Hey i will start to read cvs in medicine so do the basics should be clear for me to learn it easily
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have rich material from Costanzo Physiology and Guyton & Hall to build a comprehensive "CVS basics" guide. Let me compile this into a clear, well-structured teaching guide.
Here is your complete CVS Basics Foundation guide - everything you need to know before diving into clinical cardiovascular medicine.
Cardiovascular System (CVS) - The Complete Basics
1. Overview of the CVS
The cardiovascular system has one job: deliver oxygen and nutrients to tissues and remove waste products. It consists of:
- The heart - the pump
- Blood vessels - arteries, veins, capillaries
- Blood - the transport medium
The circulation has two loops:
- Pulmonary circulation: Right heart → lungs → Left heart (picks up O₂, drops CO₂)
- Systemic circulation: Left heart → body → Right heart (delivers O₂, picks up CO₂)
2. Heart Anatomy - The 4-Chamber Setup
| Chamber | Role | Wall thickness |
|---|---|---|
| Right atrium (RA) | Receives deoxygenated blood from SVC/IVC | Thin |
| Right ventricle (RV) | Pumps to lungs via pulmonary artery | Moderate |
| Left atrium (LA) | Receives oxygenated blood from pulmonary veins | Thin |
| Left ventricle (LV) | Pumps to entire body via aorta | Thickest |
The LV is the thickest because it must generate the highest pressure (systemic circulation). By the Law of Laplace: wall tension = pressure × radius / (2 × wall thickness). In hypertension, the LV hypertrophies as a compensatory response - but this can eventually lead to failure.
The 4 valves:
- Tricuspid (RA → RV) - 3 leaflets
- Pulmonary (RV → pulmonary artery)
- Mitral (LA → LV) - 2 leaflets (bicuspid)
- Aortic (LV → aorta)
Atrioventricular (AV) valves = Mitral + Tricuspid (open during diastole, filling)
Semilunar valves = Pulmonary + Aortic (open during systole, ejection)
3. The Conduction System
This is the electrical wiring of the heart. The sequence must be memorized:
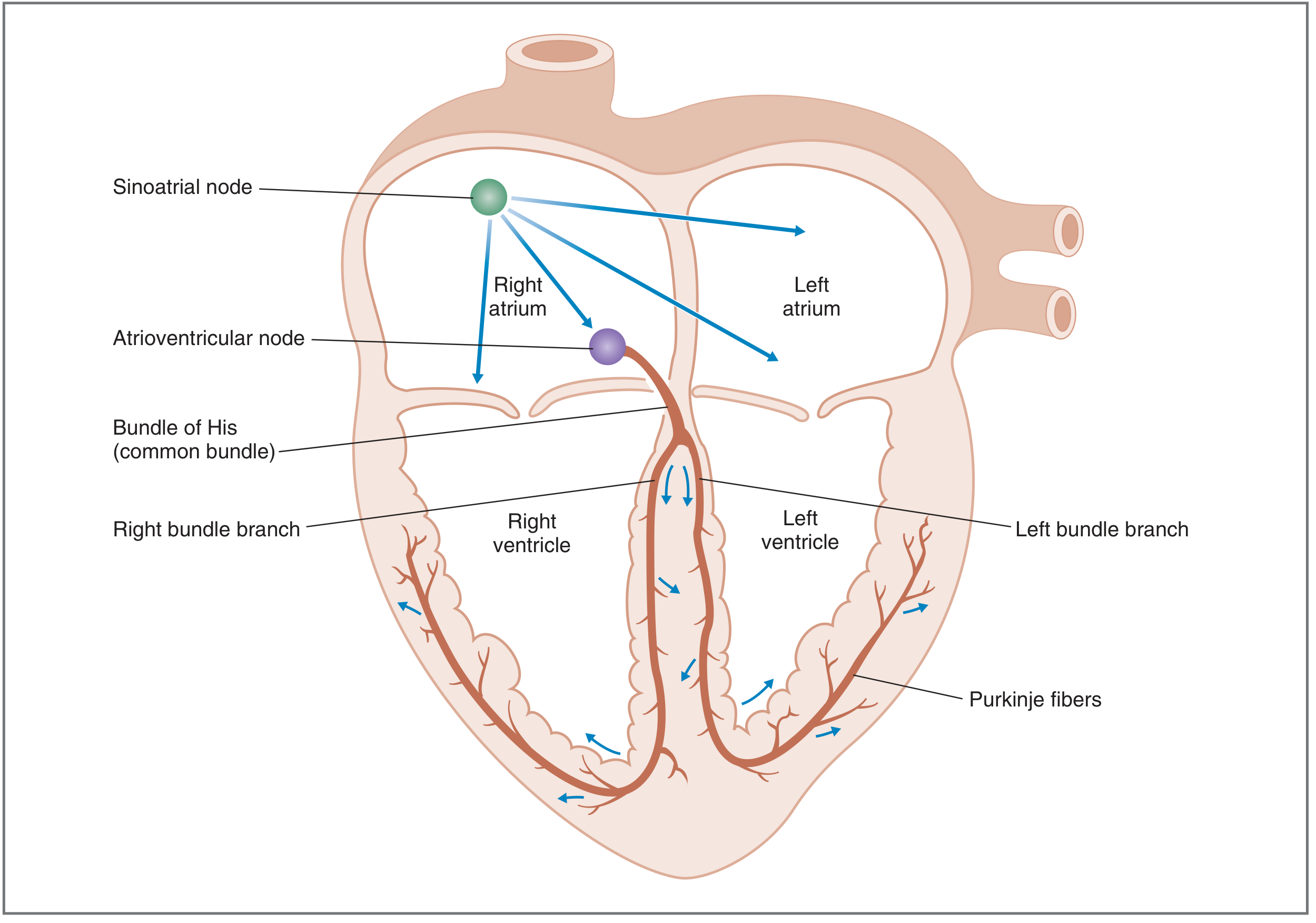
SA Node → Atria → AV Node → Bundle of His → Left & Right Bundle Branches → Purkinje Fibers → Ventricular muscle
| Structure | Location | Function |
|---|---|---|
| SA node | Superior lateral wall of right atrium (near SVC) | Primary pacemaker - fires 60-100/min |
| AV node | Junction of atria and ventricles | Delays impulse >0.1 sec - lets atria contract first |
| Bundle of His | Common bundle after AV node | Conducts to ventricles |
| Bundle branches | Left and right divisions | Distribute to each ventricle |
| Purkinje fibers | Ventricular walls | Fastest conduction - coordinates ventricular contraction |
Why the AV delay matters: It lets the atria contract first, acting as "primer pumps" to top up the ventricles before the ventricles contract. This contributes ~20-30% of ventricular filling.
Normal sinus rhythm requires all 3 criteria:
- Impulse originates in SA node
- Rate 60-100/min, regular
- Activation sequence is correct
4. Cardiac Action Potentials
There are two types - know them both.
Ventricular/Atrial/Purkinje Fiber Action Potential (Fast Response)
Resting membrane potential: -85 mV
| Phase | Name | Ion movement |
|---|---|---|
| Phase 0 | Rapid upstroke | Fast Na⁺ channels open → Na⁺ rushes IN (depolarization) |
| Phase 1 | Initial repolarization | Na⁺ channels close, brief K⁺ out |
| Phase 2 | Plateau | Ca²⁺ in (L-type channels) balances K⁺ out - unique to cardiac muscle |
| Phase 3 | Rapid repolarization | Ca²⁺ channels close, K⁺ out surges |
| Phase 4 | Resting membrane potential | Stable at -85 mV (mostly K⁺ conductance) |
The plateau (Phase 2) is what makes cardiac muscle special. It:
- Prolongs the action potential (~200-300 ms vs 1-2 ms in nerve)
- Triggers calcium-induced calcium release from the SR
- Creates the prolonged absolute refractory period - prevents tetany (the heart cannot be forced into sustained contraction)
SA Node Action Potential (Slow Response / Pacemaker)
Resting membrane potential: -60 mV (unstable - this is the key!)
| Phase | Event | Ion movement |
|---|---|---|
| Phase 4 | Pacemaker potential (slow spontaneous depolarization) | "Funny current" (If) - Na⁺/K⁺ in; decreasing K⁺ out |
| Phase 0 | Upstroke (slow, not steep) | L-type Ca²⁺ channels (NOT fast Na⁺ channels) |
| Phase 3 | Repolarization | K⁺ out |
The SA node has no stable resting potential - it automatically drifts toward threshold. This is automaticity. No nerve input needed for it to fire.
5. The Cardiac Cycle - 7 Phases
One complete heartbeat. Study this carefully - it underlies all of CVS clinical medicine.
| Phase | What happens | ECG event | Valves | Heart sound |
|---|---|---|---|---|
| A - Atrial systole | Atria contract, final ventricular filling | P wave | Mitral open | S4 (abnormal) |
| B - Isovolumetric ventricular contraction | Ventricles contract but no ejection yet, all valves closed, pressure rises sharply | QRS | Mitral closes | S1 |
| C - Rapid ventricular ejection | Aortic valve opens, blood ejected fast, ventricular pressure peaks | ST segment | Aortic opens | - |
| D - Reduced ventricular ejection | Slower ejection, ventricular volume reaches minimum | T wave | - | - |
| E - Isovolumetric ventricular relaxation | Ventricles relax, all valves closed, pressure falls | - | Aortic closes | S2 |
| F - Rapid ventricular filling | Mitral opens, blood flows passively from LA to LV | - | Mitral opens | S3 (may be normal in young) |
| G - Reduced ventricular filling | Slow passive filling continues | - | - | - |
Key rule for valves: Valves open/close based on pressure gradients, not directly from electrical signals.
- Mitral closes when LV pressure > LA pressure (start of systole)
- Aortic opens when LV pressure > aortic pressure
- Aortic closes when aortic pressure > LV pressure (start of diastole)
- Mitral opens when LA pressure > LV pressure
6. Heart Sounds
| Sound | Cause | Clinical note |
|---|---|---|
| S1 (lub) | Mitral + tricuspid valves closing | Normal; louder in tachycardia |
| S2 (dub) | Aortic + pulmonary valves closing | Normal; splits on inspiration |
| S3 | Rapid ventricular filling (F phase) | Normal in young/athletes; pathological over 40 → heart failure |
| S4 | Atrial contraction against stiff ventricle | Always pathological → LV hypertrophy, ischemia |
7. Key Cardiac Output Concepts
Cardiac Output (CO) = Stroke Volume (SV) × Heart Rate (HR)
Normal CO = ~5 L/min at rest
Stroke Volume is determined by three things:
- Preload - how much blood is in the ventricle before contraction (ventricular end-diastolic volume). More stretch → more force (Frank-Starling law)
- Afterload - the resistance the ventricle must pump against (aortic pressure in LV, pulmonary pressure in RV). More afterload → less SV
- Contractility (inotropy) - inherent force of contraction regardless of length. Increased by sympathetic stimulation, digoxin; decreased by heart failure, beta-blockers
Fick Principle for measuring CO:
CO = O₂ consumption ÷ (arterial O₂ content - venous O₂ content)
Example: if O₂ consumption = 250 mL/min, arterial O₂ = 0.20 mL/mL, venous O₂ = 0.15 mL/mL:
CO = 250 ÷ (0.20 - 0.15) = 250 ÷ 0.05 = 5,000 mL/min = 5 L/min
8. Autonomic Control of the Heart
| System | Effect on HR | Effect on Contractility | Receptor |
|---|---|---|---|
| Sympathetic (noradrenaline/adrenaline) | Increases (positive chronotropy) | Increases (positive inotropy) | β1-adrenergic |
| Parasympathetic (acetylcholine) | Decreases (negative chronotropy) | Minimal effect on ventricles | Muscarinic (M2) |
Sympathetic speeds up the SA node pacemaker potential (phase 4 rises faster). Parasympathetic slows it down (hyperpolarizes the SA node, makes phase 4 slope flatter).
9. The ECG - What Each Wave Means
| Wave/Interval | Represents |
|---|---|
| P wave | Atrial depolarization |
| PR interval | Conduction through AV node (normal: 0.12-0.20 sec) |
| QRS complex | Ventricular depolarization (normal: <0.12 sec) |
| ST segment | Ventricular plateau (all cells depolarized together) |
| T wave | Ventricular repolarization |
| QT interval | Total ventricular electrical activity |
Note: Atrial repolarization is hidden inside the QRS complex (too small to see).
10. Blood Pressure Basics
Blood Pressure = Cardiac Output × Total Peripheral Resistance (TPR)
- Systolic BP - peak pressure during ventricular ejection
- Diastolic BP - minimum pressure during ventricular relaxation
- Pulse pressure = Systolic - Diastolic (reflects stroke volume and aortic compliance)
- Mean arterial pressure (MAP) = Diastolic + (1/3 × pulse pressure)
Normal adult BP: <120/80 mmHg
Arterioles are the main site of resistance in the circulation. They control TPR and therefore blood pressure and local blood flow distribution.
Reading Order Recommendation
If you want to read CVS systematically:
- Start with Guyton & Hall (Chapter 9 onwards) for the big picture - it is the most readable
- Use Costanzo Physiology for action potentials and the cardiac cycle table above - it is very exam-focused
- Braunwald's Heart Disease is the clinical reference - come to it after the physiology is solid
Sources: Costanzo Physiology 7th Edition, Guyton and Hall Textbook of Medical Physiology, Braunwald's Heart Disease
This is a shared conversation. Sign in to Orris to start your own chat.