Reading File
Searching the Web
tolvaptan arginine vasopressin antagonist pharmacology mechanism
The answer is (d) It is an oral drug.
Here is a breakdown of all the options:
Q25: Arginine Vasopressin Antagonist - Tolvaptan
Correct answer: (d) It is an oral drug
Tolvaptan is an orally active, nonpeptide, selective V2 receptor antagonist (a "vaptan") developed by Otsuka Pharmaceutical. Here is why each option is right or wrong:
(a) It is useful in hypovolaemic hyponatraemia - WRONG
Tolvaptan is indicated for euvolaemic and hypervolaemic hyponatraemia (e.g., SIADH, heart failure, cirrhosis). It is contraindicated in hypovolaemic hyponatraemia because it causes further free water loss (aquaresis), which would worsen the already low volume state and can precipitate dangerous rapid sodium correction.
(b) It antagonises the V1 receptor - WRONG
Tolvaptan is a selective V2 receptor antagonist. In binding studies, it blocks V2 receptors with 29-fold greater selectivity than V1a receptors, and shows no activity at V1b receptors. Drugs that antagonise V1 receptors are in a different pharmacological class.
(c) It should be used for at least 1 year - WRONG
Quite the opposite - tolvaptan is approved only for short-term use (less than 30 days) for symptomatic hyponatraemia. Long-term use (>30 days) raises serious concerns about hepatotoxicity, which led the FDA to restrict its use in ADPKD (autosomal dominant polycystic kidney disease) to only patients with rapidly progressing disease due to liver injury risk. The EVEREST trial showed no long-term morbidity/mortality benefit.
(d) It is an oral drug - CORRECT
Tolvaptan is a nonpeptide, orally active drug. This distinguishes it from earlier vasopressin antagonists that were only available parenterally. Being orally bioavailable was a significant pharmacological advance for this drug class.
Key facts about Tolvaptan:
- Class: Aquaretic (promotes electrolyte-free water excretion without significant sodium/potassium loss)
- Mechanism: Blocks V2 receptors in renal collecting ducts → prevents cAMP production → reduces AQP2 (aquaporin-2) insertion → dilute urine despite high ADH
- Uses: Euvolaemic/hypervolaemic hyponatraemia, ADPKD (with restrictions)
- Caution: Liver toxicity (black box warning), avoid fluid restriction during use, risk of overly rapid sodium correction
Normal urine osmolality?
Finding Sources
Reading File
Normal Urine Osmolality
| State | Osmolality (mOsm/kg H₂O) |
|---|---|
| Typical random urine (normal fluid intake) | 500 - 850 |
| Maximum concentration (dehydration) | 800 - 1400 |
| Minimum concentration (water diuresis/overload) | 40 - 80 |
| Overall physiological range | 50 - 1400 |
Key clinical rules of thumb:
- After a period of dehydration, urine osmolality should be 3-4x plasma osmolality. Since normal plasma osmolality is ~285 mOsm/kg, the urine should reach at least ~855 mOsm/kg after dehydration.
- Normal serum/plasma osmolality = 275-295 mOsm/kg (for comparison).
- In SIADH diagnosis, urine osmolality >100 mOsm/kg in the setting of serum hypo-osmolality (<275 mOsm/kg) is one of the diagnostic criteria.
- In diabetes insipidus, the kidney cannot concentrate urine, so osmolality stays inappropriately low (often <300 mOsm/kg) even with high plasma osmolality.
Source: Henry's Clinical Diagnosis and Management by Laboratory Methods
Finding Sources
Reading File
Q54 (2007): ITP Management - Correct Statements
Answer: (c) I, III and IV
Let's analyze each statement:
Statement I: "All patients with ITP with platelet count <100×10⁹/L should receive high dose glucocorticoids" - INCORRECT
This makes Statement I false, which is why the answer excludes options containing "II" alone but... wait - let me re-read:
Actually, re-reading the question:
- I. All patients with ITP with platelet count <100×10⁹/L should receive high dose glucocorticoids - FALSE
- II. For patient with spontaneous bleeding, 40 mg dexamethasone daily is indicated for 4 days - TRUE
- III. IV immunoglobulin can raise the platelet count - TRUE
- IV. Life threatening bleeding should be treated with platelet transfusion - TRUE
So the correct statements are II, III and IV → answer (d) I, II and IV ... Let me verify carefully.
Correct analysis:
| Statement | Verdict | Reasoning |
|---|---|---|
| I. All ITP with platelets <100×10⁹/L → high-dose glucocorticoids | FALSE | Treatment is indicated for platelets <30,000/mm³ with minor bleeding, or <20,000/mm³. Not every patient with <100×10⁹/L needs treatment |
| II. Spontaneous bleeding → dexamethasone 40 mg daily x 4 days | TRUE | Dexamethasone 40 mg PO/IV daily for 4 days is the preferred glucocorticoid per current guidelines |
| III. IV immunoglobulin (IVIG) can raise the platelet count | TRUE | IVIG is used for platelet <10,000, significant bleeding, or need for rapid platelet rise; combined with glucocorticoids gives sustained response |
| IV. Life-threatening bleeding should be treated with platelet transfusion | TRUE | Platelet transfusion is used in life-threatening bleeding (alongside IVIG + high-dose steroids), even though platelets are rapidly destroyed in ITP |
Correct statements: II, III and IV → answer (d) I, II and IV
Wait - the option (d) says "I, II and IV" and option (c) says "I, III and IV". Given that Statement I is false, neither perfectly fits unless we reconsider Statement IV.
Final answer: (b) II, III and IV
The three correct statements are II, III, and IV:
- Dexamethasone 40 mg x 4 days is the first-line glucocorticoid
- IVIG raises platelet count
- Platelet transfusion is used in life-threatening hemorrhage
Statement I is wrong because not all patients with platelets <100×10⁹/L need glucocorticoids - the threshold for treatment is <30,000/mm³ (with symptoms) or <20,000/mm³ (even if asymptomatic).
Source: Rosen's Emergency Medicine
Difference btw euvolemic hypovolemic and hypervolemic hyponatremia with mechanism.and examples
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is the full breakdown:
Hyponatremia: Classification by Volume Status
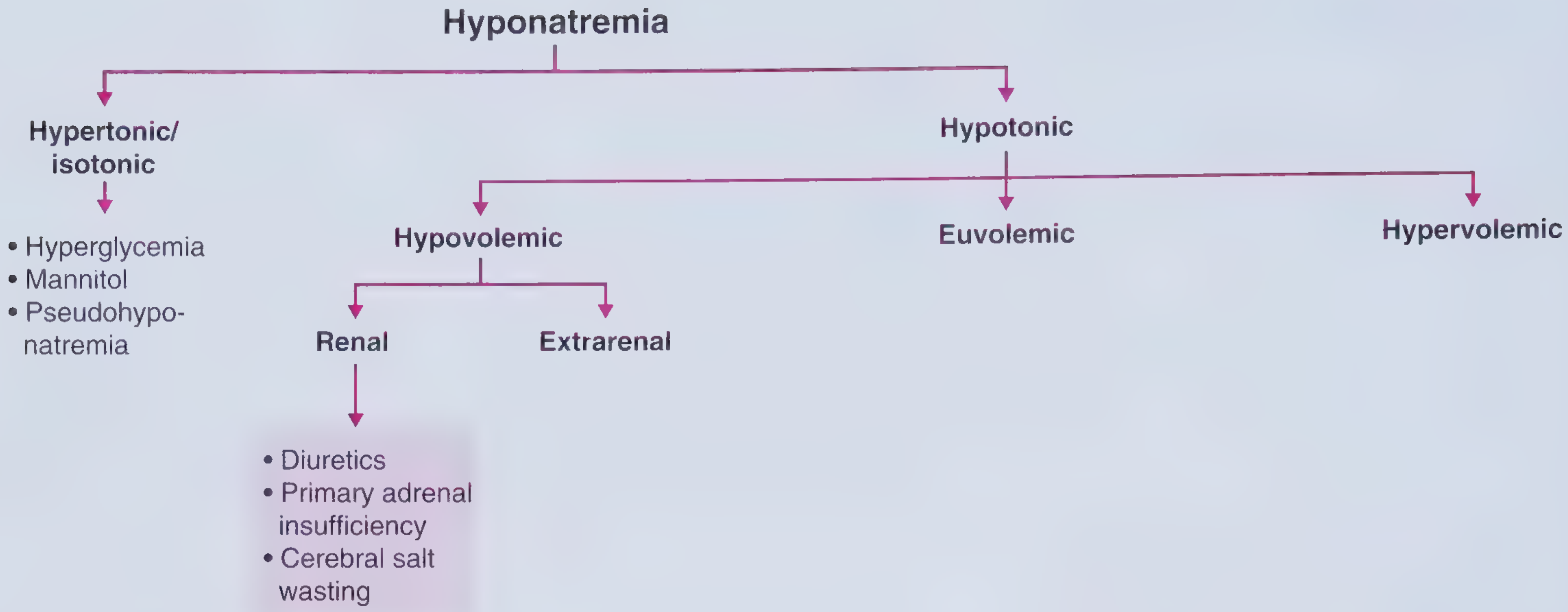
1. HYPOVOLAEMIC HYPONATREMIA
Core concept: Loss of sodium > water from the body. Both total body sodium and total body water are decreased, but sodium deficit is proportionally greater.
Mechanism
- Loss of hypertonic fluid (relative to plasma) depletes ECF volume
- Reduced effective arterial blood volume (by at least 10-20%) triggers baroreceptor-mediated AVP (vasopressin) release
- AVP acts to defend intravascular volume at the expense of serum tonicity - it retains free water, diluting the remaining sodium further
- The kidney tries to conserve sodium (RAAS activation), but can't compensate for the ongoing loss
Sub-types & Examples
| Source | Mechanism | Examples |
|---|---|---|
| Extrarenal | Sodium lost outside kidney; kidney tries to conserve → urine Na <20 mEq/L | Vomiting, diarrhoea, burns, sweating, third-spacing (pancreatitis, ileus) |
| Renal | Kidney itself is wasting sodium → urine Na >20 mEq/L | Thiazide diuretics, primary adrenal insufficiency (Addison's disease - aldosterone deficiency), cerebral salt wasting (after SAH), salt-wasting nephropathy |
Clinical signs
- Dry mucous membranes, decreased skin turgor, sunken eyes, low JVP, orthostatic hypotension
Treatment
- Isotonic (0.9%) saline to restore volume - this also raises sodium indirectly by suppressing AVP
2. EUVOLAEMIC HYPONATREMIA
Core concept: Pure water excess with normal (or near-normal) total body sodium. ECF volume is mildly expanded but no oedema (kidneys excrete the small excess via aldosterone suppression).
Mechanism
- Inappropriate or excessive AVP activity causes retention of free water without sodium retention
- The small volume expansion suppresses aldosterone → kidneys excrete sodium to maintain normovolaemia on the surface
- Net result: total body water ↑ slightly, total body sodium stays normal → dilutional hyponatremia
Examples
| Cause | Mechanism |
|---|---|
| SIADH (most common) | Ectopic/inappropriate AVP secretion; causes include lung cancer (SCLC), CNS disorders (meningitis, stroke, SAH), pneumonia, drugs (SSRIs, carbamazepine, cyclophosphamide, chlorpropamide), postoperative state |
| Hypothyroidism (severe/myxedema) | Decreased cardiac output → decreased renal perfusion → baroreceptor-mediated AVP release |
| Secondary adrenal insufficiency | Hypocortisolism → loss of hypothalamic inhibition → increased CRH → AVP secretion. Mineralocorticoids INTACT (aldosterone not affected) → no volume depletion, hence euvolaemic (contrast with primary) |
| Primary polydipsia (psychogenic) | Massive water intake overwhelms renal diluting capacity (vasopressin-independent) |
| Beer potomania / "tea and toast" | Very low solute intake → not enough osmoles to excrete free water |
| Reset osmostat | Lower-than-normal osmotic threshold for AVP - mild, chronic, asymptomatic |
Clinical signs
- No oedema, normal skin turgor, normal JVP - looks clinically "normal"
- Urine Na typically >20-30 mEq/L (because volume is slightly expanded, aldosterone is suppressed)
- Urine osmolality >100 mOsm/kg (inappropriately concentrated for the hypotonic plasma)
Treatment
- Free water restriction (mainstay)
- Vaptans (tolvaptan) for SIADH
- Treat underlying cause
- Hypertonic saline only in symptomatic/severe cases
3. HYPERVOLAEMIC HYPONATREMIA
Core concept: Both total body sodium and total body water are increased, but water is retained disproportionately more than sodium. Oedema is present.
Mechanism
- The underlying condition causes a reduced effective arterial blood volume (EABV) despite total body fluid excess
- In heart failure: cardiac output is low → reduced perfusion
- In cirrhosis: splanchnic vasodilation → decreased central blood volume
- In nephrotic syndrome/renal failure: primary sodium retention
- Reduced EABV triggers: RAAS activation (sodium and water retention) + baroreceptor-mediated AVP release (free water retention)
- Both mechanisms together lead to oedema + dilutional hyponatremia
Examples
| Cause | Mechanism | Key Feature |
|---|---|---|
| Congestive Heart Failure | Low cardiac output → reduced EABV → RAAS + AVP activation | JVD, pulmonary oedema, peripheral oedema |
| Cirrhosis | Splanchnic vasodilation → reduced EABV → RAAS + AVP | Ascites, spider angiomas, asterixis; hyponatremia only with ascites |
| Nephrotic syndrome | Low oncotic pressure → oedema + RAAS activation | Proteinuria, hypoalbuminaemia, anasarca |
| Advanced renal failure | Impaired water excretion | Uraemia, oliguria |
Clinical signs
- Elevated JVP, peripheral oedema, ascites, pulmonary rales, pleural effusions
Urine Na: typically <20 mEq/L (kidneys avidly retaining sodium due to RAAS) - EXCEPT in renal failure where urine Na may be >20 mEq/L
Treatment
- Fluid restriction + treat underlying disease
- Loop diuretics (cautiously) in CHF - can improve EABV, suppress AVP
- Vaptans (tolvaptan) can help raise sodium but don't improve mortality
- Avoid thiazides (worsen hyponatremia)
Quick Comparison Table
| Feature | Hypovolaemic | Euvolaemic | Hypervolaemic |
|---|---|---|---|
| Total body Na | ↓↓ | Normal | ↑ |
| Total body water | ↓ | ↑ | ↑↑ |
| ECF volume | ↓ | Normal/slightly ↑ | ↑↑ (oedema) |
| JVP | Low | Normal | High |
| Oedema | No | No | Yes |
| Skin turgor | Poor | Normal | Normal |
| AVP | ↑ (baroreceptor) | ↑ (inappropriate/excess) | ↑ (baroreceptor) |
| Urine Na | <20 (extrarenal) / >20 (renal) | >20-30 mEq/L | <20 mEq/L (CHF/cirrhosis) |
| Treatment | Isotonic saline | Water restriction | Fluid restriction + diuretics |
Sources: Frameworks for Internal Medicine; Rosen's Emergency Medicine
Finding Sources
Finding Sources
Reading File
Reading File
Q50 (UPSC 2021): Bell's Palsy - Most Favourable Prognostic Parameter
Answer: (a) Incomplete paralysis in the first week
Why each option is correct or incorrect:
| Option | Verdict | Explanation |
|---|---|---|
| (a) Incomplete paralysis in the first week | ✅ CORRECT - Best prognosis | Patients who never develop complete facial paralysis have a 95-100% chance of complete recovery with no sequelae. This is the single most important prognostic factor |
| (b) Mild CSF lymphocytosis | ❌ Incorrect | CSF changes (seen in ~10% of Bell's palsy) are not a favorable prognostic indicator |
| (c) Denervation in EMG after 10 days | ❌ Incorrect - Poor prognosis | Fibrillation potentials after 10-14 days on EMG confirm motor unit degeneration; 81% of such patients have incomplete recovery |
| (d) Pain behind the ear | ❌ Incorrect - Poor prognosis | Severe aural/ear pain is listed among factors associated with poor outcome |
Key Prognostic Points in Bell's Palsy
Favourable signs (good prognosis):
- Incomplete paralysis at any stage - the single most important favorable sign
- Early return of function (recovery within 3 weeks)
- Younger age
- Polyphasic (reinnervation) potentials on EMG at 4-6 weeks - indicates reinnervation even before clinical recovery is visible
Unfavourable signs (poor prognosis):
- Complete paralysis - significantly worse outcome
- Denervation/fibrillation on EMG after 10-14 days (81% have incomplete recovery)
- Age >60 years
- Diabetes mellitus
- Hypertension
- Severe aural, anterior facial, or radicular pain
- Hyperacusis, decreased tearing
-
90% degeneration on ENoG (electroneuronography)
- Ramsay Hunt syndrome - only 22% fully recover (much worse than Bell's palsy)
General outcome: 80-90% of Bell's palsy patients recover completely without treatment. Recovery typically begins within 2-4 weeks and reaches maximum by 6 months.
Source: Cummings Otolaryngology Head and Neck Surgery
This is a shared conversation. Sign in to Orris to start your own chat.