Give me cream on corn
Here's a classic Creamed Corn recipe:
Creamed Corn
Serves: 4 | Time: 15-20 minutes
Ingredients
- 4 cups fresh or frozen corn kernels (about 5-6 ears if fresh)
- 2 tbsp unsalted butter
- 1/2 cup heavy cream
- 1/4 cup whole milk
- 1 tbsp sugar (optional, enhances sweetness)
- 1/2 tsp salt
- 1/4 tsp black pepper
- 1 tbsp cornstarch + 2 tbsp cold water (slurry, for thickening)
- Optional: pinch of cayenne or smoked paprika
Instructions
- If using fresh corn - cut kernels off the cob, then scrape the cob with the back of your knife to release the milky juice. That juice adds a lot of flavor.
- Melt butter in a skillet or saucepan over medium heat.
- Add corn and cook for 3-4 minutes, stirring occasionally.
- Pour in the cream and milk. Stir to combine.
- Add sugar, salt, and pepper. Let it simmer for 5 minutes.
- Mix cornstarch with cold water to make a slurry, then stir it into the corn. Cook another 2-3 minutes until thickened to your liking.
- Taste and adjust seasoning. Serve hot.
Tips
- Richer flavor: Swap half the cream for cream cheese (2 oz), melted in.
- Cheesy version: Stir in 1/4 cup shredded parmesan or cheddar at the end.
- Herb finish: Fresh thyme, chives, or basil work great on top.
- Spicy kick: A small diced jalapeño sauteed with the butter takes it up a notch.
It's a simple, comforting side that pairs well with grilled chicken, BBQ, pork chops, or fried fish. Enjoy!
Give me cream to treat plantar corn
Reading File
Finding Sources
Searching the Web
plantar corn treatment salicylic acid cream topical options
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Good - I now have solid textbook coverage. Here's the full clinical answer:
Creams and Topical Treatments for Plantar Corns
A plantar corn (clavus) is a circumscribed, conical thickening of skin with its apex pointing inward, pressing on underlying nerves and causing a dull, boring, or sharp/lancinating pain. Treatment focuses on relieving pressure, removing the hyperkeratotic tissue, and, when needed, correcting underlying bony abnormalities.
First-Line Topical Treatment: Salicylic Acid
Salicylic acid is the mainstay topical agent. It works as a keratolytic - it causes epidermal cells to swell, soften, and desquamate, effectively dissolving the protein making up the corn.
| Form | Concentration | How to Use |
|---|---|---|
| Plaster / medicated pad | 40% (most effective) | Apply after careful paring of the corn; soak foot for 30 min before reapplying; remove after 48 hrs, rub off white macerated skin, reapply - repeat until corn resolves |
| Gel / liquid | 12-17% (OTC) | Apply daily to the corn only; cover with bandage |
| Cream | 6-12% (OTC) | Apply daily; less occlusive than plaster, slower acting |
How to apply (protocol):
- Soak the foot in warm water for 10-15 minutes to soften skin.
- Gently pare/shave the surface keratin with a pumice stone or scalpel (remove the central core if possible).
- Apply the salicylic acid preparation only to the corn - avoid surrounding normal skin.
- Cover with a bandage or plaster.
- Repeat every 48 hours until resolved.
- Andrews' Diseases of the Skin, Clinical Dermatology
- Goodman & Gilman's Pharmacological Basis of Therapeutics
Other Topical / Supportive Options
| Agent | Role |
|---|---|
| 12% Ammonium lactate lotion | Softens thickened skin; useful adjunct |
| Urea-containing cream (10-40%) | Keratolytic and moisturizing; helps soften the corn between treatments |
| Emollient / moisturizing cream | General skin softening; not curative alone |
Important Precautions
- Diabetes / peripheral neuropathy / poor circulation: High-concentration salicylic acid (especially 40%) is contraindicated - it can damage healthy surrounding skin and cause ulceration. These patients should be managed by a podiatrist or dermatologist using mechanical debridement only.
- Salicylic acid should never be applied to broken, infected, or inflamed skin.
- Corns with an underlying bony spur or exostosis will recur unless the bony abnormality is addressed - topical treatment provides only temporary relief in these cases.
When Creams Are Not Enough
If topical treatment fails, options escalate to:
-
Podiatric debridement (paring with a No. 15 blade)
-
Silicone/collagen injections over the bony prominence
-
Orthotics and corrective footwear (wide toe box, cushioned soles)
-
Surgical resection of the underlying bony prominence
-
Campbell's Operative Orthopaedics 15th Ed 2026
-
Tintinalli's Emergency Medicine
Bottom line: For a straightforward plantar corn, start with an OTC salicylic acid plaster (40%) or gel/cream (12-17%) combined with regular soaking and gentle paring. If you have diabetes, poor circulation, or the corn keeps coming back, see a podiatrist rather than self-treating.
How do I know if it's a corn vs. a plantar wart?
Finding Sources
Searching the Web
plantar wart vs corn differential diagnosis clinical features
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Here is a full clinical comparison, grounded in dermatology and orthopaedics textbooks:
Corn vs. Plantar Wart: How to Tell the Difference
These two conditions are frequently confused because both appear as thickened, painful lesions on the sole of the foot. They have completely different causes and require different treatments, so distinguishing them matters.
The #1 Bedside Test: Direction of Pain
| Test | Corn | Plantar Wart |
|---|---|---|
| Press straight down (perpendicular) | Painful | Less painful |
| Squeeze from the sides (lateral pressure) | Less painful | Painful |
This single maneuver is the most useful clinical differentiator. - Andrews' Diseases of the Skin
What You See After Paring the Surface
Gently shave or pare the top layer of skin - this is the most definitive visual test:
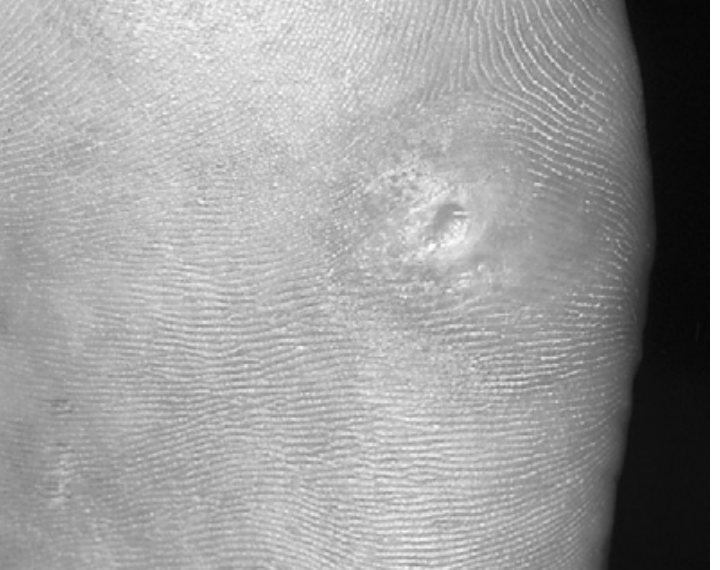
Corn after paring:
- Reveals a smooth, clear, translucent horny core (the nucleus)
- No bleeding or black dots
- Skin lines (dermatoglyphics) are preserved and pass through the lesion normally
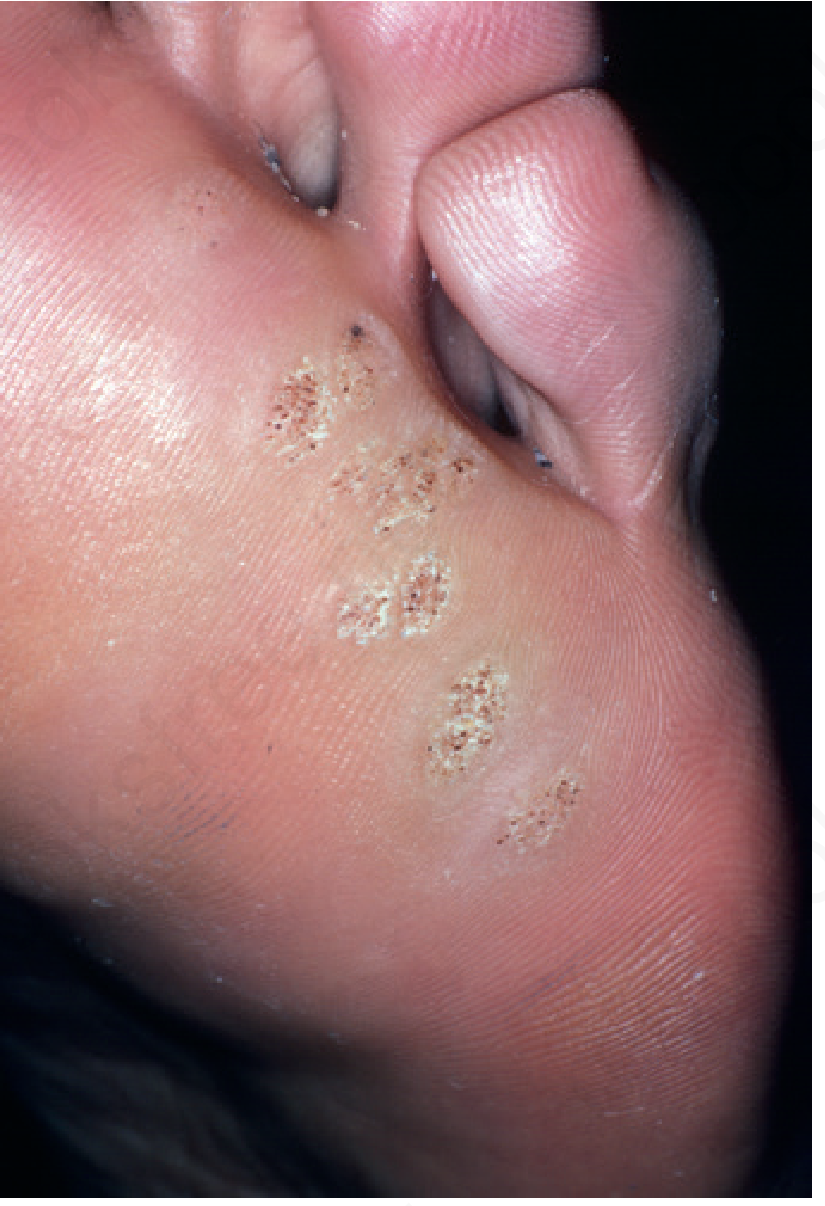
Plantar wart after paring:
- Reveals elongated dermal papillae with blood vessels
- Classic "black dots" (thrombosed capillaries) - these are tiny dark spots visible on the surface or after paring
- Skin lines are interrupted and do not pass through the lesion - a key sign
- May bleed as "pinpoint bleeders" after shaving
Full Comparison Table
| Feature | Corn (Clavus) | Plantar Wart (Verruca Plantaris) |
|---|---|---|
| Cause | Mechanical pressure / friction | HPV infection (virus) |
| Number | Usually single lesion at pressure point | Can be single or multiple; can cluster ("mosaic wart") |
| Location | Over bony prominences, under metatarsal heads | Anywhere on sole, including non-pressure areas |
| Appearance | Smooth, shiny surface; well-defined | Rough, cauliflower-like surface |
| Skin lines | Intact, pass through lesion | Interrupted - a hallmark sign |
| Black dots | Absent | Present (thrombosed capillaries) |
| After paring | Clear, smooth horny core | Elongated papillae, pinpoint bleeding |
| Pain pattern | Direct downward pressure | Lateral (side-to-side) squeezing |
| Borders | Well-defined, cone-shaped | Less well-defined, can have satellite lesions |
| Contagious? | No | Yes (HPV - spreads in shared showers, pools) |
| Spontaneous resolution | Yes, if pressure removed | Sometimes (especially in children), but often persists |
Other Conditions to Keep in Mind
A couple of imposters can mimic both:
- Porokeratosis plantaris discreta: sharply marginated, cone-shaped, rubbery lesion under metatarsal heads - frequently confused with both warts and corns. Has a 3:1 female predominance.
- Callus: diffuse thickening without a central core - broader and flatter than a corn.
- Histology: if genuinely uncertain, a biopsy can definitively distinguish a wart (HPV-driven epidermal changes) from a corn (pure hyperkeratosis). Biopsy also rules out rare mimics like epithelioid sarcoma.
Bottom Line
The two fastest checks you can do yourself:
- Squeeze the sides - if that hurts more than pressing straight down, it's more likely a wart.
- Look for black dots - their presence strongly favors a wart.
If you're not sure, or if you have diabetes or poor circulation, see a podiatrist or dermatologist rather than treating blindly - the treatments differ significantly.
OTC plaster didn’t work
Finding Sources
Searching the Web
plantar corn OTC salicylic acid failed next treatment options podiatrist
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Good - I have everything I need. Here's the full step-up plan:
When OTC Plasters Don't Work: What to Do Next
OTC salicylic acid plasters (typically 12-17%) often fail for a few reasons: the corn is too deep, there's an underlying bony prominence driving it, the plaster wasn't applied correctly, or treatment wasn't continued long enough. Here's what comes next, in order of escalation.
Step 1 - Check Why It Failed First
Before escalating, ask:
- Did you pare the corn first before each application? Salicylic acid can't penetrate a thick keratin cap - the surface must be shaved down before applying.
- Did you soak for 30 minutes beforehand? This softens skin and doubles absorption.
- Did you protect surrounding skin? If not, irritation may have stopped you too early.
- Is it actually a wart? Warts need a completely different treatment pathway (cryotherapy, etc.).
Step 2 - Professional Scalpel Debridement (Podiatrist)
This is the most effective non-surgical next step. A podiatrist or dermatologist uses a No. 10 or No. 15 scalpel blade held parallel to the lesion to gradually shave and pare back the corn layer by layer. Because hyperkeratotic skin has no nerve supply, this is usually tolerable without local anesthetic.
- Produces immediate relief by physically removing the mass pressing on underlying nerves
- Can be combined with higher-concentration agents post-debridement
- Should be followed by aperture pads (donut-shaped cushions placed around the corn site) to keep pressure off the area
Pfenninger & Fowler's Procedures for Primary Care
Step 3 - Higher-Concentration Topicals (After Professional Paring)
| Agent | Concentration | Notes |
|---|---|---|
| Salicylic acid plaster | 40% (prescription-strength) | Applied after careful professional paring; repeat every 48h |
| Urea cream | 20-40% | Keratolytic + moisturizing; helps soften between sessions |
| Ammonium lactate lotion | 12% | Useful adjunct to soften thick lesions |
| Trichloroacetic acid (TCA) | Applied in-office | Caustic; used by dermatologists on resistant lesions |
Step 4 - Address the Root Cause (Crucial for Preventing Recurrence)
A corn will always come back unless the mechanical cause is corrected. Debridement alone is only a temporary fix. Options:
- Orthotics (custom or semi-rigid) - redistribute pressure away from the affected area; semi-rigid shown to be more effective than soft
- Corrective footwear - wide toe box, thick cushioned soles, rocker-bottom soles
- Aperture/metatarsal pads (e.g. moleskin, silicone pads like Silipos) - take direct pressure off the corn site
- Wider or properly fitted shoes - many corns are caused simply by footwear that is too narrow or too short
Step 5 - When a Bony Prominence Is the Cause
If imaging reveals an underlying exostosis or bony spur, topical treatment will never produce a lasting cure. Surgery becomes appropriate:
- Condylectomy - shaving the prominent metatarsal condyle
- Metatarsal osteotomy - elevating a depressed metatarsal head
- Resection arthroplasty - for hard corns over the toe joints (e.g. proximal IP joint)
- Hallux valgus correction - if the corn is secondary to bunion deformity, over 90% of patients see improvement of lesser metatarsal callosities after correcting the primary deformity
Campbell's Operative Orthopaedics 15th Ed 2026; Pfenninger & Fowler's Procedures for Primary Care
Step 6 - Specialist Referral Criteria
See a podiatrist or dermatologist promptly if:
- OTC treatment has failed after 4-6 weeks of diligent use
- You have diabetes, peripheral neuropathy, or poor circulation (self-treatment risks ulceration)
- The lesion is growing, bleeding, or changing appearance
- You have significant pain affecting your gait
- Secondary infection develops (redness, warmth, swelling, discharge)
Complications of Untreated Corns
Leaving a resistant corn alone carries real risks: secondary infection, bursitis, and - in diabetics with neuropathy - serious ulceration. Don't delay a podiatry visit if simple measures have been exhausted.
Are plantar warts harmful
Finding Sources
Searching the Web
plantar warts dangerous harmful complications HPV
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
I now have rich textbook content. Here's a thorough answer:
Are Plantar Warts Harmful?
For most healthy people: no, not seriously. Plantar warts are caused by low-risk HPV strains (types 1, 2, 27, and 57) - these are completely different from the high-risk HPV types (16, 18) that cause cervical and other cancers. They are benign skin lesions. That said, they can cause real problems worth knowing about.
What They Actually Are
Plantar warts are HPV infections of the skin. The virus enters through tiny breaks in the skin - typically from walking barefoot on contaminated surfaces (public showers, pools, locker rooms). HPV infection is extremely common; most people will experience it at some point in their lifetime. - Andrews' Diseases of the Skin
Reasons They Can Become a Problem
1. Pain and Gait Disruption
Because they sit on weight-bearing areas of the sole, plantar warts are pressed flat by walking and can cause significant pain with every step. Over time this can subtly alter your gait, which puts abnormal stress on the ankles, knees, and hips.
2. Spreading
- On your own foot: The virus sheds from the wart and can infect nearby skin, forming clusters or "mosaic warts" (multiple contiguous warts that fuse into one large lesion). Mosaic warts are harder to treat than single warts.
- To other people: HPV is contagious via direct contact or contaminated surfaces. Walking barefoot in shared spaces spreads it.
3. They Don't Always Go Away
Many plantar warts in healthy adults persist and spread if left untreated. Unlike flat warts (which have the highest rate of spontaneous remission), plantar warts - especially the deep myrmecia type caused by HPV-1 - tend to be stubborn.
4. Immunocompromised Patients - A Real Risk
In people with HIV, transplant recipients on immunosuppressants, or others with impaired immunity, HPV can cause extensive, confluent, difficult-to-treat wart infections. The clinical appearance can also differ from that in immunocompetent hosts, making diagnosis harder.
5. Latent Infection Explains Recurrence
HPV can exist as a latent infection in apparently normal skin around the wart - meaning the virus is present even where you can't see it. This is why warts often come back after treatment; destructive methods (burning, freezing) remove the visible lesion but don't eradicate latent virus in surrounding skin.
6. Rare Malignant Risk - Verrucous Carcinoma
Rarely, chronic, long-standing HPV lesions on the foot can transform into verrucous carcinoma (also called epithelioma cuniculatum) - a low-grade squamous cell carcinoma. This is uncommon but is a reason not to ignore a lesion that has been present for years, is growing atypically, bleeds easily, or doesn't respond to any treatment. Biopsy is appropriate in these cases.
When to See a Doctor
| Situation | Why It Matters |
|---|---|
| Wart has been present for years with no response to treatment | Rule out verrucous carcinoma |
| Rapid growth or change in color/shape | Needs evaluation |
| Bleeding, ulceration, or unusual pain | Warrants biopsy |
| You are immunocompromised or diabetic | Higher infection risk; professional management needed |
| Mosaic wart (large cluster) | Harder to treat; needs podiatry/dermatology |
| Affects a child and is spreading | Treat early to prevent spread |
The Bottom Line
Plantar warts caused by HPV-1, 2, 27, and 57 are not cancer-causing and are not dangerous in healthy individuals. They are, however, contagious, painful, and persistent - and in special populations (immunocompromised, diabetic) they carry more serious implications. A wart that behaves unusually or doesn't respond to treatment after months deserves a professional look to rule out other diagnoses.
- Andrews' Diseases of the Skin, Clinical Dermatology (5th Ed)
- Pfenninger & Fowler's Procedures for Primary Care
Oth cream
Asking for Preferences
Why do legs swell red
Reading File
Searching the Web
red swollen leg causes differential diagnosis cellulitis DVT erythema
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a thorough breakdown of all the common reasons legs swell and turn red:
Why Do Legs Swell and Turn Red?
Red + swollen together points toward inflammation, infection, or vascular obstruction. The cause and urgency vary widely. Here are the main ones, from most urgent to least:
🚨 Urgent / Serious Causes
1. Cellulitis (Bacterial Skin Infection)
Most common cause of a hot, red, swollen leg. Bacteria (usually Streptococcus pyogenes or Staphylococcus aureus, including MRSA) invade the deep dermis and subcutaneous tissue through a break in the skin - a cut, wound, insect bite, or even athlete's foot.
- Signs: Redness, warmth, swelling, pain - the classic four signs of inflammation (rubor, calor, tumor, dolor). Skin feels tight and shiny.
- Key feature: Almost always affects one leg only. Bilateral redness is rarely cellulitis.
- Can progress to: Septicemia (bloodstream infection), necrotizing fasciitis ("flesh-eating" infection - rapid spread, severe pain, skin turns dark/blistered)
- Needs: Antibiotics urgently - see a doctor same day.
Fitzpatrick's Dermatology; Jawetz, Melnick & Adelberg's Medical Microbiology
2. Erysipelas
A variant of cellulitis involving the superficial lymphatic vessels. The redness is strikingly bright red with sharply defined borders - this is the distinguishing feature from regular cellulitis (which has ill-defined borders). Often associated with fever. Also caused by Streptococcus and needs antibiotics.
3. Deep Vein Thrombosis (DVT)
A blood clot in the deep veins of the leg. Can cause swelling, warmth, erythema (redness), and tenderness, often along the inner thigh or calf. Some people have no symptoms at all. The danger is that the clot can break off and travel to the lungs (pulmonary embolism) - a life-threatening emergency.
- Key features: Unilateral leg swelling, pain on squeezing the calf, distended surface veins
- Needs: Urgent ultrasound and anticoagulation - go to A&E/ER if suspected.
Thompson & Thompson Genetics and Genomics in Medicine; Rosen's Emergency Medicine
4. Necrotizing Fasciitis
Rare but life-threatening rapidly spreading infection of the fascia (deep tissue layer). The leg appears red initially but quickly turns purple then black, with severe pain disproportionate to appearance, then paradoxically numbness as nerves are destroyed. Surgical emergency.
Common / Chronic Causes
5. Venous Stasis Dermatitis (Chronic Venous Insufficiency)
One of the most frequently misdiagnosed conditions - often mistaken for cellulitis. Caused by damaged venous valves (from previous DVT, varicose veins, or surgery) that allow blood to pool in the lower legs.
- Signs: Reddish-brown or orange-brown discoloration, pitting edema, scaling, itching - typically affects both lower legs symmetrically, around the medial ankle and shin.
- Key feature: Gradual onset, bilateral, often worse at end of day, better on elevation.
- Over time: Skin becomes thick and leathery (lipodermatosclerosis), and venous ulcers can develop.

Tintinalli's Emergency Medicine; Textbook of Family Medicine 9th Ed
6. Contact Dermatitis / Allergic Reaction
Exposure to a substance (soap, cream, bandage adhesive, elastic in socks) triggers an allergic or irritant reaction - causing redness, swelling, and itching. Redness tends to follow the pattern of contact (e.g., sock line). Often bilateral. Can flare over stasis dermatitis from OTC products.
7. Gout
Uric acid crystals deposit in joints. The big toe, ankle, or knee becomes intensely red, hot, and swollen - often overnight. Extremely painful. Gout attacks in the lower leg or ankle can look exactly like cellulitis.
8. Lymphedema
Blocked lymphatic drainage causes non-pitting swelling - initially soft, later becomes firm and "brawny." Can cause reddish discoloration and significantly increases risk of recurrent cellulitis.
Quick "One vs. Both Legs" Rule
| Feature | Think... |
|---|---|
| One red swollen leg, warm, tender | Cellulitis, erysipelas, DVT, gout |
| Both legs red/swollen | Venous stasis, heart failure, contact dermatitis, kidney/liver disease |
| Rapid spread, fever, severe pain | Cellulitis, necrotizing fasciitis - urgent |
| Gradual, chronic, itchy, scaly | Venous stasis dermatitis |
| After a trip/long flight, one leg | DVT - urgent |
| Joint-centered redness | Gout, septic arthritis |
When to Go to A&E / ER Immediately
- Red streaks spreading up the leg (sign of lymphangitis / severe infection)
- Fever with a red swollen leg
- Skin turning purple, dark, blistering, or going numb
- Sudden leg swelling after a long flight or immobility (possible DVT)
- Rapidly expanding redness despite starting antibiotics
A red, swollen leg that persists, worsens, or comes with fever or systemic symptoms needs same-day medical assessment - don't wait on it.
This is a shared conversation. Sign in to Orris to start your own chat.