explain meningitis pathology from robbins pathology book
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything needed to provide a comprehensive answer. Here is the full meningitis pathology from Robbins:
Meningitis — Robbins Pathology
Sources: Robbins & Kumar Basic Pathology (9780323790185) and Robbins, Cotran & Kumar Pathologic Basis of Disease (9780443264528)
Definition
Meningitis is an inflammatory process involving the leptomeninges and the CSF within the subarachnoid space, typically caused by infection. When the inflammation extends into the underlying brain parenchyma, it is termed meningoencephalitis. The term is also applied to non-infectious settings:
- Chemical meningitis — response to irritants (e.g., debris from a ruptured epidermoid cyst)
- Carcinomatous meningitis — spread of metastatic cancer cells to the subarachnoid space
- Autoimmune meningitis — seen with systemic autoimmune disease
Classification
Infectious meningitis is classified into three subtypes based on etiology and clinical evolution:
| Type | Usual Cause | CSF Pattern |
|---|---|---|
| Acute Pyogenic | Bacterial | Neutrophilic pleocytosis, ↑↑ protein, ↓↓ glucose |
| Aseptic (Viral) | Viral (enteroviruses most common) | Lymphocytic pleocytosis, ↑ protein (moderate), normal glucose |
| Chronic | TB, spirochetes, fungi | Mixed cellularity, ↑ protein, ↓ or normal glucose |
1. Acute Pyogenic (Bacterial) Meningitis
Causative Organisms by Age
| Age Group | Common Organisms |
|---|---|
| Neonates | Escherichia coli, Group B Streptococci |
| Adolescents/Young Adults | Neisseria meningitidis |
| Elderly | Streptococcus pneumoniae, Listeria monocytogenes |
- Haemophilus influenzae was previously a major cause in infants but immunization has dramatically reduced its incidence.
- In immunosuppressed patients, organisms such as Klebsiella or anaerobes may be causative with atypical clinical presentations.
Clinical Features
- Systemic signs of infection (fever, malaise)
- Meningeal irritation: headache, photophobia, neck stiffness
- Neurologic impairment: irritability, clouding of consciousness
CSF Findings
- Increased pressure; cloudy or frankly purulent
- Abundant neutrophils
- Elevated protein
- Markedly reduced glucose
Morphology (Gross and Microscopic)
Gross:
- Exudate evident within the leptomeninges on the brain surface
- Meningeal vessels are engorged and prominent
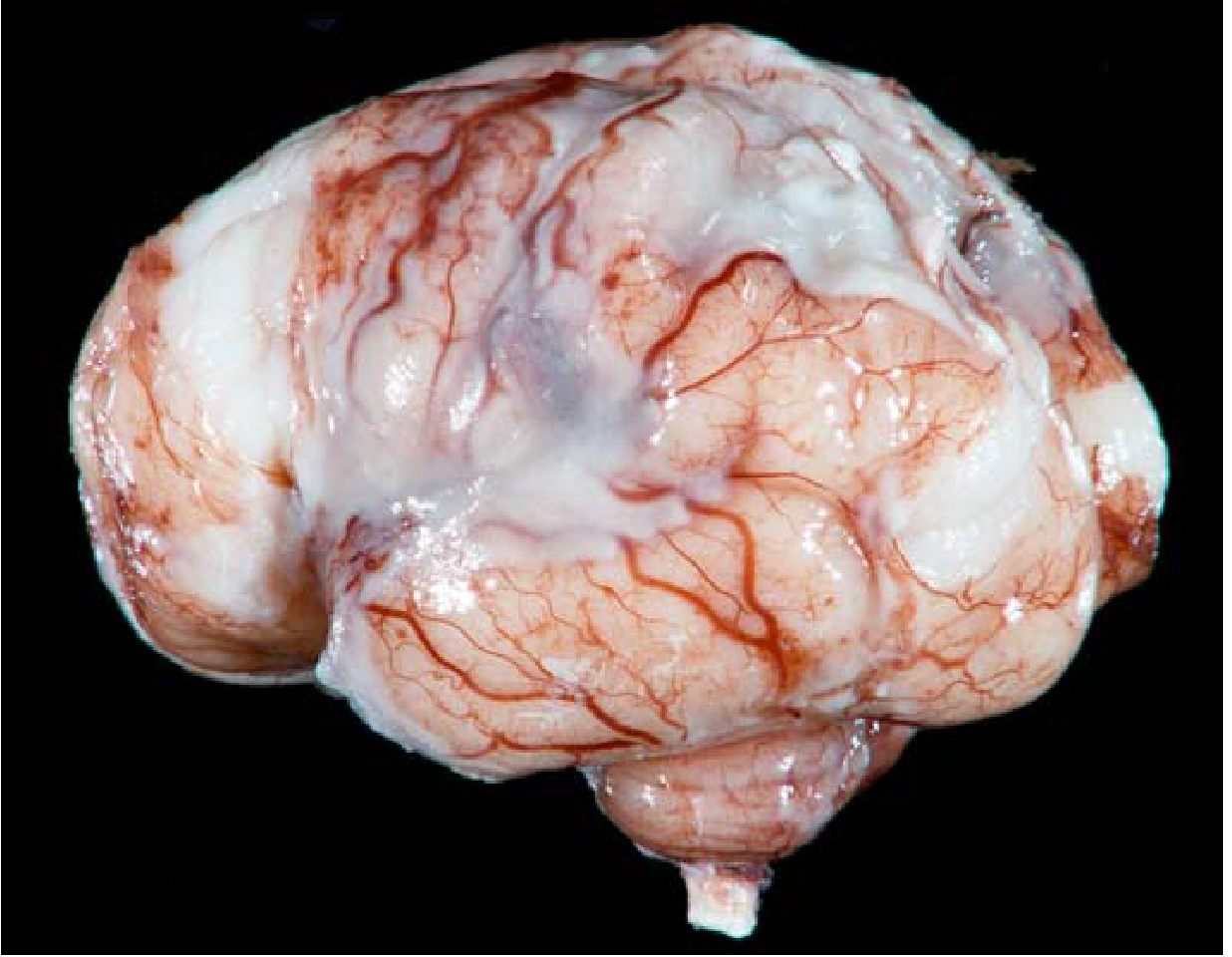
- Tracts of pus extend along blood vessels; distribution varies by organism (H. influenzae → basal; pneumococcal → over cerebral convexities near the sagittal sinus)
- In fulminant cases, inflammation extends to the ventricles (ventriculitis); the choroid plexus lacks a blood-brain barrier and may serve as a portal of entry
Microscopic:
- Neutrophils fill the subarachnoid space in severe cases; in milder cases they surround leptomeningeal blood vessels
- Gram stain reveals bacteria, particularly in untreated cases
- In fulminant meningitis: inflammatory cells infiltrate leptomeningeal vein walls and extend focally into the brain parenchyma (cerebritis); secondary vasculitis and venous thrombosis → hemorrhagic cerebral infarction
Sequelae:
- Leptomeningeal fibrosis → hydrocephalus (more common with TB meningitis, but occurs in bacterial meningitis too)
- In pneumococcal meningitis specifically: large quantities of capsular polysaccharide produce a gelatinous exudate → chronic adhesive arachnoiditis (arachnoid fibrosis)
- Waterhouse-Friderichsen syndrome: meningitis-associated septicemia with hemorrhagic infarction of the adrenal glands — most often with meningococcal and pneumococcal infection
2. Aseptic (Viral) Meningitis
Key Features
- A clinical term for meningitis manifestations (meningeal irritation, fever, altered consciousness) without organisms identifiable by bacterial culture
- Generally viral in etiology; may be rickettsial or autoimmune
- Enteroviruses account for ~80% of identified cases
- Usually self-limited; treated symptomatically
CSF Findings
- Lymphocytic pleocytosis
- Moderate protein elevation
- Normal glucose (key distinction from bacterial meningitis)
Morphology
- Less dramatic than bacterial meningitis
- Leptomeningeal infiltration by lymphocytes and monocytes rather than neutrophils
- No suppurative exudate
3. Chronic Meningitis
Caused by mycobacteria, some spirochetes, and fungi; these infections often involve the brain parenchyma as well.
A. Tuberculous Meningitis
- Symptoms: headache, malaise, mental confusion, vomiting
- CSF: moderate ↑ cellularity (mononuclear or mixed), ↑↑ protein, moderately ↓ or normal glucose
- Tuberculoma: well-circumscribed intraparenchymal mass of M. tuberculosis; may coexist with meningitis
- Complication: chronic tuberculous meningitis → arachnoid fibrosis (particularly at the base of the brain) → hydrocephalus from impaired CSF resorption
B. Spirochetal Infections (Neurosyphilis)
- Occurs in ~10% of untreated Treponema pallidum infection (tertiary syphilis); more aggressive with HIV co-infection
- Patterns of CNS involvement:
- Meningovascular neurosyphilis: chronic meningitis (usually basal), associated with obliterative endarteritis of meningeal/cortical vessels → strokes
- Paretic neurosyphilis (general paresis): progressive dementia from direct parenchymal invasion
- Tabes dorsalis: degeneration of posterior spinal columns and dorsal nerve roots
- Lyme Neuroborreliosis (Borrelia burgdorferi): can cause meningitis, cranial nerve palsies, and radiculopathy
C. Fungal Meningitis
- Cryptococcus neoformans: most important fungal cause of meningitis, especially in HIV/immunocompromised patients
- Produces a gelatinous meningitis as the organisms fill the subarachnoid space
- Characteristic "soap-bubble" lesions in basal ganglia/cortex (pseudocysts of cryptococcal organisms)
Summary of CSF Interpretation
| Parameter | Bacterial | Viral | Tuberculous/Fungal |
|---|---|---|---|
| Appearance | Turbid/purulent | Clear | Clear/viscous |
| Cells | Neutrophils ↑↑ | Lymphocytes ↑ | Lymphocytes/mixed ↑ |
| Protein | ↑↑ | Mildly ↑ | ↑↑ |
| Glucose | ↓↓ | Normal | ↓ or normal |
— Robbins & Kumar Basic Pathology (Robbins Pathology), Chapter 21; Robbins, Cotran & Kumar Pathologic Basis of Disease, Chapter 28
make pdf
Reading File
Running Command
ls -la /home/daytona/workspace/ 2>/dev/null || mkdir -p /home/daytona/workspace
Running Command
mkdir -p /home/daytona/workspace/meningitis-pdf
Writing File
~/meningitis-pdf/generate_pdf.py
from reportlab.lib.pagesizes import A4
from reportlab.lib.styles import getSampleStyleSheet, ParagraphStyle
from reportlab.lib.units import cm
from reportlab.lib import colors
from reportlab.platypus import (
SimpleDocTemplate, Paragraph, Spacer, Table, TableStyle,
HRFlowable, Image, KeepTogether
)
from reportlab.lib.enums import TA_CENTER, TA_LEFT, TA_JUSTIFY
import urllib.request
import os
OUTPUT = "/home/daytona/workspace/meningitis-pdf/Meningitis_Pathology_Robbins.pdf"
# Download brain image
img_url = "https://cdn.orris.care/cdss_images/a1b43e7b5560ad74493828517fb67d7428a26b46f8b47d8fa140658ba8d75a8c.png"
img_path = "/home/daytona/workspace/meningitis-pdf/pyogenic_meningitis.png"
if not os.path.exists(img_path):
urllib.request.urlretrieve(img_url, img_path)
doc = SimpleDocTemplate(
OUTPUT,
pagesize=A4,
rightMargin=2*cm, leftMargin=2*cm,
topMargin=2.5*cm, bottomMargin=2.5*cm
)
styles = getSampleStyleSheet()
# Custom styles
title_style = ParagraphStyle(
'CustomTitle',
parent=styles['Title'],
fontSize=22,
textColor=colors.HexColor('#1a3a5c'),
spaceAfter=6,
alignment=TA_CENTER,
fontName='Helvetica-Bold'
)
subtitle_style = ParagraphStyle(
'Subtitle',
parent=styles['Normal'],
fontSize=10,
textColor=colors.HexColor('#555555'),
alignment=TA_CENTER,
spaceAfter=16
)
h1_style = ParagraphStyle(
'H1',
parent=styles['Heading1'],
fontSize=14,
textColor=colors.white,
fontName='Helvetica-Bold',
spaceAfter=4,
spaceBefore=14,
leftIndent=0,
backColor=colors.HexColor('#1a3a5c'),
borderPad=(4, 6, 4, 6),
)
h2_style = ParagraphStyle(
'H2',
parent=styles['Heading2'],
fontSize=12,
textColor=colors.HexColor('#1a3a5c'),
fontName='Helvetica-Bold',
spaceAfter=4,
spaceBefore=10,
borderPad=0,
)
h3_style = ParagraphStyle(
'H3',
parent=styles['Heading3'],
fontSize=10,
textColor=colors.HexColor('#2c5f8a'),
fontName='Helvetica-BoldOblique',
spaceAfter=3,
spaceBefore=7,
)
body_style = ParagraphStyle(
'Body',
parent=styles['Normal'],
fontSize=10,
leading=15,
spaceAfter=6,
alignment=TA_JUSTIFY,
fontName='Helvetica'
)
caption_style = ParagraphStyle(
'Caption',
parent=styles['Normal'],
fontSize=8.5,
textColor=colors.HexColor('#444444'),
alignment=TA_CENTER,
fontName='Helvetica-Oblique',
spaceAfter=8
)
bullet_style = ParagraphStyle(
'Bullet',
parent=styles['Normal'],
fontSize=10,
leading=14,
leftIndent=16,
spaceAfter=3,
bulletIndent=4,
fontName='Helvetica'
)
def H1(text):
# Draw a colored banner
return Paragraph(f"<font color='white'><b> {text}</b></font>", h1_style)
def H2(text):
return Paragraph(text, h2_style)
def H3(text):
return Paragraph(text, h3_style)
def P(text):
return Paragraph(text, body_style)
def B(text):
return Paragraph(f"• {text}", bullet_style)
def Sp(h=8):
return Spacer(1, h)
def HR():
return HRFlowable(width="100%", thickness=0.5, color=colors.HexColor('#cccccc'), spaceAfter=4, spaceBefore=4)
# ---- TABLE HELPER ----
TABLE_HEADER_BG = colors.HexColor('#1a3a5c')
TABLE_ROW_BG = colors.HexColor('#eaf2fb')
TABLE_ALT_BG = colors.white
def make_table(data, col_widths=None):
n_cols = len(data[0])
if col_widths is None:
w = (A4[0] - 4*cm) / n_cols
col_widths = [w] * n_cols
style = TableStyle([
('BACKGROUND', (0,0), (-1,0), TABLE_HEADER_BG),
('TEXTCOLOR', (0,0), (-1,0), colors.white),
('FONTNAME', (0,0), (-1,0), 'Helvetica-Bold'),
('FONTSIZE', (0,0), (-1,0), 9),
('ALIGN', (0,0), (-1,-1), 'LEFT'),
('VALIGN', (0,0), (-1,-1), 'MIDDLE'),
('ROWBACKGROUNDS', (0,1), (-1,-1), [TABLE_ROW_BG, TABLE_ALT_BG]),
('FONTNAME', (0,1), (-1,-1), 'Helvetica'),
('FONTSIZE', (0,1), (-1,-1), 9),
('GRID', (0,0), (-1,-1), 0.4, colors.HexColor('#aaaaaa')),
('LEFTPADDING',(0,0), (-1,-1), 6),
('RIGHTPADDING',(0,0),(-1,-1), 6),
('TOPPADDING', (0,0), (-1,-1), 4),
('BOTTOMPADDING',(0,0),(-1,-1), 4),
])
formatted_data = []
for i, row in enumerate(data):
formatted_row = []
for cell in row:
fs = 9
fn = 'Helvetica-Bold' if i == 0 else 'Helvetica'
fc = colors.white if i == 0 else colors.black
p = Paragraph(str(cell), ParagraphStyle('tc', fontSize=fs, fontName=fn, textColor=fc, leading=13))
formatted_row.append(p)
formatted_data.append(formatted_row)
return Table(formatted_data, colWidths=col_widths, style=style, repeatRows=1)
# ===================== CONTENT =====================
story = []
# --- Cover ---
story.append(Sp(20))
story.append(Paragraph("Meningitis", title_style))
story.append(Paragraph("Pathology — From Robbins & Kumar", subtitle_style))
story.append(HR())
story.append(Paragraph(
"<i>Sources: Robbins & Kumar Basic Pathology (9th Ed.) | "
"Robbins, Cotran & Kumar Pathologic Basis of Disease</i>",
caption_style
))
story.append(Sp(10))
# --- Definition ---
story.append(H1("1. Definition"))
story.append(Sp(6))
story.append(P(
"<b>Meningitis</b> is an inflammatory process involving the <b>leptomeninges and CSF within the "
"subarachnoid space</b>, typically caused by infection. When inflammation extends into the brain "
"parenchyma, it is termed <b>meningoencephalitis</b>."
))
story.append(P("Non-infectious forms include:"))
story.append(B("<b>Chemical meningitis</b> — response to irritants (e.g., debris from a ruptured epidermoid cyst)"))
story.append(B("<b>Carcinomatous meningitis</b> — metastatic cancer cells spreading to the subarachnoid space"))
story.append(B("<b>Autoimmune meningitis</b> — associated with systemic autoimmune disease"))
story.append(Sp(4))
# --- Classification Table ---
story.append(H1("2. Classification"))
story.append(Sp(6))
story.append(P("Infectious meningitis is classified into three subtypes based on etiology and clinical evolution:"))
story.append(Sp(4))
class_data = [
["Type", "Usual Cause", "CSF Pattern"],
["Acute Pyogenic", "Bacterial", "Neutrophilic pleocytosis, ↑↑ protein, ↓↓ glucose"],
["Aseptic (Viral)", "Enteroviruses (80% of cases)", "Lymphocytic pleocytosis, ↑ protein (moderate), normal glucose"],
["Chronic", "TB, spirochetes, fungi", "Mixed cellularity, ↑ protein, ↓ or normal glucose"],
]
story.append(make_table(class_data, col_widths=[4.5*cm, 5.5*cm, 7.5*cm]))
story.append(Sp(10))
# --- Acute Pyogenic ---
story.append(H1("3. Acute Pyogenic (Bacterial) Meningitis"))
story.append(Sp(6))
story.append(H2("Causative Organisms by Age"))
age_data = [
["Age Group", "Common Organisms"],
["Neonates", "Escherichia coli, Group B Streptococci"],
["Adolescents / Young Adults", "Neisseria meningitidis"],
["Elderly", "Streptococcus pneumoniae, Listeria monocytogenes"],
["Immunosuppressed", "Klebsiella, anaerobes (atypical course)"],
]
story.append(make_table(age_data, col_widths=[6*cm, 11.5*cm]))
story.append(Sp(6))
story.append(P(
"Note: <i>Haemophilus influenzae</i> was formerly a major cause in infants; widespread immunization "
"has dramatically reduced its incidence."
))
story.append(H2("Clinical Features"))
story.append(B("Systemic: fever, malaise"))
story.append(B("Meningeal irritation: headache, photophobia, neck stiffness"))
story.append(B("Neurologic: irritability, clouding of consciousness"))
story.append(Sp(4))
story.append(H2("CSF Findings"))
csf_data = [
["Parameter", "Bacterial"],
["Appearance", "Turbid / frankly purulent"],
["Cells", "Neutrophils ↑↑"],
["Protein", "Elevated ↑↑"],
["Glucose", "Markedly reduced ↓↓"],
["Pressure", "Increased"],
]
story.append(make_table(csf_data, col_widths=[6*cm, 11.5*cm]))
story.append(Sp(8))
story.append(H2("Morphology"))
story.append(H3("Gross Pathology"))
story.append(B("<b>Exudate</b> within leptomeninges on brain surface; meningeal vessels engorged and prominent"))
story.append(B("<b>Tracts of pus</b> extend along blood vessels"))
story.append(B("Distribution varies: <i>H. influenzae</i> → basal; pneumococcal → cerebral convexities near sagittal sinus"))
story.append(B("Fulminant cases: inflammation extends to ventricles (<b>ventriculitis</b>); choroid plexus acts as portal of entry"))
story.append(Sp(4))
story.append(H3("Microscopic Pathology"))
story.append(B("<b>Neutrophils fill the subarachnoid space</b> (severe) or surround leptomeningeal vessels (mild)"))
story.append(B("<b>Gram stain</b> reveals bacteria, especially in untreated cases"))
story.append(B("Fulminant: inflammatory cells infiltrate leptomeningeal vein walls → extend into brain parenchyma (<b>cerebritis</b>)"))
story.append(B("Secondary <b>vasculitis</b> and <b>venous thrombosis</b> → <b>hemorrhagic cerebral infarction</b>"))
story.append(Sp(6))
# Brain image
try:
img = Image(img_path, width=12*cm, height=8*cm, kind='proportional')
img.hAlign = 'CENTER'
story.append(KeepTogether([
img,
Paragraph(
"<i>Fig. 21.16 / Fig. 28.23 — Pyogenic meningitis. A thick layer of suppurative exudate covers "
"the brain surface and thickens the leptomeninges. (Robbins Pathology)</i>",
caption_style
)
]))
except Exception as e:
story.append(P(f"[Image not available: {e}]"))
story.append(Sp(6))
story.append(H3("Sequelae"))
story.append(B("<b>Leptomeningeal fibrosis</b> → <b>hydrocephalus</b>"))
story.append(B("Pneumococcal meningitis: capsular polysaccharide → gelatinous exudate → <b>chronic adhesive arachnoiditis</b>"))
story.append(B("<b>Waterhouse-Friderichsen syndrome</b>: septicemia + hemorrhagic infarction of adrenal glands (meningococcal/pneumococcal)"))
story.append(Sp(8))
# --- Aseptic Viral ---
story.append(H1("4. Aseptic (Viral) Meningitis"))
story.append(Sp(6))
story.append(P(
"Aseptic meningitis is a <b>clinical term</b> for meningitis manifestations (meningeal irritation, "
"fever, altered consciousness) <b>without organisms identifiable by bacterial culture</b>. "
"It is generally viral in etiology; may be rickettsial or autoimmune. "
"<b>Enteroviruses</b> account for ~<b>80%</b> of identified cases. Usually self-limited."
))
story.append(H2("CSF Findings"))
vcsf_data = [
["Parameter", "Viral (Aseptic)"],
["Cells", "Lymphocytic pleocytosis"],
["Protein", "Moderately elevated"],
["Glucose", "Normal (key distinguishing feature)"],
]
story.append(make_table(vcsf_data, col_widths=[6*cm, 11.5*cm]))
story.append(Sp(4))
story.append(H2("Morphology"))
story.append(B("Leptomeningeal infiltration by <b>lymphocytes and monocytes</b> (not neutrophils)"))
story.append(B("No suppurative exudate"))
story.append(B("Less dramatic changes than bacterial meningitis"))
story.append(Sp(8))
# --- Chronic Meningitis ---
story.append(H1("5. Chronic Meningitis"))
story.append(Sp(6))
story.append(P(
"Caused by <b>mycobacteria, spirochetes, and fungi</b>. These infections often also involve "
"the brain parenchyma."
))
story.append(H2("A. Tuberculous Meningitis"))
story.append(B("Symptoms: headache, malaise, mental confusion, vomiting"))
story.append(B("CSF: moderate ↑ cellularity (mononuclear or mixed), ↑↑ protein, ↓ or normal glucose"))
story.append(B("<b>Tuberculoma</b>: well-circumscribed intraparenchymal mass; may coexist with meningitis"))
story.append(B("Complication: <b>arachnoid fibrosis</b> at base of brain → <b>hydrocephalus</b> (impaired CSF resorption)"))
story.append(Sp(6))
story.append(H2("B. Spirochetal Infections (Neurosyphilis)"))
story.append(P(
"Occurs in ~10% of untreated <i>Treponema pallidum</i> infection (tertiary syphilis). "
"HIV co-infection increases risk and aggressiveness."
))
syphilis_data = [
["Pattern", "Description"],
["Meningovascular neurosyphilis", "Chronic meningitis (basal) + obliterative endarteritis → strokes"],
["Paretic neurosyphilis (General paresis)", "Progressive dementia from direct parenchymal invasion"],
["Tabes dorsalis", "Degeneration of posterior spinal columns and dorsal nerve roots"],
["Lyme neuroborreliosis (B. burgdorferi)", "Meningitis, cranial nerve palsies, radiculopathy"],
]
story.append(make_table(syphilis_data, col_widths=[6.5*cm, 11*cm]))
story.append(Sp(6))
story.append(H2("C. Fungal Meningitis"))
story.append(B("<b>Cryptococcus neoformans</b>: most important fungal cause; especially in HIV/immunocompromised"))
story.append(B("Produces <b>gelatinous meningitis</b> as organisms fill the subarachnoid space"))
story.append(B("Characteristic <b>'soap-bubble' lesions</b> (pseudocysts) in basal ganglia/cortex"))
story.append(Sp(8))
# --- CSF Comparison Table ---
story.append(H1("6. CSF Summary — Comparison Table"))
story.append(Sp(6))
csf_comp = [
["Parameter", "Bacterial", "Viral", "TB / Fungal"],
["Appearance", "Turbid/purulent", "Clear", "Clear/viscous"],
["Predominant cells", "Neutrophils ↑↑", "Lymphocytes ↑", "Lymphocytes/mixed ↑"],
["Protein", "↑↑", "Mildly ↑", "↑↑"],
["Glucose", "↓↓", "Normal", "↓ or normal"],
]
story.append(make_table(csf_comp, col_widths=[4.5*cm, 4.5*cm, 4.5*cm, 4*cm]))
story.append(Sp(10))
# Footer note
story.append(HR())
story.append(Paragraph(
"<i>Robbins & Kumar Basic Pathology (Robbins Pathology), Chapter 21 | "
"Robbins, Cotran & Kumar Pathologic Basis of Disease, Chapter 28</i>",
caption_style
))
# Build
doc.build(story)
print("PDF generated successfully:", OUTPUT)
Running Command
python /home/daytona/workspace/meningitis-pdf/generate_pdf.py
PDF generated successfully. Here's your download link:
Meningitis Pathology Robbins
PDF Document · PDF
The PDF includes:
- Definition & classification table
- Acute Pyogenic Meningitis — organisms by age, clinical features, CSF findings, gross & microscopic morphology, sequelae
- Gross pathology image from Robbins (Fig. 21.16)
- Aseptic (Viral) Meningitis section
- Chronic Meningitis — TB, neurosyphilis (with pattern table), and cryptococcal
- Full CSF comparison table across all three types
- Sourced from both Robbins editions throughout
This is a shared conversation. Sign in to Orris to start your own chat.