Stroke
Reading File
Asking for Preferences
I'm physiotherapist so i want to full knowledge on stroke on my pov
Finding Sources
Finding Sources
Searching PubMed
"stroke rehabilitation" AND physiotherapy
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Stroke - A Complete Guide for Physiotherapists
1. DEFINITION
A stroke (cerebrovascular accident, CVA) is the sudden onset of a focal neurological deficit caused by either ischemia (reduced blood flow) or hemorrhage in the brain. It is a medical emergency where "time is brain" - every minute ~1.9 million neurons are lost during a large vessel occlusion.
A TIA (Transient Ischemic Attack) produces similar deficits but fully resolves within 24 hours (usually <1 hour) without infarction - a strong warning sign requiring urgent investigation.
2. TYPES OF STROKE
| Type | Frequency | Mechanism |
|---|---|---|
| Ischemic | ~85% | Vessel occlusion - thrombotic or embolic |
| Hemorrhagic | ~15% | Vessel rupture - intracerebral or subarachnoid |
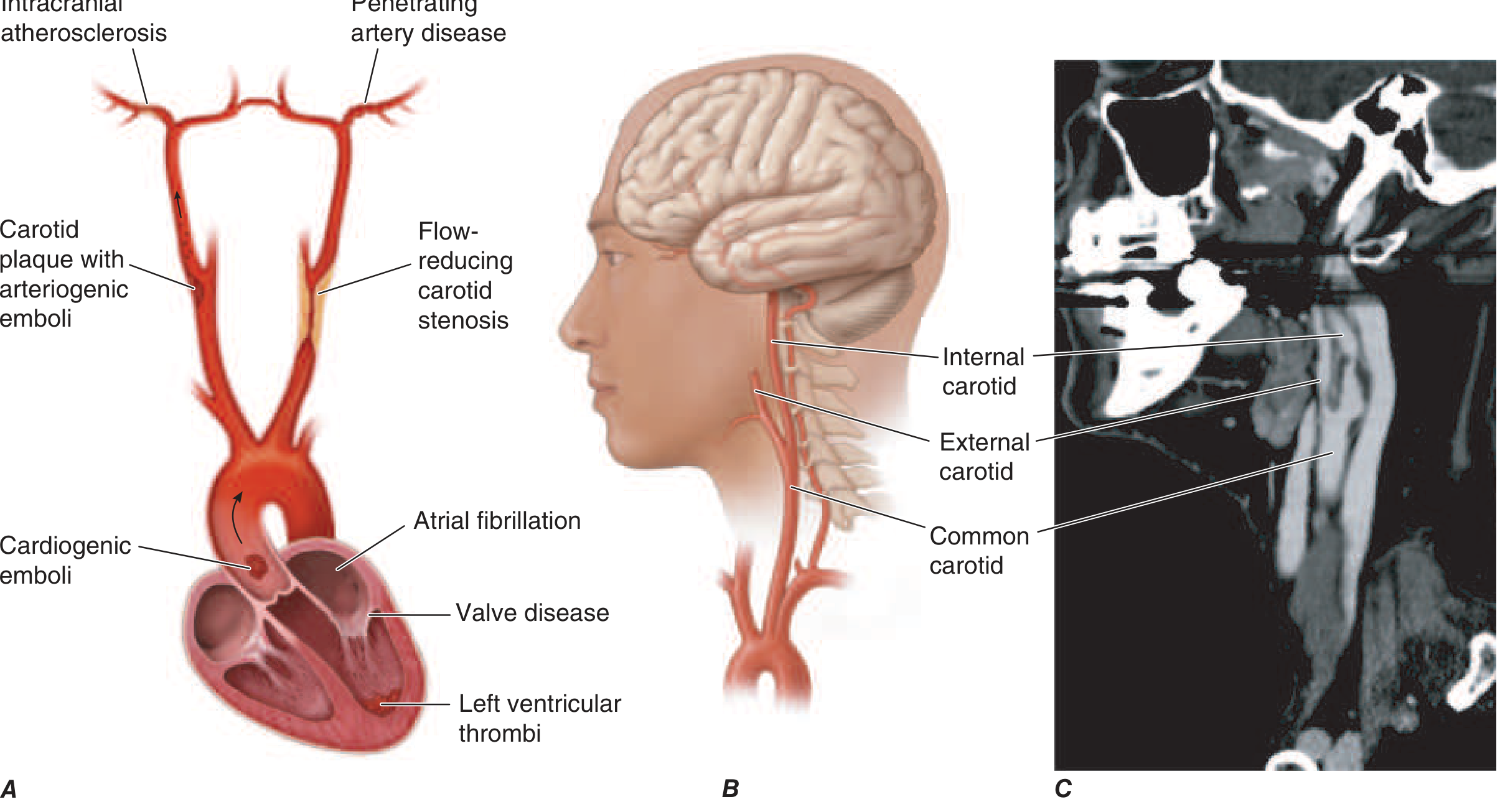
Ischemic Stroke Subtypes (TOAST Classification)
- Large artery atherosclerosis - carotid/vertebral plaque rupture + thrombosis
- Cardioembolism - clot from heart (atrial fibrillation is the most common cause)
- Small vessel / Lacunar - penetrating artery disease; causes pure motor or sensory strokes
- Cryptogenic - no identified cause
- Other determined cause - vasculitis, dissection, coagulopathy
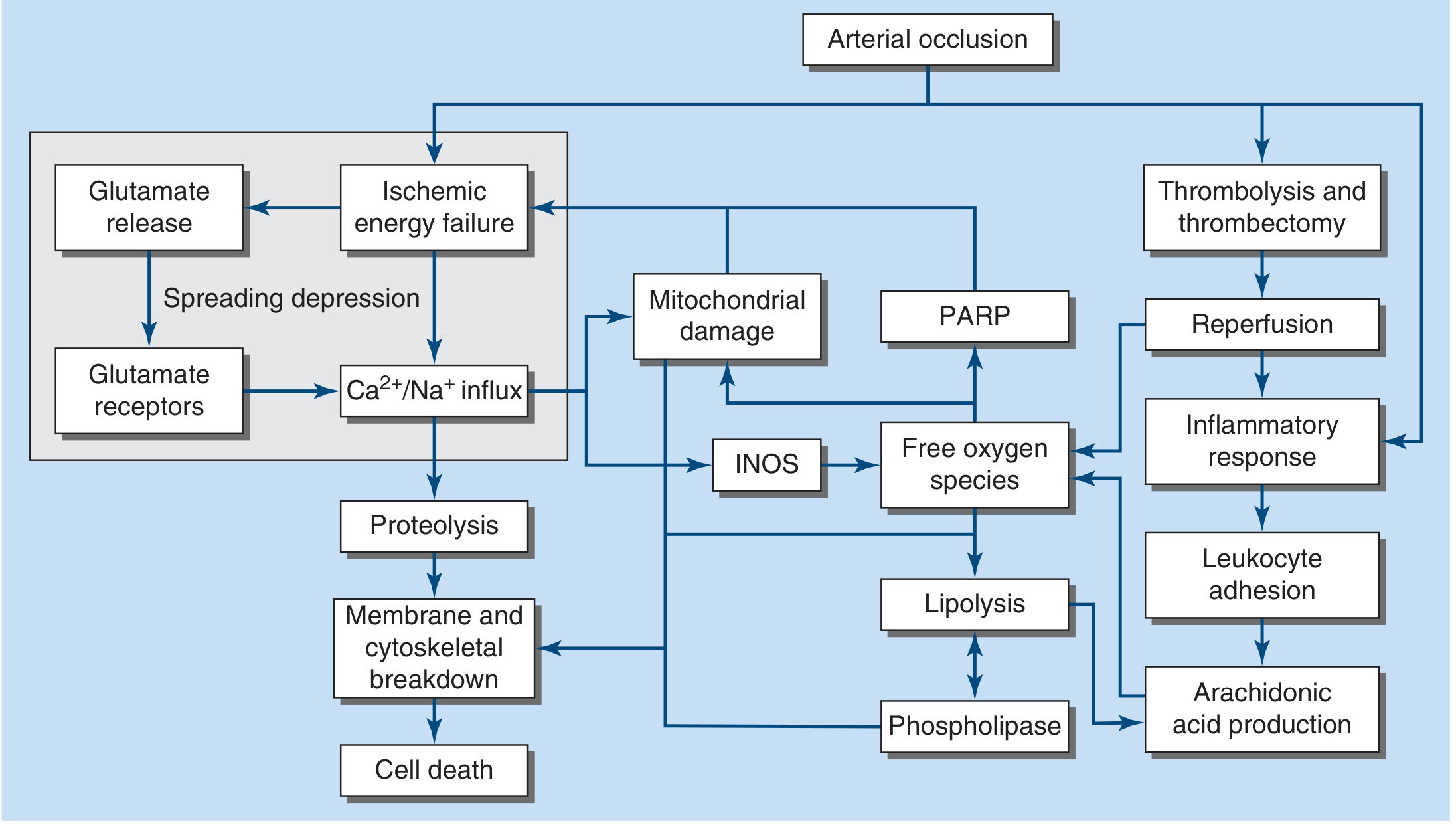
3. PATHOPHYSIOLOGY
Ischemic Cascade
Acute vessel occlusion reduces cerebral blood flow (CBF). Normal CBF = ~50 mL/100g/min.
- CBF < 16-18 mL/100g/min → neuronal dysfunction (recoverable with reperfusion)
- CBF → 0 → brain tissue death within 4-10 minutes
Ischemic core = already infarcted tissue (irreversible)
Ischemic penumbra = surrounding tissue at risk but still viable - the TARGET of rehabilitation and acute intervention
Why this matters for PT: The penumbra is the rationale for early rehabilitation - the injured brain has plasticity and unused neural pathways can be recruited with training even months after large strokes.
4. RISK FACTORS
Non-modifiable: Age (risk doubles each decade after 55), sex (males more at risk), race (higher in Black individuals), family history.
Modifiable (PT can help address these):
- Hypertension (single biggest risk factor)
- Atrial fibrillation
- Diabetes mellitus
- Dyslipidemia
- Smoking
- Physical inactivity - PT role in secondary prevention
- Obesity
- Carotid artery stenosis
5. CLINICAL FEATURES BY VASCULAR TERRITORY
This is essential for a physiotherapist - knowing the artery tells you the likely deficits.
Middle Cerebral Artery (MCA) - Most Common
- Contralateral hemiplegia - upper limb > lower limb (face and arm worse than leg)
- Contralateral hemisensory loss
- Homonymous hemianopia (visual field defect)
- If dominant (usually left) hemisphere: aphasia (Broca's = expressive; Wernicke's = receptive)
- If non-dominant hemisphere: neglect, anosognosia (unawareness of paralysis), constructional apraxia
Anterior Cerebral Artery (ACA)
- Contralateral leg > arm weakness (foot/leg more affected than hand/face)
- Contralateral leg sensory loss
- Urinary incontinence
- Grasp and suck reflexes, abulia (lack of motivation)
Posterior Cerebral Artery (PCA)
- Homonymous hemianopia (pure or with macular sparing)
- Memory impairment
- Thalamic sensory loss
- Less motor involvement than MCA
Brainstem Stroke (Vertebrobasilar)
- Crossed deficits (ipsilateral face + contralateral body) - hallmark
- Lateral Medullary (Wallenberg's) syndrome: dysphagia, ipsilateral Horner's, ataxia, contralateral pain/temperature loss
- Dysarthria, dysphagia, diplopia, vertigo, ataxia
- Locked-in syndrome (basilar artery): conscious but unable to move except eye movements
Lacunar Infarcts (Small Vessel)
- Pure motor hemiparesis (posterior limb of internal capsule or pons)
- Pure sensory stroke (thalamus)
- Ataxic hemiparesis (ipsilateral ataxia + contralateral weakness)
- Dysarthria-clumsy hand syndrome
- Generally better prognosis
Cerebellar Stroke
- Ipsilateral ataxia, dysmetria, dysdiadochokinesia
- Vertigo, nausea, nystagmus
- No hemiplegia unless brainstem compressed
- Risk of fatal herniation into foramen magnum - monitor closely
6. NEUROLOGICAL DEFICITS - THE PT ASSESSMENT FRAMEWORK
Motor Deficits (Most Relevant to PT)
Phase 1 - Flaccid (Acute, days to weeks):
- Hypotonia, absent or decreased reflexes
- Limb is limp; arm hangs, leg buckles
- Risk of shoulder subluxation, contracture, DVT
Phase 2 - Spastic (Subacute to chronic, weeks onwards):
- Spasticity develops gradually
- Upper limb pattern: shoulder adduction + internal rotation, elbow flexion, wrist/finger flexion
- Lower limb pattern: hip extension + adduction, knee extension, ankle plantar flexion + inversion (equinovarus) - the "hemiplegic gait" posture
- Tendon reflexes become brisk, Babinski sign positive
- Botulinum toxin can help relieve focal spasticity
PT Note: Flaccid limbs that remain so (without progressing to spasticity) - especially with extensive temporoparietal lesions - carry a worse prognosis. Early development of spasticity in the arm or early grasp reflex may actually signal a more favorable outcome. - Adams & Victor's Neurology, 12th Ed.
Sensory Deficits
- Hemisensory loss (contralateral to lesion)
- Deep sensory loss (proprioception, vibration) is a major limiting factor for gait and balance rehabilitation
- Pain sensation loss increases risk of pressure sores and burns
Cognitive and Perceptual Deficits
- Neglect (unilateral spatial neglect) - patient ignores affected side - significantly impairs rehabilitation
- Apraxia - inability to perform learned movements despite intact motor and sensory function; movement doesn't "make sense" to patient
- Anosognosia - unawareness of the paralysis; patient may resist therapy
- Attention and concentration deficits
- Memory impairment
- Vascular dementia - multiple infarcts over time lead to cumulative cognitive decline
Communication Deficits
- Aphasia - affects verbal communication; coordinate with speech therapist; use written/picture communication if needed
- Dysarthria - slurred speech but language intact; patient understands commands
Other PT-Relevant Deficits
- Dysphagia - aspiration risk; inform team; sit patient upright for exercises
- Hemianopia - visual field loss; patient may not see on affected side; safety during ambulation
- Bladder/bowel incontinence - usually resolves; manage with pads initially
- Depression and emotional lability - common after left frontal lesions and others; impacts motivation and rehab participation
- Fatigue - very common; patients tire quickly; plan session duration accordingly
- Post-stroke pain - central pain (thalamic), shoulder pain, spasticity pain
7. PROGNOSIS FOR RECOVERY - WHAT TO TELL PATIENTS
- If clinical recovery does not begin in 1-2 weeks, outlook is poorer for both motor and language functions
- Motor and language deficits remaining after 5-6 months are likely to be permanent
- However: aphasia, dysarthria, cerebellar ataxia, and walking may improve for a year or longer
- Nearly all hemiplegic patients regain the ability to walk to some extent, usually within 3-6 months - this should be the primary PT aim
- Key limiting factors for ambulation: deep sensory loss + anosognosia (in addition to hemiplegia)
- Lacunar infarct patients generally fare well but may take months to reach maximum improvement
- Constructional apraxia, neglect, hemianopia - tend to diminish over weeks but hemianopia that hasn't cleared in weeks is usually permanent
Source: Adams and Victor's Principles of Neurology, 12th Ed.
8. PHYSIOTHERAPY MANAGEMENT - BY PHASE
Phase 1: Acute (ICU/Acute Ward, Day 1 onwards)
Start as soon as stroke is completed and blood pressure is stable.
Goals:
- Prevent complications of immobility
- Preserve joint range of motion
- Maintain skin integrity
- Begin early mobilization
Interventions:
- Passive range of motion (PROM): Carry paralyzed limbs through full ROM several times daily - prevents contracture (capsulitis), especially at shoulder, elbow, hip, knee, and ankle
- Positioning: Correct anti-spasticity positioning in bed and chair; protect shoulder from subluxation
- Early mobilization: Move patient from bed to chair as soon as BP is stable
- DVT prophylaxis: Compression boots + active exercise when possible
- Swallowing assessment - critical before oral intake; PT assists with positioning (upright) to reduce aspiration risk
- Respiratory physiotherapy if needed (pneumonia prevention)
- Avoid immobilizing splints - studies have shown undesirable effects of prolonged splinting after stroke
Acute Complications to Monitor:
- Shoulder pain / capsulitis - begin early shoulder PROM; avoid traction on flaccid shoulder
- DVT - calf squeeze, early mobilization
- Pressure sores - positioning, regular turning
- Aspiration pneumonia - positioning, oral hygiene, swallow screening
Phase 2: Subacute Rehabilitation (Inpatient Rehab, Weeks to Months)
Goals:
- Maximize motor recovery and neuroplasticity
- Achieve independent ambulation
- Independence in ADLs
- Manage spasticity
Evidence-Based Interventions:
Neuroplasticity Principles Underlying All PT:
The injured brain has plasticity - remodeling and reorganization of neural function occurs with training. Physical therapy can recruit unused neural pathways even months after large strokes.
1. Task-Specific Training
- Practice actual functional tasks repeatedly (walking, reaching, transfers)
- Intensity matters - more therapy = better outcomes: adding just 30 min/day of focused treatment to leg or arm (5 days/week for 20 weeks) achieves significantly better walking ability and dexterity - Adams & Victor, Kwakkel RCT
2. Gait Retraining
- Progressive gait training - parallel bars → walker → cane → independent
- Ankle-Foot Orthosis (AFO): Use early to assist foot clearance and knee control. Improves weight-bearing on affected leg, increases single-limb stance time, reduces postural sway. Indicated for:
- Inadequate dorsiflexion for heel contact or toe clearance
- Excessive hip hiking during swing
- Mediolateral subtalar instability
- Tibial instability during stance
- AFO set in slight plantarflexion if knee buckles (extends knee earlier); 5° dorsiflexion decreases knee hyperextension
- Treadmill training with body weight support - allows earlier gait practice
- Balance training - dynamic balance, reactive balance, perturbation training
3. Constraint-Induced Movement Therapy (CIMT)
- Immobilize the unaffected upper limb (mitt on good hand) and force use of hemiplegic limb >90% of waking time for 2 weeks
- Reflects cortical motor representation expansion into adjacent undamaged areas
- Benefits shown even years after stroke - Wolf RCT, Adams & Victor
- Current Cochrane review (2025) confirms physical rehabilitation improves function and mobility
4. Strength Training
- Resistance training is safe and effective post-stroke
- Recent meta-analysis (BJSM 2025) confirms strength training improves muscle strength, function, and quality of life
- Progressive resistance exercises for upper and lower limbs
5. Mirror Therapy
- Patient views mirror image of moving unaffected limb creating illusion of moving paretic side
- Cochrane meta-analysis of 14 studies: modest benefit in motor recovery + more prominent benefit for pain relief and quality of life - Adams & Victor
6. Balance and Proprioception Training
- Standing balance exercises
- Perturbation training
- Core stability
- Visual feedback training (mirror, video)
- Particularly important when deep sensory loss is present
7. Spasticity Management
- Prolonged stretching - daily passive stretching of spastic muscles
- Positioning - anti-spasticity positioning (shoulder abduction, elbow extension, wrist/fingers extension; ankle in neutral)
- Splinting - static night splints at wrist/ankle to maintain length
- Functional electrical stimulation (FES) - reduces spasticity, improves voluntary activation
- Cryotherapy - temporary reduction in spasticity
- Coordination with medical team for botulinum toxin injections when splinting insufficient
8. Sensory Retraining
- Graded tactile stimulation
- Proprioceptive exercises
- Mirror therapy for sensory as well as motor deficits
- Attention to safety for patients with deep sensory loss
9. Dysphagia (if trained in oro-motor rehab)
- Positioning strategies (upright sitting, chin tuck)
- Oral motor exercises
- Recent meta-analysis (2023) supports transcranial direct current stimulation for post-stroke dysphagia
10. Virtual Reality (VR) Rehabilitation
- Recent Cochrane review (June 2025) shows VR improves upper limb function and activity compared to conventional therapy or as a dose-matched supplement
- Engaging, repetitive, task-specific - promotes neuroplasticity
- Increasingly available as affordable technology
Phase 3: Community/Home Rehabilitation
Goals:
-
Maintain and build on gains
-
Prevent secondary complications (falls, re-stroke, deconditioning)
-
Maximize participation in home/community
-
Home exercise programs - self-management skills
-
Falls prevention - home environment assessment, balance training, footwear
-
Aerobic exercise - walking programs, cycling; beneficial for cardiovascular risk (secondary stroke prevention)
-
Home-based exercise for post-stroke depression - systematic review (2024) confirms home exercise reduces post-stroke depression
-
Caregiver training in handling, transfers, passive exercises
-
Community ambulation training
9. OUTCOME MEASURES USED IN STROKE PT
| Measure | Assesses |
|---|---|
| Fugl-Meyer Assessment (FMA) | Motor impairment (upper + lower limb) - gold standard |
| Berg Balance Scale (BBS) | Balance and fall risk |
| 10-Metre Walk Test (10MWT) | Gait speed |
| 6-Minute Walk Test (6MWT) | Walking endurance |
| Timed Up and Go (TUG) | Functional mobility |
| Barthel Index / FIM | Activities of daily living |
| Modified Ashworth Scale (MAS) | Spasticity grading |
| NIHSS | Overall neurological severity (medical use; useful for PT context) |
| Motricity Index | Simple bedside motor assessment |
10. SHOULDER PAIN - A KEY PT CONCERN
Shoulder pain is one of the most common complications post-stroke (30-40% of patients). Causes include:
- Subluxation - from hypotonic deltoid pulling humeral head inferiorly
- Capsulitis / frozen shoulder - from immobility; begins early if PROM not started
- Shoulder-hand syndrome (Complex Regional Pain Syndrome Type 1) - pain, atrophy of bone in hand accompanying shoulder pain
- Rotator cuff tear - from improper handling or falls
Prevention is better than treatment:
- Correct positioning and support of flaccid shoulder from day 1
- Avoid traction (pulling on the arm during transfers)
- Begin shoulder PROM within days of stroke
- Arm slings in standing/ambulation when shoulder is subluxed and flaccid
11. STROKE UNIT & MULTIDISCIPLINARY TEAM
As a physiotherapist you work within a multidisciplinary stroke team. Care in stroke units reduces mortality and improves neurologic outcomes.
| Team Member | Primary Role |
|---|---|
| Physiotherapist | Motor recovery, gait, balance, transfers, respiratory |
| Occupational Therapist | Upper limb function, ADLs, cognitive rehab, home assessment |
| Speech & Language Therapist | Dysphagia, aphasia, communication |
| Neurologist / Physician | Medical management, thrombolysis, secondary prevention |
| Nurse | Pressure care, bladder/bowel, medication |
| Social Worker | Discharge planning, family support, community resources |
| Neuropsychologist | Cognitive and emotional deficits |
| Orthotist | AFO fitting and adjustment |
12. SECONDARY PREVENTION - PT'S ROLE
Physiotherapists play a direct role in modifying lifestyle risk factors:
- Physical activity counseling - regular aerobic exercise reduces BP, glucose, lipids
- Exercise prescription for cardiovascular fitness
- Weight management guidance
- Falls prevention strategies
- Encourage smoking cessation, medication adherence (education)
13. NEUROPLASTICITY - THE SCIENCE BEHIND YOUR WORK
Key principles that underpin all stroke PT:
- Use it or lose it - neurons that don't fire together lose their connections
- Use it and improve it - training drives specific brain changes
- Specificity - the training must be task-specific to the goal
- Repetition matters - thousands of repetitions are needed for plastic change
- Intensity matters - more therapy time = better outcomes
- Time matters - earlier is better; there is a critical window but recovery continues for years
- Salience - meaningful, engaging tasks drive greater plasticity
- Transference - skills gained in one context transfer to others (limited)
The nervous system is more adaptable than previously thought. CIMT and mirror therapy studies show cortical motor representation can expand into adjacent undamaged areas. - Harrison's Principles of Internal Medicine 22E; Adams & Victor 12th Ed.
14. RED FLAGS DURING REHABILITATION
Stop therapy and inform the medical team if you observe:
- Sudden worsening of neurological deficits (stroke extension or new stroke)
- Severe headache, vomiting, decreased consciousness (hemorrhagic transformation)
- BP > 220/120 mmHg (ischemic) or significant hypo/hypertension
- Signs of DVT (unilateral calf swelling, pain, warmth)
- Aspiration during oral feeding (coughing, desaturation, wet voice)
- Chest pain, arrhythmia, significant desaturation during exercise
- Signs of seizure activity
Key Sources:
- Harrison's Principles of Internal Medicine, 22nd Ed. (McGraw Hill, 2025) - Chaps 437/438
- Adams and Victor's Principles of Neurology, 12th Ed.
- Bradley and Daroff's Neurology in Clinical Practice
- Cochrane Review: Physical rehabilitation approaches for stroke recovery (2025) - PMID 39932103
- Prescribing strength training for stroke recovery (BJSM 2025) - PMID 39406459
- Virtual reality for stroke rehabilitation, Cochrane 2025 - PMID 40537150
- Home-based exercise for post-stroke depression (2024) - PMID 38290424
This is a shared conversation. Sign in to Orris to start your own chat.