Leprosy according to Harsh Mohan textbook of pathology
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Finding Sources
Reading File
Finding Sources
Loading Image
I now have all the material needed for a comprehensive response. Note that Harsh Mohan's Textbook of Pathology is not in the library, but I have pulled the equivalent content from Robbins (the international gold standard for pathology), supplemented with Park's and other sources. I'll present this clearly.
Note: Harsh Mohan's Textbook of Pathology is not available in this library's collection. The content below is drawn primarily from Robbins, Cotran & Kumar Pathologic Basis of Disease (the equivalent international pathology standard) and supplemented with Park's Textbook of Preventive & Social Medicine and other authoritative sources. The pathological concepts are identical to what Harsh Mohan covers.
Leprosy (Hansen Disease) - Pathology
Definition and Epidemiology
Leprosy (Hansen disease) is a slowly progressive chronic granulomatous infection caused most often by Mycobacterium leprae and, less frequently, by the more recently proposed M. lepromatosis (named 2008). It primarily affects the skin and peripheral nerves.
- Despite low communicability, ~200,000 new infections/year globally
- Endemic in Southeast Asia, East Africa, and Brazil
- M. leprae cannot be cultured in vitro; proliferates best at 32-34°C (temperature of human skin)
- Transmitted via human respiratory secretions; rare zoonotic transmission from armadillos
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 356
Pathogenesis
M. leprae is an obligate intracellular pathogen taken up by dermal macrophages. Key points:
- Disseminates via blood but replicates primarily in cool tissues (skin, extremities)
- Virulence is based on cell wall properties; bacterial lipid PGL-1 is critical for host cell invasion
- Inhibits mitochondrial energy metabolism to evade immune response
- Secretes no exotoxins
- BCG immunization confers some cross-protection (similar enough to M. tuberculosis)
The spectrum of disease is determined entirely by the host's helper T-lymphocyte (CD4+) response:
| Feature | Tuberculoid (TT) | Lepromatous (LL) |
|---|---|---|
| Immune response | Strong Th1 + Th17 | Weak Th1; Th2/regulatory T cells dominant |
| Cytokines | IL-2, IFN-γ | IL-4, IL-10 |
| Bacterial load | Low (paucibacillary) | High (multibacillary) |
| Cell-mediated immunity | Intact | Deficient |
| Antibodies | Low | High (but non-protective) |
- In lepromatous leprosy, antibodies form immune complexes that can cause erythema nodosum, vasculitis, and glomerulonephritis
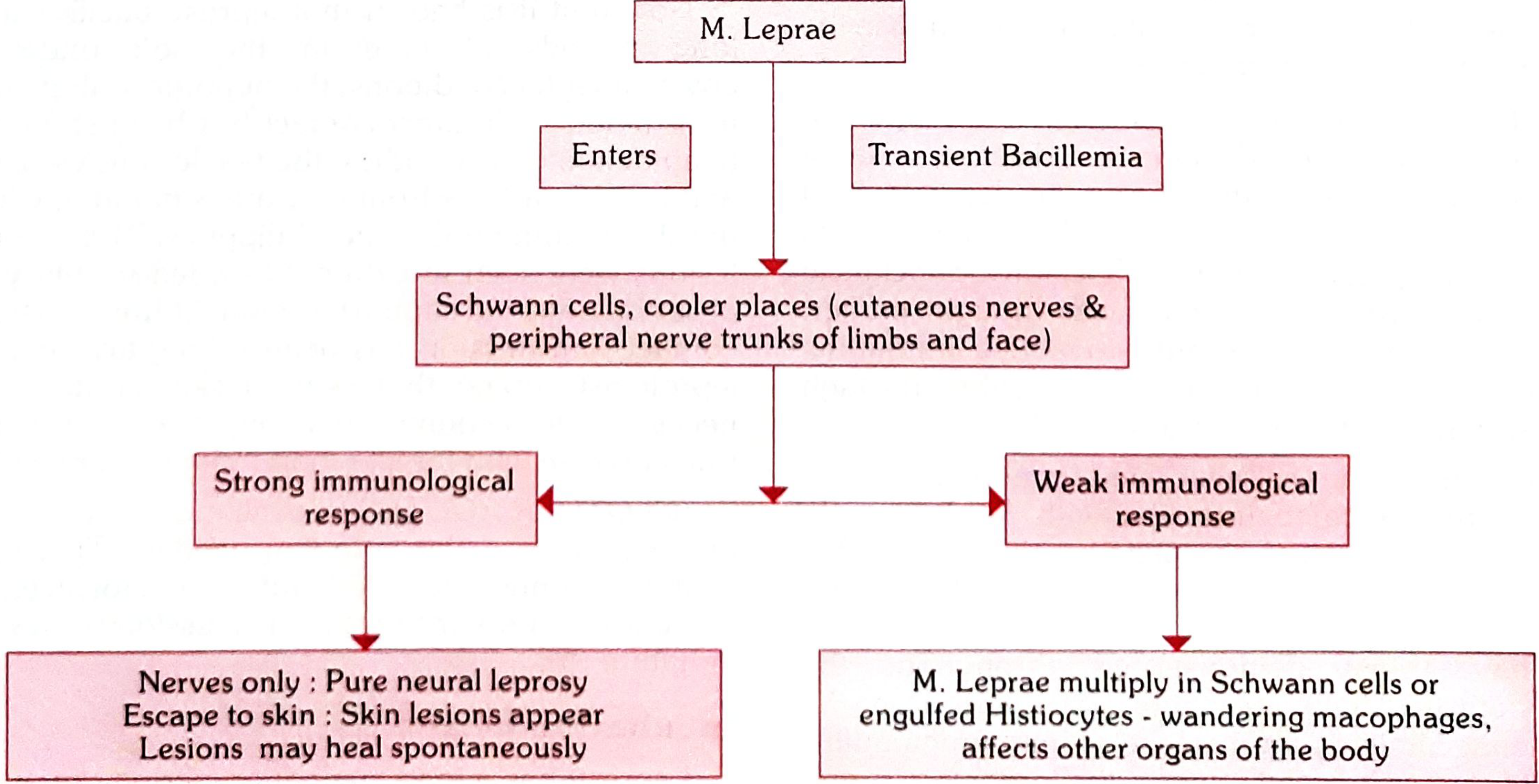
- Park's Textbook of Preventive and Social Medicine, Fig. 1: Pathogenesis of Leprosy
Classification
Ridley-Jopling Classification (Immuno-histological spectrum)
The most important research classification, dividing leprosy into 5 groups on an immunological scale:
| Group | Full Name |
|---|---|
| TT | Tuberculoid |
| BT | Borderline Tuberculoid |
| BB | Mid-Borderline |
| BL | Borderline Lepromatous |
| LL | Lepromatous |
Note: The neuritic (pure neural) type has no skin lesions and does not fit into the Ridley-Jopling scheme - it is recognized in the Indian classification separately.
WHO Classification (for control programs)
| Type | Skin Lesions | Nerve Involvement | Skin Smear |
|---|---|---|---|
| Paucibacillary (PB) | 1-5 lesions | 0-1 nerve | Negative at all sites |
| Multibacillary (MB) | 6 or more | >1 nerve | Positive at any site |
Morphology / Histopathology
Tuberculoid Leprosy (Paucibacillary)
Gross/Clinical:
- Localized flat, red skin lesions that enlarge with irregular shapes
- Indurated, elevated, hyperpigmented margins with depressed pale centers (central healing)
- Skin lesions are anesthetic (loss of sensation)
- Asymmetric involvement of large peripheral nerves
Microscopy:
- Well-formed epithelioid cell granulomas closely resembling tuberculosis (sarcoid-like granulomas)
- Granulomas enclose and destroy small peripheral nerve twigs
- Langhans giant cells may be present
- Bacilli are almost never found (paucibacillary) - reflects strong T-cell immunity
- Nerves show granulomatous destruction → skin anesthesia, muscle atrophy, chronic ulcers
- Facial nerve involvement → paralysis of eyelids → keratitis and corneal ulceration
- Can result in: contractures, paralyses, autoamputation of digits
Note: Most patients die with leprosy rather than of it due to the extremely slow course spanning decades.
Lepromatous Leprosy (Multibacillary)
Organs affected: Skin, peripheral nerves, anterior eye chamber, upper airways (down to larynx), testes, hands, and feet. CNS and vital organs are spared (too warm for M. leprae).
Gross/Clinical:
- Symmetric skin thickening: macular, papular, or nodular lesions on face, ears, wrists, elbows, knees
- Coalescence of nodular lesions → leonine facies (lion-like face)
- Most skin lesions are hyposthetic or anesthetic
- Nasal lesions: persistent inflammation, bacilli-laden discharge
- Symmetric peripheral nerve invasion (ulnar, peroneal nerves)
- Testes destruction → sterility
Microscopy:
- Large aggregates of lipid-laden foamy macrophages called:
- Lepra cells (= Virchow cells / foam cells)
- Filled with masses ("globi") of acid-fast bacilli
- Minimal lymphocytic inflammation around nerves (unlike tuberculoid)
- Lymph nodes: bacteria-filled foamy macrophages in paracortical (T-cell) areas with reactive germinal centers
- Spleen: aggregates in red pulp
- Liver: macrophage aggregates
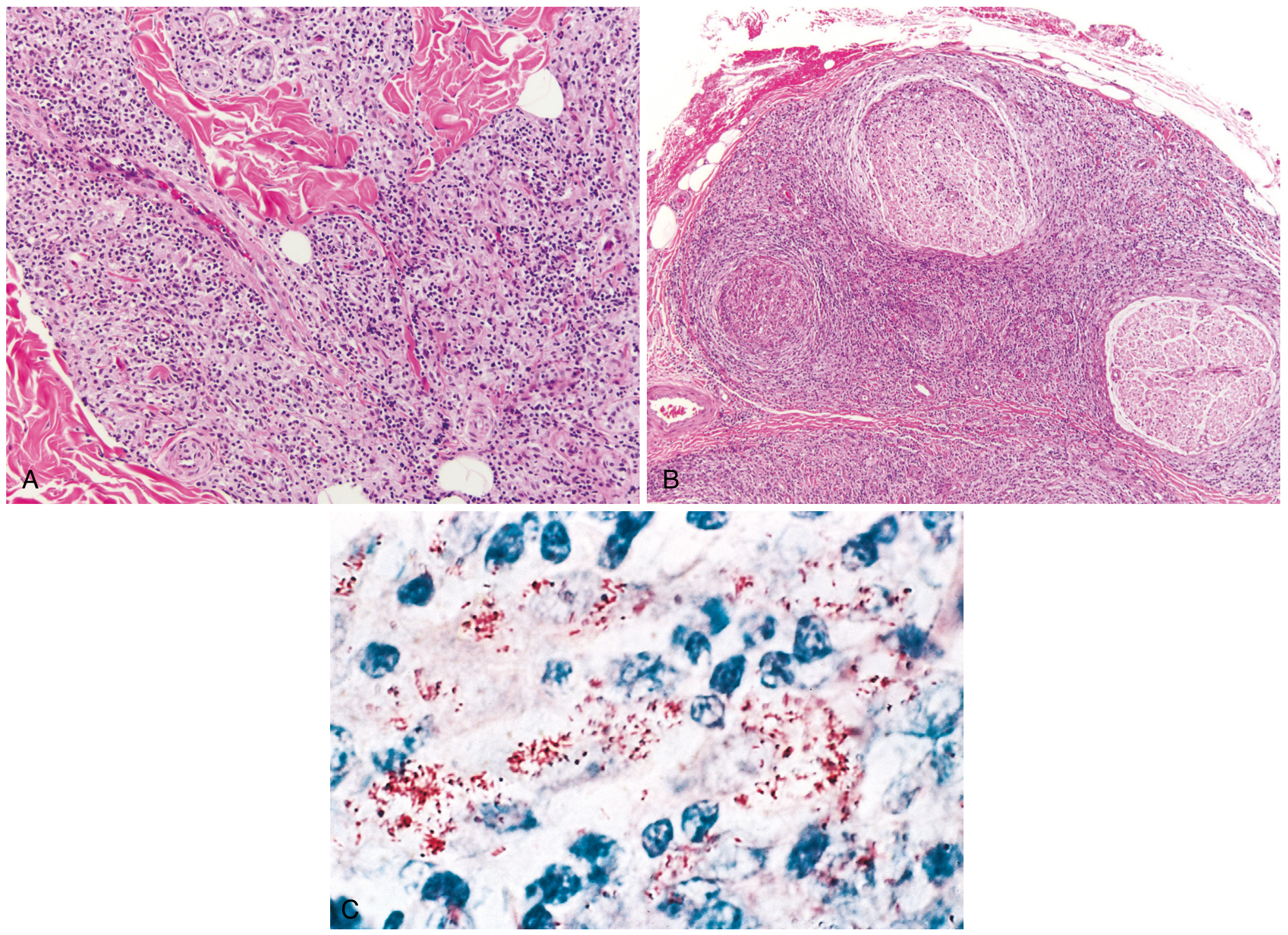
Fig. 8.33 - Robbins, Cotran & Kumar: (A) Dense dermal macrophage infiltration surrounding adnexa, vessels, and nerves in tuberculoid leprosy; (B) Dense lymphocytic and macrophage infiltration into large nerve bundles in lepromatous leprosy; (C) Acid-fast bacilli within macrophages (lepromatous form)
Comparative Summary Table
| Feature | Tuberculoid (TT) | Lepromatous (LL) |
|---|---|---|
| Skin lesions | Few, well-defined, anesthetic | Many, symmetric, hyposthetic |
| Nerve involvement | Asymmetric, early, severe | Symmetric, late |
| Bacillary load | Paucibacillary | Multibacillary |
| Lepromin test | Positive | Negative |
| Histology | Epithelioid granulomas, no bacilli | Lepra/Virchow cells, globi, abundant bacilli |
| Immune response | Strong Th1/CMI | Weak CMI, strong Th2 |
| Leonine facies | Absent | Present |
| Sterility | No | Yes (testicular involvement) |
| Immune complexes / ENL | Rare | Common |
Lepra Reactions
Two types of acute inflammatory episodes can occur:
- Type 1 (Reversal reaction): Occurs in borderline leprosy (BT, BB, BL); upgrading reaction due to sudden increase in cell-mediated immunity; existing lesions become inflamed
- Type 2 - Erythema Nodosum Leprosum (ENL): Occurs in LL/BL; immune complex-mediated (Type III hypersensitivity); painful erythematous nodules, fever, systemic inflammation; can cause vasculitis and glomerulonephritis
Key Staining
- Ziehl-Neelsen (ZN) / Wade-Fite stain: Demonstrates acid-fast bacilli in lepromatous leprosy
- In tuberculoid leprosy, bacilli are not demonstrable on staining
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease | Park's Textbook of Preventive and Social Medicine | Andrews' Diseases of the Skin | Harrison's Principles of Internal Medicine 22e
Classification and immuno pathology of leprosy according to Harsh Mohan textbook of pathology
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
I now have everything needed for a thorough, well-illustrated answer. Let me compile this.
Note: Harsh Mohan's Textbook of Pathology is not in this library's collection. The content below is drawn from Robbins, Cotran & Kumar Pathologic Basis of Disease, Harrison's Principles of Internal Medicine 22e, Goldman-Cecil Medicine, and Dermatology 5e - all of which carry the same pathological concepts that Harsh Mohan covers on this topic. The immunopathology of leprosy is a well-established framework consistent across all major pathology textbooks.
Classification and Immunopathology of Leprosy
Overview: The Immunological Spectrum Concept
The entire classification of leprosy is based on the host's cell-mediated immune (CMI) response to Mycobacterium leprae. This is the foundational concept - leprosy is not just one disease but a spectrum of diseases, with the type of disease a patient develops being determined by their immunological resistance.
"The histopathologic changes in nerve and skin - and thus the type of leprosy that develops - depend on the immunologic resistance of the person infected, in particular on the cell-mediated immune response to the bacillus and its antigens."
- Harrison's Principles of Internal Medicine 22e
A. Classifications of Leprosy
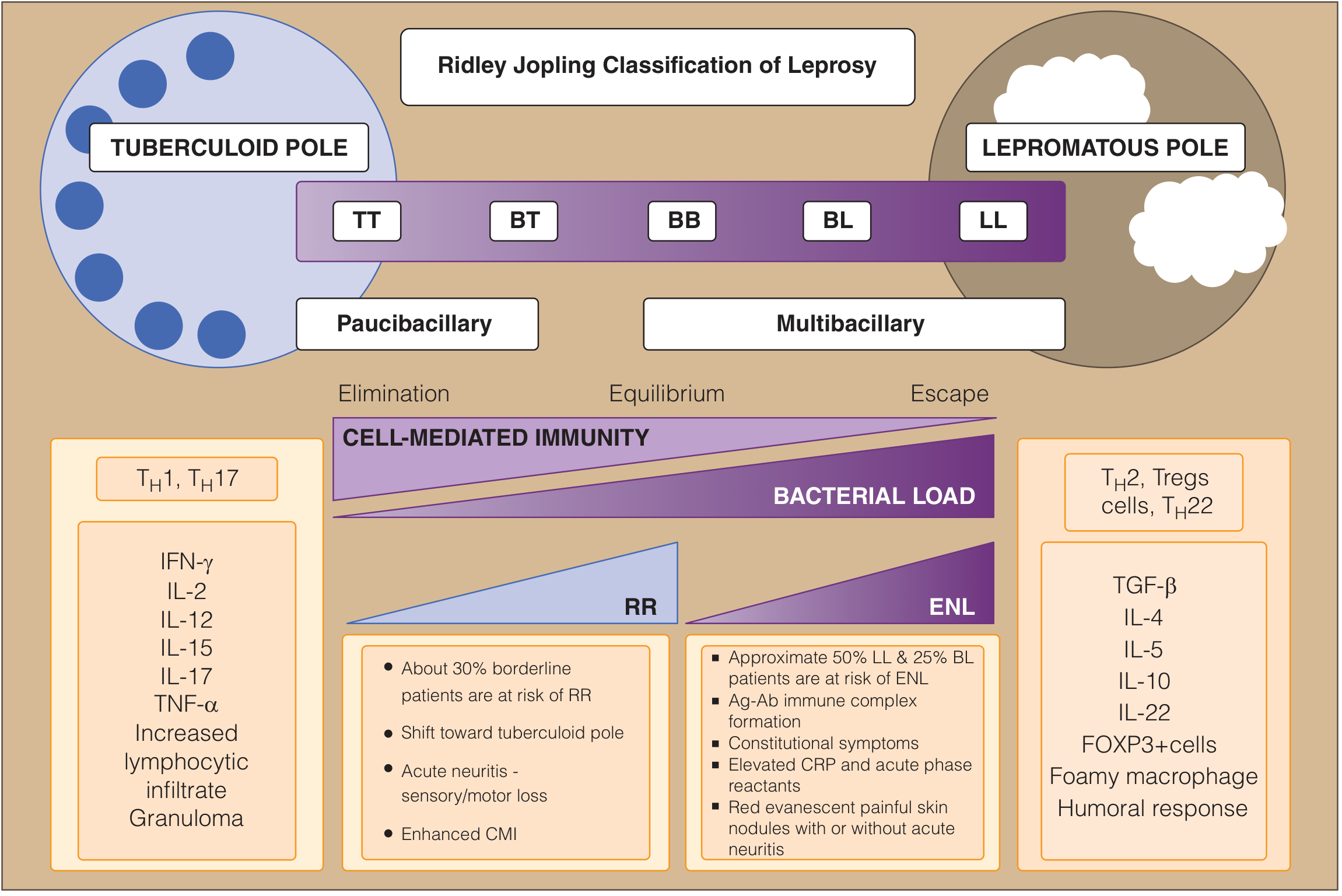
1. Ridley-Jopling Classification (1966) - THE STANDARD
The most important immunohistological classification. Divides leprosy into 5 overlapping types on a spectrum from tuberculoid to lepromatous:
| Type | Abbreviation | Position on Spectrum |
|---|---|---|
| Tuberculoid | TT | Tuberculoid pole |
| Borderline Tuberculoid | BT | Near tuberculoid end |
| Mid-Borderline | BB | Centre |
| Borderline Lepromatous | BL | Near lepromatous end |
| Lepromatous | LL | Lepromatous pole |
- An early/pre-classification form is recognized: Indeterminate Leprosy (IL) - the earliest sign, characterized by infiltration by lymphocytes alone, with no granuloma formed yet
- TT and LL are the stable "polar" types - they show little change over time
- BT, BB, BL are unstable - can shift toward either pole, especially if untreated; BB is the most immunologically unstable and short-lived, mostly progressing toward LL if untreated
- The neuritic (pure neural) type - recognized in the Indian classification - has no skin lesions and does not fit into the Ridley-Jopling scheme
E-Fig. 301-1: The bacteriologic, immunologic, and clinical spectrum of leprosy - Goldman-Cecil Medicine
2. Indian Classification (Most used in field programs in India)
| Type |
|---|
| Indeterminate |
| Tuberculoid |
| Borderline |
| Lepromatous |
| Pure Neuritic (unique to Indian classification - no Madrid equivalent) |
3. Madrid Classification
| Type |
|---|
| Indeterminate |
| Tuberculoid (flat; raised) |
| Borderline |
| Lepromatous |
4. WHO Classification (for treatment/field use)
Used when research facilities are unavailable. Based purely on clinical criteria:
| Type | Skin Lesions | Nerve Involvement | Skin Smear |
|---|---|---|---|
| Paucibacillary (PB) | 1-5 lesions | 0-1 nerve | Negative at all sites |
| Multibacillary (MB) | 6 or more | >1 nerve | Positive at any site |
- PB corresponds broadly to: Indeterminate, TT, BT
- MB corresponds broadly to: BB, BL, LL
- Goldman-Cecil Medicine, Table 301-1; Harrison's 22e
B. Immunopathology of Leprosy
This is the core of classification and the key concept for exams.
The Fundamental Principle
The host's CD4+ T helper cell response determines which type of leprosy develops. The entire immunological spectrum pivots on the Th1 vs. Th2 balance:
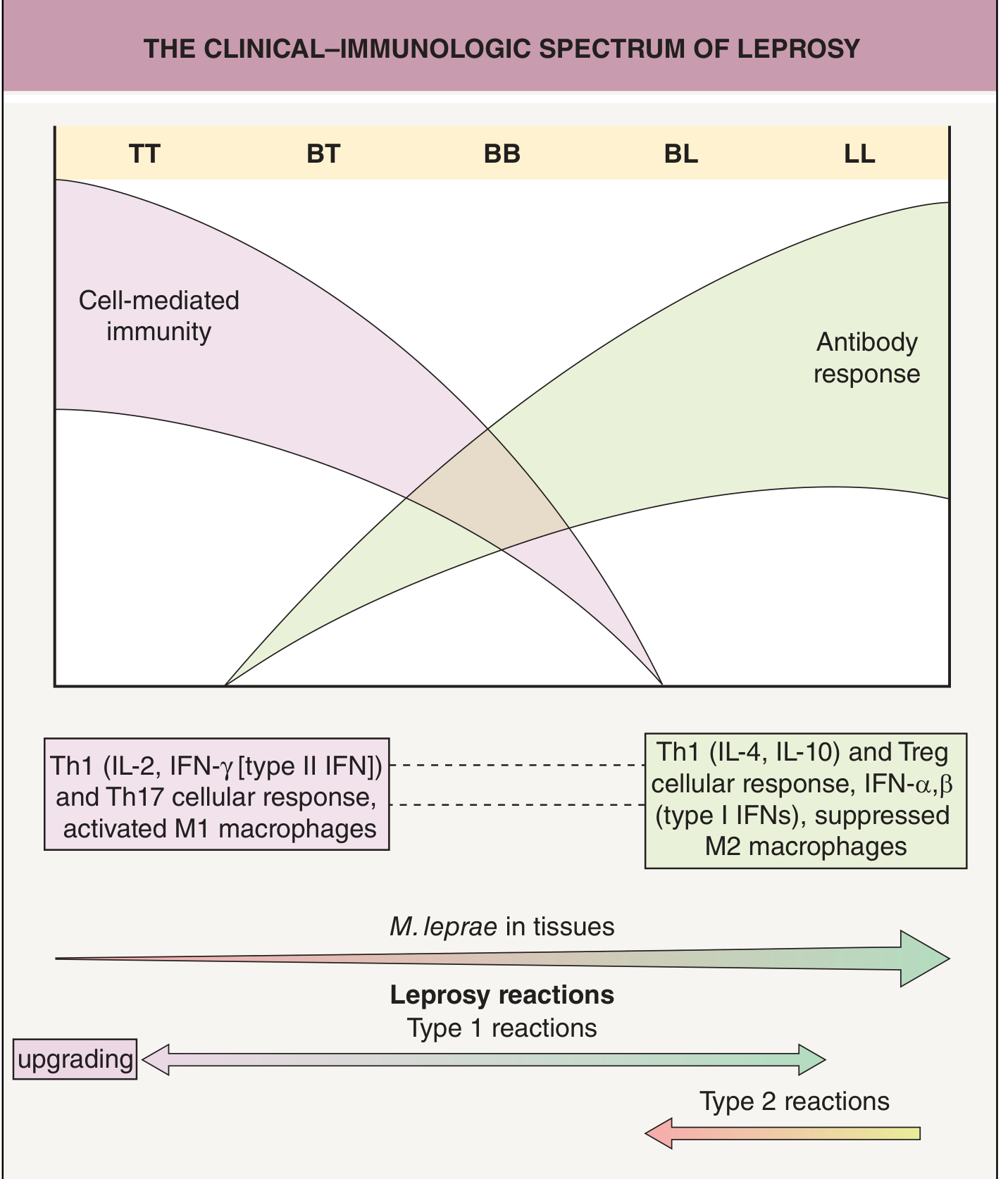
Fig. 75.2 - The clinical-immunologic spectrum of Hansen disease showing how CMI decreases and antibody response increases from TT to LL - Dermatology 5e
Immunopathology at the Tuberculoid Pole (TT)
Immune response: Strong Th1 + Th17
Key cytokines and mediators:
- IL-2, IFN-γ (Type II IFN), IL-12, IL-15, IL-17, TNF-α
- Th17 cellular response
- Activated M1 macrophages (classically activated)
Resulting tissue changes:
- Dendritic cells recognize M. leprae via complement receptor → upregulate MHC class II + CD40L → produce IL-12
- IL-12 drives Th0 → Th1 differentiation
- IFN-γ activates macrophages → transform into epithelioid cells
- Epithelioid cells cluster to form well-organized granulomas with Langhans giant cells
- CD4+ T cells predominate in lesions; CD8+ cytotoxic T cells also participate
- TLR1 and TLR2 are strongly expressed on monocytes/dendritic cells → robust innate response
- Lepromin test: POSITIVE (delayed hypersensitivity reaction at 3-4 weeks = Mitsuda reaction)
- Bacilli are eliminated/controlled → paucibacillary disease
- Antibody production is LOW
Tissue consequence:
- Granulomas destroy peripheral nerve twigs → anesthesia, muscle wasting, trophic ulcers
- High CMI = nerve destruction but low bacterial burden
Immunopathology at the Lepromatous Pole (LL)
Immune response: Weak Th1; dominant Th2 + Regulatory T cells (Tregs) + Th22
Key cytokines and mediators:
- IL-4, IL-5, IL-10, IL-13, IL-22, TGF-β
- Type I IFNs (IFN-α, IFN-β) predominate (instead of type II IFN-γ)
- FOXP3+ regulatory T cells, CD8+ suppressor T cells
- Suppressed M2 macrophages (alternatively activated - foamy phenotype)
Resulting tissue changes:
- Weak Th1 response → macrophages are not effectively activated
- Macrophages engulf bacilli but cannot kill them → bacilli proliferate intracellularly
- Macrophages become lipid-laden foamy macrophages = Lepra cells (Virchow cells)
- Lepra cells are packed with masses of bacilli called "globi"
- TLR1 and TLR2 expression is WEAK → poor innate activation
- M. leprae PGL-1 (cell wall lipid) actively suppresses T-cell responses and IFN-γ production
- M. leprae also inhibits mitochondrial energy metabolism to evade the immune response
- Lepromin test: NEGATIVE (anergy - no CMI to the bacillus)
- Bacilli proliferate unchecked → multibacillary disease
- Antibody production is HIGH but non-protective; antibodies are against PGL-1 antigen
Tissue consequence:
- Minimal inflammation around nerves despite massive bacterial invasion
- Symmetric nerve damage due to direct invasion by bacilli
- Immune complex deposition → Type III hypersensitivity features (vasculitis, glomerulonephritis, ENL)
Immunopathology of Borderline Types
The borderline spectrum represents immunological instability and transition:
| Type | CMI | Bacilli | Granuloma | Nerve damage |
|---|---|---|---|---|
| BT | Moderate-strong CMI | Few | Well-formed but with grenz zone | Significant, asymmetric |
| BB | Equilibrium (unstable) | Moderate | Less organized | Variable |
| BL | Weak CMI | Many | Macrophage granulomas + lymphocytes | Less severe per lesion |
- BT: resembles TT but subepidermal grenz zone present; satellite lesions / pseudopodia; 3-10 lesions
- BB: annular lesions with "Swiss cheese" appearance (punched-out inner edge, ill-defined outer edge); most unstable, mostly progresses to LL if untreated
- BL: numerous copper-hued round/oval macules, symmetrical; moderate bacillary load
Genetic Susceptibility (Immunogenetics)
The immune response is partly genetically determined:
- HLA-DR2 and HLA-DR3 (MHC class II genes) influence which end of the spectrum a patient develops
- Susceptibility to tuberculoid leprosy mapped to chromosome 10p13
- SNPs in TNF-α and IL-10 genes have been identified
- Innate immunity genes: NRAMP1, TLR2, MICA, TNF-α, MRC1
- Adaptive immunity genes: HLA, TAP2, VDR, PTPN22
Nerve Damage Mechanism
M. leprae has the unique ability to invade peripheral nerves - a pathognomonic feature:
- Binds to G domain of laminin alpha-2 chain on the Schwann cell-axon surface via a 21-kDa histone-like protein
- Invasion of Schwann cells and axons → demyelination + axonal degeneration
- In TT: nerve destruction by granuloma (immune-mediated)
- In LL: nerve destruction by direct bacillary invasion with minimal inflammation
- Goldman-Cecil Medicine, p. 3273-3274 | Harrison's Principles of Internal Medicine 22e, p. 2329-2335 | Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 356-357 | Dermatology 5e
Summary Comparison Table
| Feature | Tuberculoid (TT) | Lepromatous (LL) |
|---|---|---|
| T-helper response | Th1 + Th17 | Th2 + Treg + Th22 |
| Key cytokines | IFN-γ, IL-2, IL-12, TNF-α | IL-4, IL-10, TGF-β, IL-22 |
| Macrophage type | M1 (activated, epithelioid) | M2 (foamy, suppressed) |
| Granuloma | Well-formed epithelioid | Absent / diffuse foamy macrophages (leproma) |
| Bacillary load | Paucibacillary | Multibacillary |
| Lepromin test | Positive | Negative |
| Antibody levels | Low | High (non-protective) |
| TLR1/TLR2 | Strong expression | Weak expression |
| Lepra reactions | RR (Type 1) | ENL (Type 2) |
| Disease stability | Stable | Stable |
| Nerve damage mechanism | Granuloma-mediated | Direct bacillary invasion |
This is a shared conversation. Sign in to Orris to start your own chat.