Priapism
Reading File
Finding Sources
Searching PubMed
priapism management treatment
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
I now have all I need for a comprehensive answer. Here is a full clinical overview of priapism:
Priapism
Priapism is a prolonged, persistent penile erection unrelated to sexual stimulation, conventionally defined as lasting >4 hours. It is one of the most common urologic emergencies. The condition was named after Priapus, the ancient Greek god of fertility, who was depicted with permanently oversized genitalia.
Classification
There are three distinct types, each with different pathophysiology, urgency, and management:
| Type | Flow | Pain | Cause | Urgency |
|---|---|---|---|---|
| Ischemic (low-flow, veno-occlusive) | Low/absent | Painful, rigid | Venous outflow obstruction | Emergency |
| Nonischemic (high-flow, arterial) | Increased, unregulated | Usually painless | Arteriocavernous fistula post-trauma | Non-urgent |
| Stuttering (recurrent ischemic) | Variable | Painful episodes | Recurrent veno-occlusion | Elective/preventive |
1. Ischemic (Low-Flow) Priapism
The most common type. Incidence: up to 5.34 per 100,000 men/year.
Pathophysiology
- Venous outflow from the corpora cavernosa is obstructed
- Stagnant blood becomes hypoxic, hypercapnic, and acidotic
- A cascade of endothelial and smooth-muscle damage leads to progressive fibrosis
- Conceptually analogous to compartment syndrome of the penis
- Cavernosal blood gas: ↓PO₂, ↑PCO₂, ↓pH
Causes
Hematologic:
- Sickle cell disease (most common in children; occurs in 2–29% of affected males — sickled RBCs occlude sinusoids during sleep-related mild hypoventilatory acidosis)
- Leukemia, other hemoglobinopathies, G6PD deficiency
Medications (intracavernous or systemic):
- Intracavernous vasoactive agents: papaverine, phentolamine, prostaglandin E1 (alprostadil)
- Antipsychotics (especially chlorpromazine, trazodone)
- Anticoagulants, antihypertensives
- PDE5 inhibitors (rare)
Other:
- Spinal cord injury
- Pelvic/perineal malignancy
- Cocaine use (underreported)
- Idiopathic (most common overall)
⚠️ Pseudopriapism (non-deflating penile prosthesis or malignant corporal replacement in prostate/bladder cancer) must be distinguished from true priapism.
2. Nonischemic (High-Flow) Priapism
Pathophysiology
- Typically follows trauma to the perineum or penis
- Injury to the cavernosal or helicine artery → arteriocavernous fistula
- Unregulated arterial inflow causes partial, painless tumescence
- Venous drainage is preserved → no ischemia
- This is not a medical emergency
3. Stuttering (Recurrent) Priapism
- Periodic painful erections of shorter duration with spontaneous detumescence
- Most common in sickle cell disease patients
- Involves dysregulation of PDE5, nitric oxide (NO), and cGMP signaling
- Episodes often occur during sleep
Evaluation
History
- Duration and onset, pain, prior episodes
- Medications, drug use (cocaine), sickle cell history
- Prior trauma (points toward nonischemic)
Physical Examination
- Ischemic: fully rigid, tender corpora; soft glans
- Nonischemic: partial tumescence, soft/non-tender corpora, often palpable perineal bruit
Investigations
- Corporal blood gas (or color Doppler ultrasound): key diagnostic test
- Low-flow: pO₂ <30 mmHg, pCO₂ >60 mmHg, pH <7.25
- High-flow: blood gas resembles arterial values
- CBC/blood film: sickle cell, leukemia
- Color Doppler ultrasound: identifies arteriovenous fistula in nonischemic type
- CT angiography: locates the damaged vessel in nonischemic priapism
Management
Ischemic Priapism — Step-up Approach
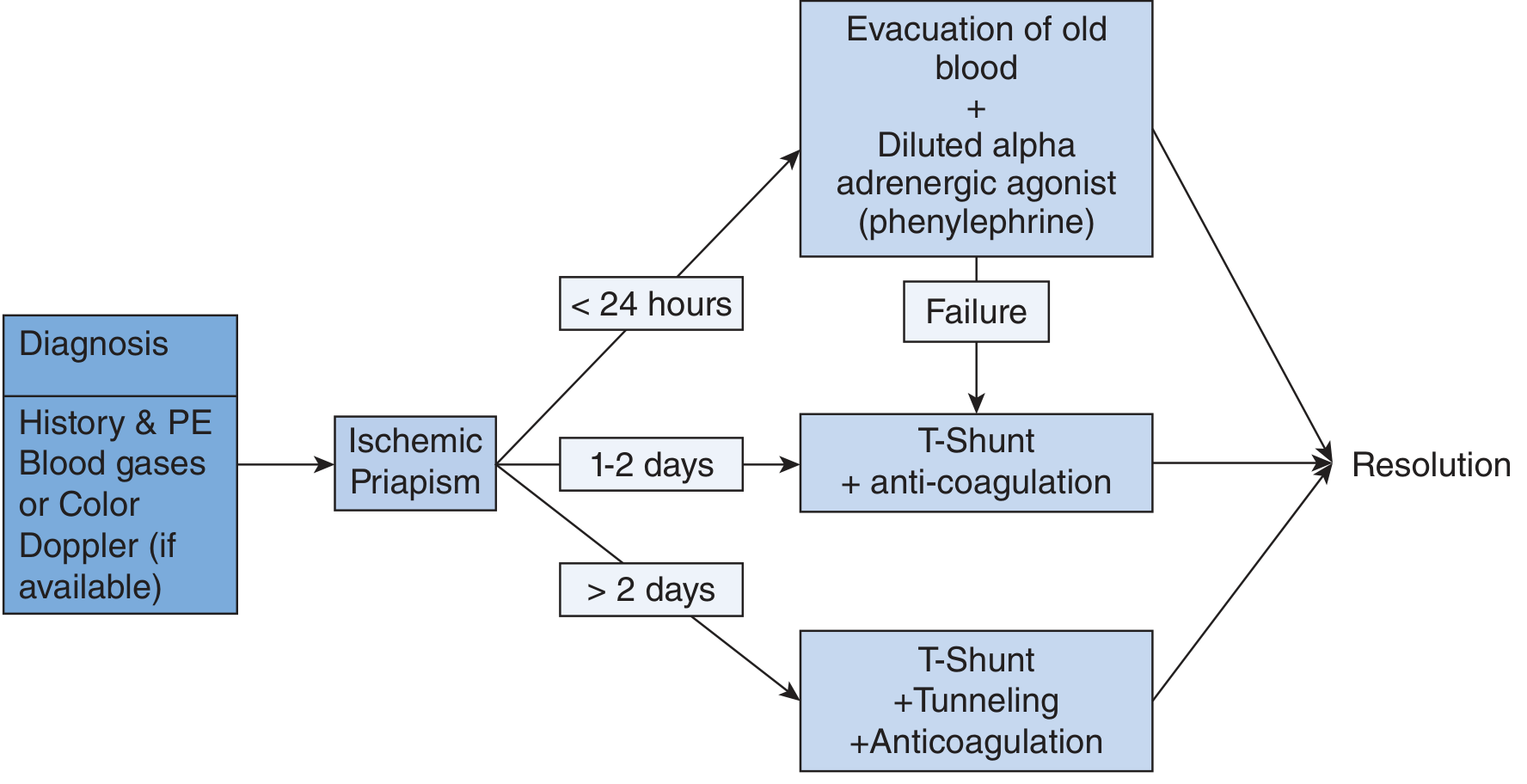
Management of ischemic priapism — Roberts & Hedges' / Smith & Tanagho's
Step 1 — Conservative (optional initial trial):
- Subcutaneous or oral terbutaline 0.25–0.5 mg SQ (repeat in 15 min) or 5 mg PO
- Less effective than direct injection but may be tried first
Step 2 — Intracavernous injection (preferred first-line invasive):
- Phenylephrine 200–500 μg every 5–20 min (up to 3 doses) — drug of choice due to selective α1 activity without cardiac β effects
- Inject at 10 o'clock or 2 o'clock position at base of penis (25–27 gauge needle), avoiding the dorsal neurovascular bundle
- Because the corpora communicate, unilateral injection suffices
| Agent | Dose | Preparation |
|---|---|---|
| Phenylephrine | 0.2–0.5 mg | Dilute to 1 mL final volume in NS |
| Epinephrine (1:1000) | 0.1 mg (0.1 mL) | Dilute with 0.9 mL NS |
Step 3 — Corporal aspiration ± irrigation (if injection alone fails):
- Aspirate 20–30 mL of dark corporal blood (using 21-gauge butterfly)
- Irrigate with saline or dilute phenylephrine
- Visible change from dark venous to bright arterial blood = success
Step 4 — Surgical shunting (if medical treatment fails):
Escalate from least to most invasive:
| Shunt Type | Procedure | Access |
|---|---|---|
| Distal (preferred) | Winter shunt, Ebbehoj shunt, T-shunt | Percutaneous (glans-to-corpus) |
| Al-Ghorab shunt | Open distal | |
| Proximal | Quackels shunt | Corpus-to-spongiosum |
| Barry shunt | Corpus-to-vein | |
| Tunneling | Lue, Burnett (for >48 h) | Extends shunt tract |
- For duration 1–2 days: T-shunt + anticoagulation
- For duration >2 days: T-shunt + tunneling + anticoagulation
- Perioperative anticoagulation: heparin 5000 units SQ + aspirin 325 mg immediately; continue aspirin 325 mg + clopidogrel 75 mg PO daily for ≥5 days postoperatively (reduces shunt closure)
Step 5 — Early penile prosthesis implantation:
- Considered when ischemia has lasted >48 hours and shunting fails
- Implantation within 4 weeks yields fewer complications (erosion, infection, shortening) vs. delayed implantation
- Malleable prosthesis allows later upsizing to inflatable device
Nonischemic Priapism — Conservative to Selective
- Observation + compression: may resolve spontaneously
- Androgen ablation (1–3 months): reduces sleep erections, allows vascular injury to heal
- Selective arterial embolization: autologous clot, gel foam, or coiling — preferred over surgery
- Surgery: last resort
Stuttering Priapism — Prevention
- Oral pseudoephedrine or other α-agonists at bedtime
- PDE5 inhibitors (long-term, low-dose): paradoxically prevent recurrence by restoring normal PDE5/cGMP homeostasis (Burnett hypothesis)
- Sickle cell–directed: hydration, oxygenation, alkalization, analgesia, exchange transfusion to reduce HbS concentration
- Home self-injection kits for patients with frequent recurrences
Complications
- Erectile dysfunction: >1/3 of patients with severe priapism develop permanent ED despite treatment — risk increases with duration
- Penile fibrosis: irreversible smooth muscle damage from prolonged ischemia
- Hematoma, infection from corporal procedures
- Systemic hypertension from α-adrenergic agents (monitor BP during injection)
Key Takeaways
- Ischemic priapism = urologic emergency; treat within hours to preserve potency
- Phenylephrine is the preferred intracavernous drug (selective α1, minimal cardiac risk)
- Duration determines surgical strategy: <24 h → aspiration/injection; 1–2 days → T-shunt; >2 days → T-shunt + tunneling
- Nonischemic priapism is painless, not urgent, and treated conservatively/with embolization
- Sickle cell disease is the leading secondary cause, especially in children
Sources: Smith & Tanagho's General Urology, 19th ed. | Roberts & Hedges' Clinical Procedures in Emergency Medicine | Campbell-Walsh Wein Urology | Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.