Evaluation of vertigo?
Reading File
Finding Sources
Searching PubMed
vertigo evaluation diagnosis
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive material to produce a thorough, well-organized answer. Let me compile it all.
Evaluation of Vertigo
Vertigo is the perceived sensation of motion - typically spinning - either of oneself relative to the environment or vice versa. The evaluation starts with carefully characterizing this symptom, since patients use "dizzy" to describe many distinct sensations.
Differential Diagnosis by Duration: The First Branch Point
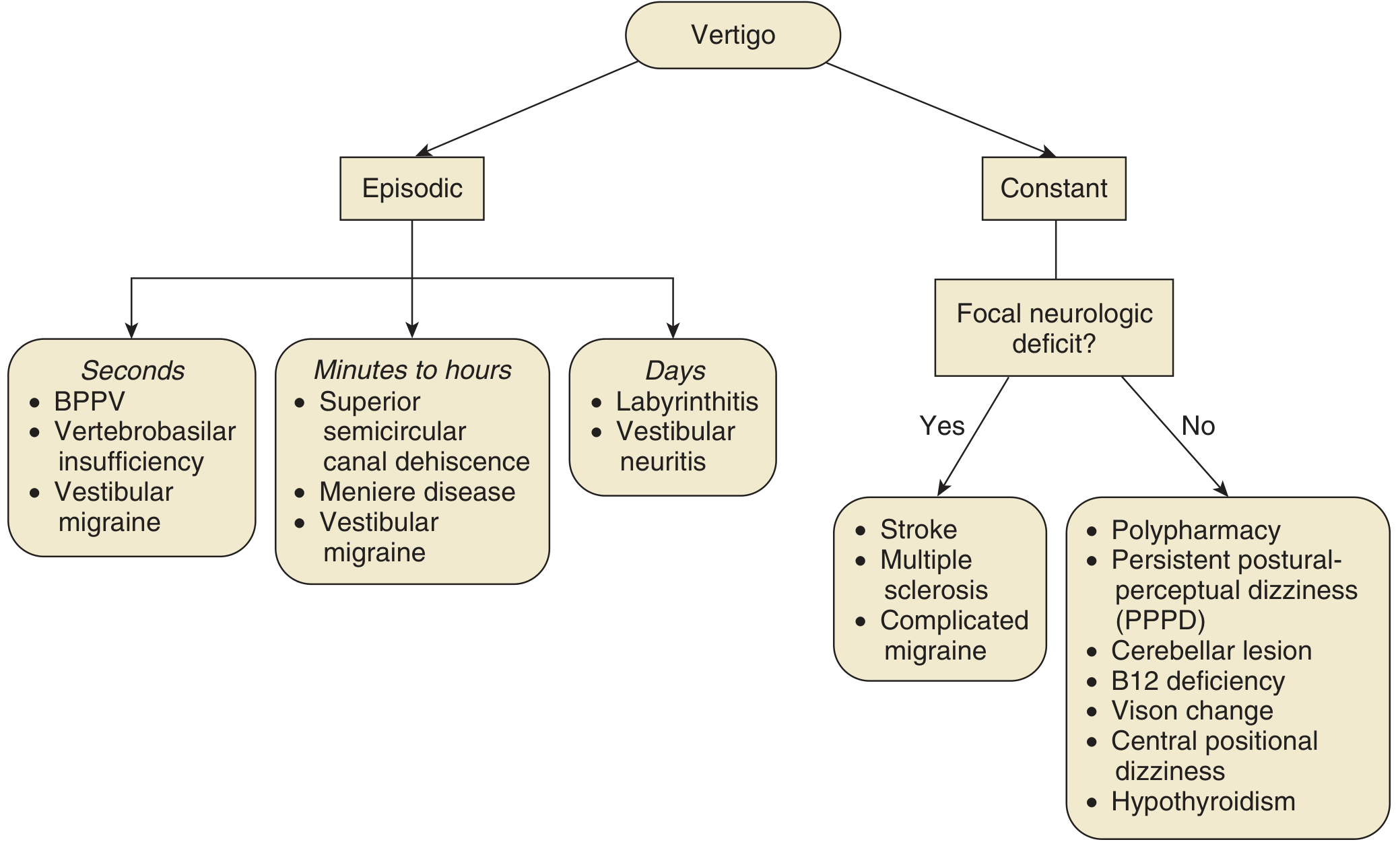
Adapted from Cummings Otolaryngology, Fig. 137.5
Duration drives the differential:
| Duration | Episodic Causes |
|---|---|
| Seconds | BPPV, vertebrobasilar insufficiency, vestibular migraine |
| Minutes to hours | Meniere disease, superior semicircular canal dehiscence, vestibular migraine |
| Days | Vestibular neuritis, labyrinthitis |
| Constant + focal deficits | Stroke, MS, complicated migraine |
| Constant + no focal deficits | PPPD, polypharmacy, cerebellar lesion, B12 deficiency, hypothyroidism |
Step 1: History
History accounts for 85% of diagnostic information in the dizzy patient (Cummings Otolaryngology). Key questions:
Characterize the sensation:
- Is it true spinning vertigo, near-faint/lightheadedness, disequilibrium, or non-specific?
- Onset: acute vs. gradual
- Duration of each episode and total illness duration
- Continuous vs. intermittent
Precipitating/modifying factors:
- Positional change (strongly suggests BPPV)
- Head movement (worsens peripheral and central vertigo)
- Valsalva, loud noise, pressure (suggests perilymphatic fistula or superior canal dehiscence)
Associated ear symptoms (suggest peripheral cause):
- Hearing loss, tinnitus, aural fullness, otalgia, autophony, otorrhea
Neurologic symptoms (red flags for central cause):
- Diplopia, dysphagia, dysarthria, facial numbness, limb weakness/numbness
- Headache, memory loss, personality change, visual auras
- Loss of consciousness (does NOT occur with peripheral vertigo)
Other history:
- Medications (aminoglycosides, loop diuretics, anticonvulsants, antihypertensives)
- Head trauma, recent viral illness, history of migraine
- Cardiovascular disease, diabetes, hypertension
Key peripheral vs. central distinction from history:
- Peripheral vertigo tends to be episodic; central vertigo is more often constant
- Peripheral: no neurologic symptoms, auditory symptoms common
- Central: neurologic symptoms possible, hearing loss less common (except in AICA stroke)
Step 2: Physical Examination
General Exam
- Orthostatic blood pressure - rules out presyncope/near-faint
- Cranial nerve evaluation - focal deficits point centrally
- Gait assessment - tandem walking, Romberg test (falls toward affected side in peripheral disease)
- Ear exam - otoscopy (pneumatic otoscopy can elicit vertigo in perilymphatic fistula)
- Tuning fork tests (Weber, Rinne) - assess for conductive vs. sensorineural hearing loss
- Cardiovascular exam - cardiac murmurs, arrhythmias
Vestibular-Specific Tests
1. Dix-Hallpike Maneuver - for BPPV
- Patient sits on exam table, legs extended; examiner turns head 45° to one side and rapidly lowers to head-hanging position over table edge
- Positive result for posterior canal BPPV:
- Latency of 3-30 seconds before onset of nystagmus/vertigo
- Upbeat-torsional nystagmus (fast phase toward forehead; torsional component toward the downward ear)
- Nystagmus and vertigo escalate then resolve over 5-30 seconds
- May reverse direction when patient returns to sitting
- Fatigability with repeated testing (hallmark of BPPV)
- Supine roll test (Pagnini-McClure) is used if Dix-Hallpike negative, to evaluate horizontal canal BPPV
2. Head Impulse Test (HIT)
- Examiner rapidly turns patient's head ~10° to one side while patient fixates on examiner's nose
- Positive (corrective saccade seen): vestibulo-ocular reflex (VOR) is impaired on that side - indicates peripheral vestibular lesion (e.g., vestibular neuritis) - reassuring (benign)
- Negative (eyes stay on target): VOR intact despite vertigo - suggests a central cause (stroke)
3. Nystagmus Examination (use Frenzel lenses to remove fixation suppression)
| Feature | Peripheral | Central |
|---|---|---|
| Direction | Unidirectional, horizontal or horizontal-torsional | Bidirectional (direction-changing) or purely vertical |
| Fixation | Suppressed by fixation | NOT suppressed |
| Vertical nystagmus | Never | Pathognomonic of central disease |
4. Test of Skew
- Cover-uncover test: any vertical/diagonal movement of the eye on uncovering indicates a central cause
- Vertical skew deviation = strong central sign
The HINTS Exam (for Acute Vestibular Syndrome)
Use ONLY in patients with continuous vertigo lasting hours to days with spontaneous or gaze-evoked nystagmus - i.e., Acute Vestibular Syndrome (distinguishing vestibular neuritis from cerebellar/brainstem stroke).
HINTS = Head Impulse test + Nystagmus + Test of Skew
HINTS-Plus = HINTS + bedside hearing assessment
| Component | Peripheral (reassuring) | Central (dangerous) |
|---|---|---|
| H - Head Impulse | Abnormal (corrective saccade seen) | Normal (no corrective saccade) |
| I - Direction of Nystagmus | Unidirectional | Bidirectional (direction-changing) |
| N - Test of Skew | Absent | Vertical skew present |
| Plus - New hearing loss | No new hearing loss | New hearing loss (suggests AICA stroke) |
"HINTS-Plus = Central" if ANY ONE of: Normal HIT, bidirectional nystagmus, vertical skew, or new hearing loss.
Studies show HINTS performed by neurology residents had 100% sensitivity and 94% specificity for stroke vs. vestibular neuritis - more sensitive than early MRI (Tintinalli's Emergency Medicine).
Step 3: Ancillary Testing
Audiometry
- Indicated when unilateral otologic symptoms (hearing loss, tinnitus) are present
- Low-frequency sensorineural hearing loss is characteristic of Meniere disease
- Ordered after history and exam if cause remains unclear
Electronystagmography (ENG) / Videonystagmography (VNG)
- Objective assessment of vestibular function
- Battery includes: tests of visual-ocular control (saccades, smooth pursuit, optokinetic nystagmus), search for pathologic nystagmus, and measurement of vestibular nystagmus (caloric and rotational)
- Caloric testing: irrigating each ear individually to compare semicircular canal function side-to-side; canal paresis on one side = peripheral lesion
- Useful when cause of vertigo is not clear after history and exam
Neuroimaging
- Brain MRI with posterior fossa protocol is the imaging of choice
- Indicated when:
- Focal neurologic signs or symptoms
- Unilateral otologic symptoms (rule out acoustic neuroma/vestibular schwannoma)
- Failure to respond to treatment
- Suspected central cause
- Acute vestibular syndrome where HINTS suggests central lesion
- Note: Early MRI can miss posterior fossa stroke (false-negative rate up to 20% in first 24-48 hours); HINTS exam may be more reliable early on
Blood Tests
Indicated selectively, not routinely:
- CBC (infection, anemia)
- RPR (syphilis - can cause labyrinthitis)
- Vitamin B12 and folate
- Thyroid function (hypothyroidism)
- Fasting glucose
- Drug levels/toxicology screen
- Heavy metals (if exposure suspected)
Cardiac Workup
- Holter monitor / loop recorder when episodic near-faint is suspected
- ECG, echocardiogram as indicated
Common Diagnoses at a Glance
| Diagnosis | Key Features |
|---|---|
| BPPV | Brief seconds-long episodes triggered by head position change; positive Dix-Hallpike; fatigable nystagmus; no hearing loss |
| Vestibular neuritis | Acute onset constant vertigo lasting days; often follows viral illness; positive HIT; horizontal nystagmus; no hearing loss |
| Labyrinthitis | Like vestibular neuritis but WITH hearing loss (cochlea also involved) |
| Meniere disease | Episodic vertigo (20 min - 12 hours); fluctuating low-frequency SNHL; tinnitus; aural fullness |
| Vestibular migraine | Episodes seconds to days; migraine history; no hearing loss; may have headache, photophobia |
| Posterior fossa stroke | Acute onset; normal HIT; direction-changing nystagmus; skew deviation; focal neuro signs; MRI required |
| PPPD | Chronic (>3 months); worse with standing/motion/visual stimuli; normal neuro-otologic exam; often with anxiety |
Epidemiology Note
- Peripheral vestibular disorders account for 38-56% of persistent dizziness cases
- Psychogenic/PPPD accounts for 6-33%
- Multiple sensory deficits/polypharmacy accounts for ~25%
- Central etiologies represent fewer than 10% of all cases (Textbook of Family Medicine, 9e)
Key References:
- Cummings Otolaryngology Head and Neck Surgery - Chapters 137, 167
- Goldman-Cecil Medicine - Chapter 396 ("Evaluating the Dizzy Patient")
- Harrison's Principles of Internal Medicine 22E - Chapter 24 (Central Vestibular Disorders)
- Rosen's Emergency Medicine - Chapter 15
- Tintinalli's Emergency Medicine - Chapter 170 (HINTS Plus)
- Textbook of Family Medicine, 9e - Chapter 18
This is a shared conversation. Sign in to Orris to start your own chat.