Cancer of larynx ent
Reading File
Finding Sources
Finding Sources
Searching PubMed
"laryngeal cancer" AND treatment
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full answer.
Cancer of the Larynx
Epidemiology
Laryngeal carcinoma represents about 2% of all cancers. It occurs most commonly after age 40, with a strong male predominance (M:F ratio of 7:1). The sixth decade is the most typical presentation age. - Robbins & Kumar Basic Pathology, p. 494
Etiology and Risk Factors
- Tobacco smoking - the dominant risk factor; risk is proportional to exposure. Prior to malignant transformation, epithelial changes can regress after smoking cessation.
- Alcohol - synergizes with tobacco to substantially increase risk.
- Asbestos exposure.
- HPV infection (especially types 16 and 18) - found in about 15% of tumors; these tend to have a better prognosis.
- Irradiation, nutritional factors.
- Robbins Pathologic Basis of Disease, p. 693; Basic Pathology, p. 494
Histopathology
- ~95% are squamous cell carcinomas (SCC); adenocarcinomas are rare.
- Gross appearance: pearly gray, wrinkled mucosal plaques progressing to ulcerated, fungating masses.
- Adjacent mucosa commonly shows squamous hyperplasia, dysplasia, or carcinoma in situ - reflecting the Hyperplasia-Dysplasia-Carcinoma sequence.
- Mild dysplasia: 1-2% risk of malignant transformation over 5-10 years.
- Severe dysplasia: 5-10% risk.
- Histologically well- to moderately-differentiated keratinizing SCC in most glottic tumors. - Robbins Pathologic Basis of Disease
Anatomical Classification (Sites)
The larynx is divided into three zones, each with distinct behavior:
| Site | Frequency | Lymphatics | LN Metastasis | Prognosis |
|---|---|---|---|---|
| Glottis (true vocal cords) | 60-75% | Sparse | 1-4% | Best - ~90% confined at diagnosis |
| Supraglottis (epiglottis, false cords, aryepiglottic folds, arytenoids) | 25-40% | Rich | ~30% | Intermediate |
| Subglottis (below cords) | <5% | Rich | High (bilateral) | Worst - presents late |
The supraglottic larynx includes the upper half of the ventricle, false vocal cords, arytenoids, aryepiglottic folds, and epiglottis. Laryngeal cartilages (thyroid, cricoid), the conus elasticus, quadrangular membrane, hyoepiglottic ligament, and thyrohyoid membrane act as barriers to spread. - Schwartz's Principles of Surgery, p. 668
Clinical Features
- Glottic tumors: Early hoarseness (dysphonia) - most common presenting symptom. Because they interfere with vocal cord mobility early and lymphatics are sparse, they present at an early stage.
- Supraglottic tumors: "Hot potato voice," dysphagia, referred otalgia, neck mass. Symptoms appear late, so nodal metastases are common at presentation.
- Subglottic tumors: Vocal cord paralysis and/or airway compromise. Very few early symptoms.
- General features: progressive voice change, dysphagia, weight loss, referred otalgia, stridor (late).
- Vocal cord fixation results from paraglottic space invasion, cricoarytenoid joint involvement, or recurrent laryngeal nerve (RLN) invasion. - Schwartz's Principles of Surgery
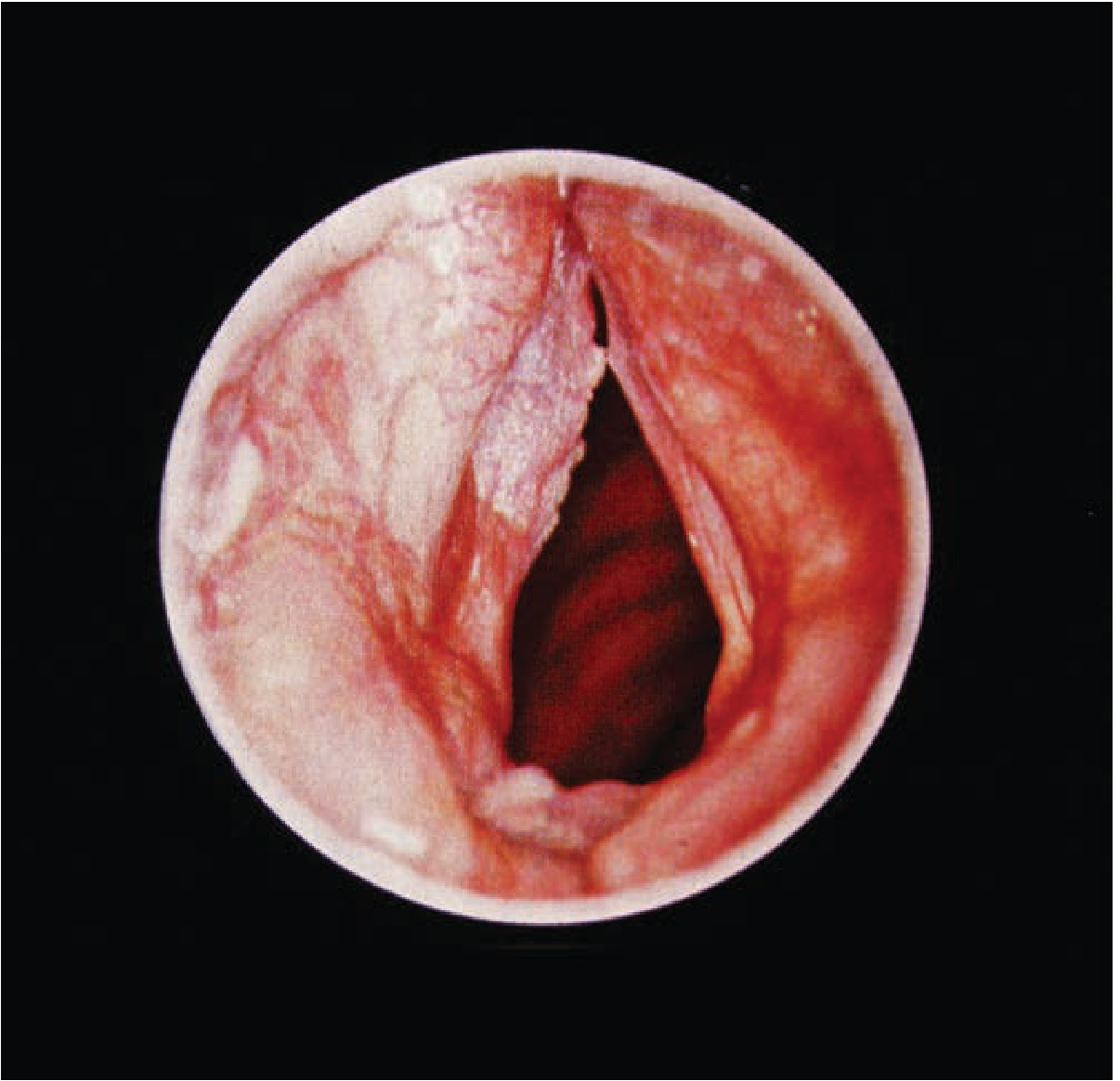
Endoscopic view of laryngeal SCC - Schwartz's Principles of Surgery
Workup and Staging
- Direct laryngoscopy - assesses local tumor extent, vallecula, base of tongue involvement, subglottic extension. Also allows biopsy and planning of surgical entry if laryngectomy is needed.
- Esophagoscopy + bronchoscopy - assess for synchronous second primary tumors.
- CT scan with contrast (preoperative) - evaluates cervical lymphadenopathy, thyroid/cricoid cartilage invasion, preepiglottic and paraglottic space extension.
- MRI - superior for soft tissue and skull base assessment.
- PET-CT - complete staging, radiation field planning.
Lymphatic Drainage (for staging)
- Supraglottis: drains via neurovascular bundle through thyrohyoid membrane to upper/lateral cervical nodes (levels II-IV).
- Glottis/Subglottis: drains through cricothyroid membrane to Delphian (prelaryngeal) nodes, paratracheal nodes, and lower cervical nodes (levels IV and VI).
- Schwartz's Principles of Surgery
TNM Staging (AJCC)
| T Stage | Description |
|---|---|
| T1 | Confined to subsite, normal cord mobility |
| T2 | Extends to adjacent site or subglottis; impaired cord mobility |
| T3 | Cord fixation; limited preepiglottic/paraglottic space invasion |
| T4a | Invasion through cartilage or into extralaryngeal soft tissues |
| T4b | Prevertebral, encases carotid, or mediastinal involvement |
Management
Principles
- Early-stage (T1-T2): Single-modality treatment - surgery OR radiotherapy.
- Advanced-stage (T3-T4): Combined modality - surgery + radiotherapy ± chemotherapy, OR concurrent chemoradiotherapy for organ preservation.
- Larynx-preservation is a key goal; the VA Laryngeal Cancer Study showed concurrent chemoradiation is effective for laryngeal preservation in advanced disease.
Glottic Carcinoma
- T1/T2 glottic - managed with single modality: radiotherapy OR transoral laser microsurgery (TLM) / conservation laryngeal surgery (partial laryngectomy). Both give equivalent oncologic results with high cure rates.
- T3/T4 glottic - concurrent chemoradiation (cisplatin-based) for laryngeal preservation; total laryngectomy if preservation fails or primary functions are compromised.
Supraglottic Carcinoma
- Typically treated with primary concurrent chemoradiotherapy for organ preservation.
- Surgery (supraglottic laryngectomy or total laryngectomy) if chemoradiation fails or primary laryngeal functions are irrecoverably lost.
- Bilateral neck dissection is commonly required due to bilateral lymphatic drainage.
Subglottic Carcinoma
- No difference in survival between surgery-first vs. chemoradiation-first approaches.
- Concurrent chemoradiotherapy is the modality of choice for laryngeal preservation.
- Surgical salvage has lower cure rates and increased wound complications.
- Rare early T1 lesions without adenopathy may be treated with primary radiotherapy alone.
Total Laryngectomy
- Indications: T4 disease with cartilage invasion, failure of organ-preservation therapy, poor laryngeal function after organ-preservation attempts.
- Involves removal of larynx from epiglottis to inferior cricoid border, total thyroidectomy, and bilateral neck dissection (levels II-IV + level VI).
- Creates a permanent tracheostoma.
- Reconstruction with pedicled pectoralis major flap or free flaps (radial forearm, anterolateral thigh) when pharyngeal reconstruction is needed.
- Schwartz's Principles of Surgery, p. 668-669
Prognosis
| Stage/Site | Behavior |
|---|---|
| Glottic T1/T2 | Excellent cure rates (>90%) with single modality |
| Supraglottic | ~30% present with regional metastasis; worse than glottic |
| Subglottic | Worst prognosis due to late presentation and bilateral nodal spread |
| HPV-positive | Better overall prognosis |
Prognosis is directly related to clinical stage. Thyroid/cricoid cartilage invasion and preepiglottic/paraglottic space extension significantly worsen outcomes. - Robbins & Kumar Basic Pathology; Schwartz's Principles of Surgery
Summary Key Points
- 95% SCC - linked to tobacco and alcohol in chronic smokers, typically males >40 years.
- Glottic tumors most common (60-75%) and have the best prognosis due to early hoarseness and sparse lymphatics.
- Supraglottic tumors - rich lymphatics, ~30% have nodal mets at diagnosis.
- Subglottic tumors - rarest, worst prognosis, presents late.
- Workup: direct laryngoscopy + biopsy, CT neck, PET-CT for staging.
- Early disease: single modality (surgery or RT). Advanced disease: concurrent chemoradiation ± surgery.
- Laryngeal preservation is the primary goal for advanced disease using chemoradiation (VA Laryngeal Study protocol).
Sources: Robbins Pathologic Basis of Disease, Robbins & Kumar Basic Pathology, Schwartz's Principles of Surgery 11e, Mulholland & Greenfield's Surgery 7e, Cummings Otolaryngology Head and Neck Surgery.
I asked ent dingara
Asking for Preferences
"Dingara" likely means diagram - a visual/diagrammatic representation. Here is a structured diagrammatic layout for Cancer of the Larynx (ENT):
🔷 CANCER OF LARYNX — Diagrammatic Notes
CANCER OF LARYNX
|
┌────────────────┼────────────────┐
SUPRAGLOTTIS GLOTTIS SUBGLOTTIS
(25-40%) (60-75%) (<5%)
| | |
Late symptoms EARLY hoarseness Late airway
Dysphagia (earliest sx) compromise
Neck mass Cord fixation
| | |
Rich lymphatics SPARSE lymphatics Rich lymphatics
~30% LN mets 1-4% LN mets Bilateral mets
| | |
WORST at staging BEST prognosis WORST prognosis
🔷 ETIOLOGY (Risk Factors)
┌─────────────────────────────────┐
│ LARYNGEAL CARCINOMA │
└────────────┬────────────────────┘
│
┌───────────────┼───────────────────┐
▼ ▼ ▼
TOBACCO ALCOHOL HPV (16,18)
(Main factor) (Synergistic) ~15% of tumors
Risk ∝ dose Better prognosis
▼ ▼ ▼
ASBESTOS RADIATION NUTRITIONAL
exposure exposure deficiency
🔷 PATHOLOGY
HYPERPLASIA → DYSPLASIA → CIS → INVASIVE CARCINOMA
| |
No risk Mild dysplasia → 1-2% risk (5-10 yrs)
Severe dysplasia → 5-10% risk
95% = SQUAMOUS CELL CARCINOMA
↓
Pearly gray → Ulcerated → Fungating mass
🔷 CLINICAL FEATURES
GLOTTIC SUPRAGLOTTIC SUBGLOTTIC
| | |
Hoarseness Hot potato voice Stridor
(EARLIEST) Dysphagia Airway obstruction
Referred otalgia Cord fixation/paralysis
Neck mass (30%)
Common features all sites: Dysphagia, weight loss, referred otalgia, vocal cord fixation (late)
🔷 WORKUP / INVESTIGATIONS
SUSPECTED LARYNGEAL CA
|
▼
Direct Laryngoscopy + BIOPSY ← Gold standard
|
├──► CT Neck (contrast) — cartilage invasion, LN, paraglottic space
├──► MRI — soft tissue detail
├──► PET-CT — distant mets, staging
└──► Panendoscopy — rule out second primary
(laryngoscopy + esophagoscopy + bronchoscopy)
🔷 TNM STAGING (Glottis)
| T Stage | Key Feature |
|---|---|
| T1 | Limited to cord(s), normal mobility |
| T2 | Extends to supra/subglottis OR impaired mobility |
| T3 | Cord fixation / paraglottic space invasion |
| T4a | Cartilage erosion / extralaryngeal spread |
| T4b | Prevertebral / encases carotid / mediastinum |
🔷 MANAGEMENT FLOWCHART
LARYNGEAL CANCER
|
┌───────────┴────────────┐
EARLY (T1-T2) ADVANCED (T3-T4)
| |
Single modality Combined modality
| |
┌─────┴──────┐ ┌─────────┴──────────┐
SURGERY RT Chemo + RT Surgery + RT
(TLM/partial (Larynx (if preservation
laryngectomy) preservation) not possible)
|
TOTAL LARYNGECTOMY
(if functions lost /
RT fails)
|
Permanent tracheostoma
+ Neck dissection (II-VI)
+ Reconstruction (pec major
flap / free flap)
🔷 PROGNOSIS SUMMARY
BEST ──────────────────────────────── WORST
| |
GLOTTIC SUPRAGLOTTIC SUBGLOTTIC
T1/T2 T3-T4 All stages
90% confined 30% LN mets Late presentation
at diagnosis at presentation Bilateral nodes
HPV+ tumors → Better prognosis than HPV- tumors
🔷 HIGH-YIELD EXAM POINTS
| Fact | Detail |
|---|---|
| Most common site | Glottis (60-75%) |
| Earliest symptom | Hoarseness (glottic) |
| Best prognosis site | Glottis |
| Worst prognosis site | Subglottis |
| Histology | 95% SCC |
| Age/Sex | >40 yrs, M:F = 7:1 |
| Lymph node-free site | Glottis (sparse lymphatics) |
| Organ preservation protocol | Concurrent chemoradiation |
| Delphian node | Pre-laryngeal node — involved in glottic/subglottic spread |
| Gold standard diagnosis | Direct laryngoscopy + biopsy |
This is a shared conversation. Sign in to Orris to start your own chat.