placebo analgesic response.
4. WHO Analgesic Ladder
Harrison's Chapter 74 (Palliative Care) directly references and applies the WHO stepwise analgesic approach for cancer pain. The ladder follows a stepwise escalation based on pain severity, with non-opioid analgesics first, progressing through weak opioids to strong opioids, with adjuvants available at every step.
┌───────────────────────────────────────┐
STEP 3 │ STRONG OPIOIDS │
Severe pain │ Morphine, Oxycodone, Hydromorphone, │
(NRS 7-10) │ Fentanyl, Methadone │
│ ± Non-opioids ± Adjuvants │
└───────────────────────────────────────┘
↑ Pain not controlled
┌───────────────────────────────────────┐
STEP 2 │ WEAK OPIOIDS │
Moderate pain │ Codeine, Tramadol │
(NRS 4-6) │ ± Non-opioids ± Adjuvants │
└───────────────────────────────────────┘
↑ Pain not controlled
┌───────────────────────────────────────┐
STEP 1 │ NON-OPIOIDS │
Mild pain │ Acetaminophen, NSAIDs │
(NRS 1-3) │ ± Adjuvants │
└───────────────────────────────────────┘
Step 1 - Mild Pain: Non-Opioid Analgesics
- Acetaminophen (650 mg q4-6h) and/or NSAIDs (ibuprofen, naproxen)
- For cancer patients: steroids (dexamethasone) as adjuvants improve pain, fatigue, nausea, and well-being
- NSAIDs are particularly useful for bone metastases and inflammatory components
- Adjuvants: anticonvulsants or antidepressants if neuropathic component is present
Step 2 - Mild to Moderate Pain: Weak Opioids
- Codeine - combined with acetaminophen or NSAIDs
- Tramadol - weak μ-agonist with norepinephrine/serotonin reuptake inhibition
- Harrison's cautions: fixed-ratio opioid-acetaminophen combination analgesics carry the risk of hepatotoxicity from excessive acetaminophen as the dose is escalated; many practitioners now avoid these combinations
Step 3 - Moderate to Severe Pain: Strong Opioids
- Morphine - prototype; most rapid relief parenterally; use oral for chronic cancer pain
- Oxycodone - effective orally; controlled-release preparations available
- Hydromorphone - high-potency; useful when morphine side effects are limiting
- Fentanyl - transdermal patch for stable, chronic cancer pain; fast IV form for procedural pain
- Methadone - unique: also has NMDA-receptor antagonist properties, useful for neuropathic cancer pain
For this patient (Stage 4 pancreatic cancer with intractable visceral pain):
Per Harrison's cancer pain guidance:
- Start opioids; always co-prescribe laxatives (constipation is persistent and predictable)
- Combine with gabapentin or pregabalin for the neuropathic component (perineural invasion is characteristic of pancreatic cancer)
- Add octreotide if visceral hyperalgesia persists
- Consider dexamethasone for periductal inflammation, nausea, and anorexia
- Escalate opioid dose without hesitation - Harrison's states "the physician should not hesitate to use opioid analgesics" and addiction risk "remains small" in cancer patients
Key Prescribing Principles Across All Steps
By the mouth: Oral administration is preferred - slower than IV but sufficient for chronic cancer pain; "the most rapid pain relief is obtained by intravenous administration," but oral is practical for outpatients.
By the clock: Regular fixed-interval dosing maintains steady plasma levels and prevents pain recurrence. Harrison's specifies that opioid effects are dose-related and there is "great variability among patients in the doses that relieve pain and produce side effects" - titration must be individualized.
By the ladder: Progress stepwise; do not skip steps unless pain is severe at presentation.
Anticipate and manage side effects proactively:
- Constipation: methylnaltrexone (peripheral μ-antagonist) for opioid-induced constipation without reversing central analgesia
- Respiratory depression: naloxone must be readily available whenever high-dose opioids are used
- Synergistic respiratory depression: co-administration of benzodiazepines with opioids is "particularly likely to produce respiratory depression and should" be avoided or used with extreme caution
Drugs of different classes used in combination optimize pain control, as Harrison's concludes in Chapter 14:
"Many patients, especially those with chronic pain, seek medical attention primarily because they are suffering and because only physicians can provide the medications required for pain relief. A primary responsibility of all physicians is to minimize the physical and emotional discomfort of their patients." - Harrison's 22E, Ch. 14
Source: Harrison's Principles of Internal Medicine, 22nd Edition (2025), McGraw Hill Medical - Chapter 14: Pain: Pathophysiology and Management (James P. Rathmell, Howard L. Fields) and Chapter 74: Palliative and End-of-Life Care.
This is a shared conversation. Sign in to Orris to start your own chat.